call girls in Connaught Place DELHI 🔝 >༒9540349809 🔝 genuine Escort Service ...
Pericarditis
1.
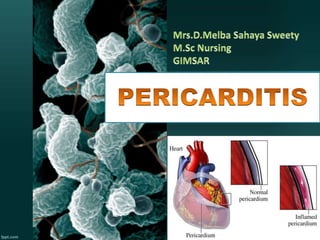
2. The pericardium is a fibroelastic sac made up of visceral
and parietal layers separated by a (potential) space, the
pericardial cavity. In healthy individuals, the pericardial
cavity contains 15 to 50 mL of an ultrafiltrate of plasma.
Pericarditis is swelling and irritation of the pericardium, the
thin saclike membrane surrounding your heart. The sharp
chest pain associated with pericarditis occurs when the
irritated layers of the pericardium rub against each other.
3. Pericarditis is inflammation of the
pericardium (the fibrous sac
surrounding the heart
Pericarditis is inflammation of the
pericardium, a sac-like structure with
two thin layers of tissue that
surround the heart to hold it in place
and help it work.
4. Pericarditis occurs after pericardectomy
in 5 % - 30% patients.
1% - 3 % of cases develop after 10 days to 2
months after acute myocardial infarction.
In the developed world, viruses are
believed to be the cause of about 85% of
cases.
In the developing world tuberculosis is a
common cause but it is rare in the
developed world.
6. C. Mycoplasma
D. Fungal - Histoplasmosis, aspergillosis,
blastomycosis, coccidiodomycosis,
actinomycosis, nocardia, candida
E. Parasitic - Echinococcus, amebiasis,
toxoplasmosis
F. Infective endocarditis with valve ring
abscess
7. 3. Neoplasm
A. Metastatic – Lung or breast cancer,
Hodgkin's disease, leukemia, melanoma
B. Primary – Rhabdomyosarcoma,
teratoma,fibroma, lipoma, leiomyoma,
angioma
C. Paraneoplasm
8. 4. Cardiac
A. Early infarction
pericarditis
B. Late postcardiac injury
syndrome (Dressler's
syndrome)
C. Myocarditis
D. Dissecting aortic
aneurysm
9. 5.Autoimmune
A. Rheumatic diseases – Including lupus,
rheumatoid arthritis, vasculitis, scleroderma,
mixed connective disease
B. Other – Granulomatosis with
polyangiitis (Wegener's), polyarteritis
nodosa, sarcoidosis,IBD (Crohn's, ulcerative
colitis), Whipple's Disease, giant cell
arteritis,Behcet's disease,rheumatic fever
10. 6.Drugs
Pericarditis can also develop from a drug-
induced lupus syndrome caused by
medications including procainamide,
hydralazine, methyldopa, isoniazid,
mesalazine, and reserpine.
Doxorubicin: The anthracycline
antineoplastic agents, such as doxorubicin
and cyclophosphamide, have direct cardiac
toxicity and can cause acute pericarditis
11. 6.Drugs
Penicillin : Penicillin and cromolyn sodium,
induce pericarditis through a hypersensitivity
reaction
Methysergide: Methysergide antimigraine
drug belongs to the group of medicines known
as ergot alkaloids. It causes constrictive
pericarditis through mediastinal fibrosis
12. 7. Metabolic
A. Hypothyroidism - Primarily pericardial effusion
B. Uremia
C. Ovarian hyperstimulation syndrome
13. • Trauma
A. Blunt, Penetrating
B. Iatrogenic - Catheter and
pacemaker perforations,
cardiopulmonary resuscitation
• Radiation
14. BASED ON THE SYMPTOMS :-
Acute pericarditis (<6 weeks)
Sub acute pericarditis (6 weeks to 6
months)
Chronic pericarditis (>6 months)
Recurrent pericarditis
15. Constrictive pericarditis
Viral pericarditis
Purulent pericarditis
Tuberculous pericarditis
Radiation Pericarditis
BASED ON THE CAUSES :-
Traumatic pericarditis
Serous pericarditis
Fiberous pericarditis
Hemorrhagic
pericarditis
Adhesive mediastino
pericarditis
16. • Constrictive pericarditis
When the pericarditis is
associated with a
thickening or scarring of
the pericardial layers, this
starts constricting the heart
within the thoracic cavity,
which in turn limits its
effective functioning. This
condition is known as
constrictive pericarditis.
17. • Viral pericarditis
Viruses that cause
pericarditis is known
as viral pericarditis
This kind of
pericarditis is simple
and can be handled
as an outpatient
procedure.
• Tuberculous pericarditis
This condition is also
seen in a very minor
percentage of patients
having pulmonary
tuberculosis. Some of the
developing countries
remain the leading risk
groups of tuberculous
pericarditis.
18. • Purulent or
suppurative
pericarditis :-
It is due to causative
organisms may arise from
direct extension,
hematogenous seeding, or
lymphatic extension, or by
direct introduction during
cardiotomy.
Immunosuppression
facilitates this condition.
19. • Radiation Pericarditis
This type of pericarditis
is caused due to recent
mediastinal radiation at
any time from weeks to
months after the
exposure.
• Traumatic
pericarditis
• Sharp or blunt trauma
causes traumatic
pericarditis. Invasive
cardiac procedures also
may give rise to this type
of pericarditis, which
includes cardiac
diagnostic catheterization
and electrophysiological
ablation procedure.
20. • Serous
pericarditis
Is usually caused by
noninfectious
inflammation such
as occurs in
rheumatoid arthritis
and systemic lupus
erythematosus .
21. • Fibrous and serofibrinous
pericarditis
• Itrepresent the same basic
process and are the most
frequent type of pericarditis.
Common causes include acute
myocardial infarction (MI),
postinfarction (including
Dressler syndrome), uremia,
radiation and trauma
22. • Hemorrhagic pericarditis
It involves blood mixed with a fibrinous or
suppurative effusion, and it is most
commonly caused by tuberculosis or direct
neoplastic invasion. This condition can also
occur in severe bacterial infections.
Hemorrhagic pericarditis is common after
cardiac surgery and may cause tamponade.
The clinical significance is similar to
suppurative pericarditis
23. • Chronic pericarditis Adhesive
mediastino pericarditis
• Is a reaction that usually follows suppurative
or caseous pericarditis, cardiac surgery, or
irradiation. This condition is rarely caused
by a simple fibrinous exudate. The
pericardial potential space is obliterated, and
adhesion of the external surface of the
parietal layer to surrounding structures
occurs.
24. when microbes are inhaled or ingested, they migrate to
myocardium and cause inflammation
Accumulation of fluid in the pericardial sac called pericardial
effusion.
Compression of the heart
Increased Intra Pericardial pressure
Decreased ventricular filling and emptying
Increased venous
pressure
Decreased cardiac
output
Decreased Arterial
pressure
Cardiac Failure
25. Chest pain beneath the clavicle,
in the neck region worsens with
deep inspiration, relieved with
sitting or leaning forward.It is the
cardinal sign of pericarditis
Mild fever, chills and night
sweats.
Malaise, myalgia
Dyspnea due to constriction or
cardiac tamponade
Palpitation
26. Ewart sign: Ewart's sign is a set of
findings on physical examination in people
with large collections of fluid around their
heart (pericardial effusions).Dullness to
percussion ("woody" in quality), egophony,
and bronchial breath sounds may be
appreciated at the inferior angle of the left
scapula when the effusion is large enough to
compress the left lower lobe of the lung •
Beck’s triad: falling BP; rising JVP;
27. In Constrictive Pericarditis :
Pedal edema
Hepatomegaly
Ascites
JVD
Kussmaul’s sign
Pericardial knock (early
diastolic sound) heard at the
apex
Usually - no friction rub
28. • History Collection- regarding the
etiological factors
• Physical Examination- check for Ewart’s
sign,pedal dema ,hepatomegaly JVD etc..
• CBC- Increased WBC, ESR, and CRP
• Cardiac Enzymes- increased but not as
much as with MI
• ECG- diffuse St elevation *important to
different from MI changes (acute
pericarditis)
29. • Echo- for heart wall
movement
• Chest X ray- shows
an enlarged heart and
pericardial calcification
• Doppler imaging- to
measure the amount of
blood flow through
your arteries and veins
30. • CT Scan to look for
calcium in the
pericardium, fluid,
inflammation, tumors and
disease of the areas
around the heart. Iodine
dye is used during the test
to get more information
about the inflammation.
• Pericardiocentesis fluid-
determine cause; treat
cardiac tamponade
31. • Cardiac MRI to check for
extra fluid in the pericardium,
pericardial inflammation or
thickening, or compression of
the heart. A contrast agent
called gadolinium is used
during this highly specialized
test.
• Cardiac catheterization
To get information about the
filling pressures in the heart.
This is used to confirm a
diagnosis of constrictive
pericarditis.
32. • Cardiac tamponade
Accumulation of pericardial fluid raises intra-
pericardial pressure, hence poor ventricular
filling and fall in cardiac output.
The drop in blood pressure can cause blurred
vision, nausea, confusion, and weakness.
33. • Pericardial effusion.
• Accumulation of fluid in the
pericardial sac. may have
symptoms such as:Chest pain
or discomfort, Enlargement
of the veins of the
neck,Fainting,Fast
breathing, Increased heart
rate,Nausea,Pain in the right
upper abdomen,Shortness of
breath,Swelling in the arms
and legs
34. • Chronic effusive
pericarditis It is an
uncommon pericardial
syndrome characterized by
concomitant tamponade,
caused by
tense pericardial effusion,
and constriction, caused by
thevisceral pericardium. th
e symptoms are chest pain,
lightheadedness, hiccups,
and shortness of breath.
35. • ASA or tylenol Acetaminophen decreases fever and pain ,
but does not help inflammation.Adult dosing is 2 regular
strength (325 mg) every 4 hours or 2 extra-strength (500 mg)
every 6 hours. Maximum dose is 4,000 mg per day.
• Aspirin or NSAIDs are recommended as first-line therapy
for acute pericarditis with gastroprotection. Commonly used
NSAID regimens include : Ibuprofen — Depending on the
severity of the pericarditis and individual medication
response, a dose of 400 to 800 mg of ibuprofen three times
daily is usually adequate for symptom relief. Ibuprofen can
be the preferred NSAID because of its rare side effects,
favorable impact on coronary artery blood flow, and large
36. • Aspirin — Aspirin can be given at a dose of 750 to 1000
mg every six to eight hours followed by gradual tapering
every week for a treatment period of three to four weeks.
• Corticosteroids Corticosteroids are strong medications
that fight inflammation. Your doctor may prescribe a
corticosteroid such as prednisone if your symptoms don't
get better with other medications, or if symptoms keep
returning.
• Colchicine anti-inflammatory agent It is recommended as
first-line therapy for acute pericarditis as an adjunct to
aspirin/NSAID therapy. You should not take this drug if
you have liver or kidney disease
37. Indomethacin — Indomethacin (NSAID)can be
administered at a dose of 50 mg three times daily for one to
two weeks followed by slow tapering But commonly it is
not rcommended due to its adverse effects
• Penicillin - for Bacterial infection
• ACE Inhibitors - relax the blood vessels in the heart and
help blood flow more easily •
• Beta-blockers are avoided because it decreases the
strength of ventricular contraction (have a negative
inotropic effect)
38. • Anticongestive measures such as
diuretics And Inotropics agents
(Inotrtropic agents such as milrinone,
digoxin, dopamine, and dobutamine are
used to increase the force of cardiac
contractions.)
• Anti-anxiety medication (Alprazolam
Diazepam ,Estazolam ,Flurazepam )
• Proton pump inhibitors (Omeprazole,
Pantoprazole)
39. • Pericardiocentesis:- is the aspiration of
fluid from the pericardial space that
surrounds the heart.
40. • Pericardial window a small opening
made in the pericardium, may be performed to
allow continuous drainage into the chest
cavity.
41. • Percutaneous balloon
pericardiotomy :- is a procedure done to
drain excess fluid in the sac around the heart.
The procedure uses a long thin tube with
a balloon attached. During PBP, a doctor inserts
a needle through the chest wall and into the
tissue around the heart. Once the needle is inside
the pericardium, the doctor removes it and
replaces it with a long, thin tube called a
catheter. This tube has an inflatable balloon at
its tip. Repeated inflation of the balloon creates
a small hole or “window” in the pericardium.
When the hole is large enough, the doctor
removes the catheter and balloon replaces them
with a new catheter for final draining. This
allows fluid to drain out of the pericardium,
which improves heart function.
42. Percardiectomy may be
necessary to release both ventricles
from the constrictive and
restrictive inflammation and
scarring Pericardiectomy is
performed through a median
sternotomy, an incision through
the breastbone (sternum) in the
middle front part of the ribs that
allows the surgeon to reach the
heart. The surgeon will remove the
pericardium from the heart, wire
the breastbone and ribs back
together and close the incision
with stitches.
43. • Collaboration of oxygen and delivery of
analgesic drugs and drug side effects
observed.
• Observation of vital signs.
• Perform 12 lead ECG, 24 lead if necessary
• Bed rest with Fowler position / semi-
Fowler position client with pillows.
Positioning/sit up/lean forward
• Instruct client to deep breathe or use
incentive spirometery every 1 - 2 hours
44. • Monitor urine output
• Prevent complications of immobility
• Psychological support
• Monitor the drainage of pericardial fluid
• Manage the anxiety of the client
• Provide health teaching regarding the
disease condition and its treatment
process
45. Ineffective Breathing Pattern related to
inflammatory process and decreased lung capacity
as evidenced by dyspnea,shortness of breath
Acute pain related to tissue ischemia secondary to
arterial occlusion, tissue inflammation as
evidenced by patient facial expression, forward
leaning posture,patient compaint for sharp chest
pain
Impaired thermoregulation , hyperthermia, related
to infection and inflammation as evidenced by
Raised temperature
46. Ineffective tissue perfusion related to decrease
blood flow as evidenced but delayed capillary
refilling,pale mucous membrane
Activity Intolerance related to imbalance
between oxygen supply and metabolic as
manifested by fatigue,decreased activity of
daily living
Anxiety related to therapeutic interventions and
uncertainty of prognosis as manifested by
Facial flushing , Restlessness , Voice quivering
47. Risk for Decreased Cardiac Output
related to structural abnormalities of
the heart
Risk for cardiogenic shock related to
decreased cardiac output.