Reduction in Reintervention for Retained Blood and Post Operative Atrial Fibrilation
•
1 j'aime•238 vues

A recently published study highlighted the fact that 36% of chest tubes clog after cardiac surgery. The following poster, presented at the 11th Annual Cardiovascular-Thoracic Critical Care Conference delves further into rates of Retained Blood Syndrome (RBS) resulting from clogged chest tubes. Phase 0 using standard chest tubes resulted in 20% incidence of RBS. After implementation of Active Clearance Technology the rate decreased by 42%. An additional benefit of using the Active Clearance Technology was a reduction of post-operative atrial fibrillation by 30%! Click on the poster to learn more about the importance of chest tube patency after heart surgery.

Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
Similaire à Reduction in Reintervention for Retained Blood and Post Operative Atrial Fibrilation
Similaire à Reduction in Reintervention for Retained Blood and Post Operative Atrial Fibrilation (20)
Plus de clearflow
Plus de clearflow (7)
Dernier
Dernier (20)
Reduction in Reintervention for Retained Blood and Post Operative Atrial Fibrilation
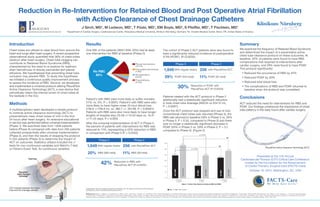
- 1. PleuraFlow Active Clearance Technology (ACT) PleuraFlow® Active Clearance Technology® ACT inserted between the chest tube and the drainage canister. Introduction Chest tubes are utilized to clear blood from around the heart and lungs after heart surgery. A recent prospective observational study quantified that 36% of chest tubes obstruct after heart surgery. Chest tube clogging can contribute to Retained Blood Syndrome (RBS), characterized by the need to re-explore for washout, drain hemothorax or bloody pericardial and pleural effusions. We hypothesized that preventing chest tube occlusion may prevent RBS. To study this hypothesis we initiated a continuous quality improvement process to assess the incidence of RBS. Second, we developed and implemented a universal protocol utilizing PleuraFlow Active Clearance Technology (ACT), a new device that periodically clears the internal lumen of chest tubes at the bedside in the ICU. Methods A multidisciplinary team developed a simple protocol to institute active clearance technology (ACT) to preventatively clear chest tubes of clot in the first 24 hours after heart surgery. An extensive educational in-service was performed before universal implementation (Phase 1). We examined data from 1,849 patients before (Phase 0) compared with data from 256 patients collected prospectively after universal implementation (Phase 2), and then the results of stopping the protocol in 222 patients (Phase 3) to determine the impact of ACT on outcomes. Statistics utilized included the 2 tests for non-continuous variables and Welch’s T-test or Fisher’s Exact Test, for continuous variables. Results One fifth of the patients (360/1,849; 20%) had at least one intervention for RBS at baseline (Phase 0) Patient’s with RBS were more likely to suffer mortality (11% vs. 5%, P < 0.0001). Patient’s with RBS were also more likely to have higher mean 24 hour blood loss (756.6 +/-759.9 mL vs. 480.7 +/- 357.89, P < 0.00001). Patients with RBS were also more likely to have longer lengths of hospital stay (15.59 +/-13.53 days vs. 13.41 +/-11.23 days, P < 0.005) After the universal implementation of ACT in Phase 2, the percent of patients with interventions for RBS was reduced to 11%, representing a 42% reduction in RBS in comparison with Phase 0 (P = 0.0022) The cohort of Phase 2 ACT patients were also found to have a significantly reduced incidence of postoperative A Fib (POAF). (P=0.0033). Patients treated with the ACT protocol in Phase 2 additionally had a statistically significant reduction in total chest tube drainage (469.04 vs 534.12 mL, P = 0.0067). Once the ACT protocol was stopped and use of only conventional chest tubes was resumed (Phase 3), the RBS rate returned to baseline (18% in Phase 3 vs. 20% in Phase 0, P = 0.54, compared to Phase 0) and there was no longer a statistically significant decrease in POAF (24% in Phase 3 vs. 29% in Phase 0, P = 0.1, compared to Phase 0). (Figure 2) Summary We examined the frequency of Retained Blood Syndrome and determined the impact of a preventative active chest tube clearance protocol on these outcomes. At baseline, 20% of patients were found to have RBS complications that required re-interventions after cardiac surgery, and 29% were found to have POAF. This protocol significantly: • Reduced the occurrence of RBS by 42% • Reduced POAF by 30% • Reduced total blood loss • The complications of RBS and POAF returned to baseline when the protocol was completed. Conclusions ACT reduced the need for interventions for RBS and POAF. Our findings underscore the importance of chest tube patency in the early hours after cardiac surgery. References Shalli, S., Saeed, D., Fukamachi, K., Gillinov, A.M., Cohn, W.E., Perrault, L.P., and Boyle, E.M. Chest tube selection in cardiac and thoracic surgery: a survey of chest tube-related complications and their management. J Card Surg. 2009; 24:503-509. Karimov, J.H., Gillinov, A. M., Schenck, L., Cook, M., Kosty Sweeney, D., Boyle, E.M., Fukamachi, K. Incidence of chest tube clogging after cardiac surgery: A single-center prospective observational study. Eur J Cardiothorac Surg. 2013; 44:1029-1036. Shalli, S., Boyle, E.M., Saeed, D., Fukamachi, K., Cohn, W.E., and Gillinov, A.M. 2010. The active tube clearance system: a novel bedside chest-tube clearance device. Innovations (Phila). 2010; 5:42-47. Perrault, L.P., Pellerin, M., Carrier, M., Cartier, R., Bouchard, D., Demers, P., and Boyle, E.M. The PleuraFlow Active Chest Tube Clearance System: Initial Clinical Experience in Adult Cardiac Surgery. Innovations (Phila). 2012; 7:354-358. Presented at the 11th Annual Cardiovascular-Thoracic (CVT) Critical Care Conference, hosted by the Foundation for the Advancement of Cardio-Thoracic Surgical Care (FACTS-Care) October 10, 2014, Washington, DC, USA Supported In part by a research grant from ClearFlow, Inc. Dr. Boyle is a Founder and Consultant for ClearFlow, which manufactures PleuraFlow ACT. Reduction in Re-Interventions for Retained Blood and Post Operative Atrial Fibrillation with Active Clearance of Chest Drainage Catheters J Sirch, MD1 , M Ledwon, MD1 , T Püski, MD1 , EM Boyle, MD2 , S Pfeiffer, MD1 , T Fischlein, MD1 1 Department of Cardiac Surgery, Cardiovascular Center, Paracelsus Medical University, Klinikum Nürnberg, Germany 2 St. Charles Medical Center, Bend, OR, United States of America Phase 0 Phase 2 1,849 With regular drains 256 with PleuraFlow ACT 20% RBS (360 total) 11% RBS (29 total) 42% Reduction in RBS with PleuraFlow ACT (P=0.0022) Phase 0 Phase 2 1,849 With regular drains 256 with PleuraFlow ACT 29% POAF (543 total) 11% POAF (52 total) 30% Reduction in POAF with PleuraFlow ACT (P=0.0033) Pleural Interventions (12.7%) Pericardial Interventions (1.9%) Re-exploration (3.6%) Pneumothorax (3.2%) No RBC 80%