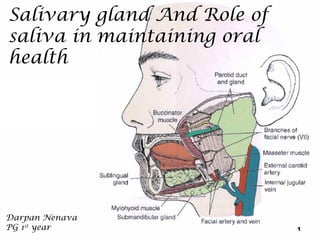
3. Introduction
Salivary glands are group of compound exocrine glands secreting
saliva.
Parenchymal elements consists of terminal secretory units leading
into ducts.
Connective tissue forms a capsule around a gland, and extend into it
dividing groups of secretory units & ducts into lobes & lobules.
Tubulo acinar units are merocrine
3
4. Introduction
Salivary Gland is any cell or organ
discharging a secretion into the oral
cavity.
Major and minor Salivary Glands
Major (Paired)
Parotid
Submandibular
Sublingual
Minor
Those in the Tongue,
Palatine Tonsil, Palate,
Lips and Cheeks
4
6. Parotid Gland
Largest
Average Wt - 25gm
Irregular lobulated mass lying
mainly below the external acoustic
meatus between mandible and
sternomastoid.
On the surface of the masseter,
small detached part lies b/w
zygomatic arch and parotid ductaccessory parotid gland or ‘socia
parotidis’
6
7. Parotid Capsule
Derived from investing layer of deep cervical fascia.
Superficial lamina-thick, closely adherent-sends fibrous septa
into the gland.
Deep lamina-thin- attached to styloid process,mandible and
tympanic plate.
Stylomandibular ligament.
7
8. External Features
Resembles an inverted 3
sided pyramid
Four surfaces
Superior(Base of the
Pyramid)
Superficial
Anteromedial
Posteromedial
Separated by three borders
Anterior
Posterior
Medial
8
9.
Superior Surface
Relations
Concave
Related to
Cartilaginous part of ext
acoustic meatus
Post. Aspect of
temperomandibular
joint
Auriculotemporal
Nerve
Sup. Temporal vessels
Apex
Overlaps posterior belly of
digastric and adjoining part of
carotid triangle
9
10.
Superficial Surface
Covered
by
Skin
Superficial fascia containing facial
branches of great auricular N
Superficial parotid lymph nodes and post
fibers of platysma
Anteromedial Surface
Grooved
by posterior border of
ramus of mandible
Related to
Masseter
Lateral Surface of temperomandibular
joint
Medial pterygoid muscles
Emerging branches of Facial N
10
11.
Posteromedial Surface
Related
to mastoid process with
sternomastoid and posterior
belly of digastric.
Styloid process with
structures attached to it.
External Carotid A. which
enters the gland through
the surface
Internal Carotid A. which
lies deep to styloid process
11
12. Borders
Anterior border
Separates
superficial surface
from anteromedial surface.
Structures
border
which emerge at this
Parotid
Duct
Terminal Branches of
facial nerve
Transverse facial vessels
12
13.
Posterior Border
Separates
superficial surface
from posteromedial surface
Overlaps sternomastoid
Medial Border
Separates
anteromedial
surface from posteromedial
surface
Related to lateral wall of
pharynx
13
14. Structures within
Parotid Gland
tempora
l
External
carotid A
Retromandibular Vein
Facial Nerve
Zygomaticotemporal
zygomatic
Facial Nerve
buccal
mandibula
r
cervical
Superficial temporal V
Maxillary V
Post auricular
V
External jugular
Cervicofacial
Superficial temporal A
Maxillary A
P.Auricular A
Common Facial V
14
15.
Facial Nerve trunk lies approximately 1 cm
inferior and 1 cm medial to tragal cartilage pointer
of external acoustic meatus.
15
16. Parotid Duct
Ductus parotideus; Stensen’s duct
5 cm in length
Appears in the anterior border
of the gland
Runs anteriorly and downwards
on the masseter b/w the upper
and lower buccal branches of
facial N.
16
17.
At the anterior border of
masseter it pierces
Buccal pad of fat
Buccopharyngeal fascia
Buccinator Muscle
It opens into the vestibule of
mouth opposite to the 2nd
upper molar
17
18. Surface anatomy of Parotid Duct
Corresponds to middle third of a line drawn from
lower border of tragus to a point midway b/w nasal
ala and upperlabial margin
18
20. Nerve Supply
Parasymapthetic N
Secretomotor via
auriculotemporal N
Symapathetic N
Vasomotor
Delivered from plexus
around the external
carotid artery
Sensory N
Reach through the
Great auricular and
auriculotemporal N
20
21. Clinical Consideration
1.
2.
3.
A viral inflammation of the parotid gland (mumps)
causes it to swell, resulting to pain on movement of
the jaw.
Abcesses or cysts of the gland may result in pressure
to the facial nerve
Stones or calculi in the duct can block it, causing
painful swelling of the gland.
21
22. Submandibular Salivary Glands
It is a mixed serous and mucous secreting
gland.
Irregular in shape
Large superficial and small deeper part
continous with each other around the post.
Border of mylohyoid
Superficial Part
Situated in the digastric triangle
Wedged b/w body of mandible and mylohyoid
3 surfaces
Inferior,Medial,Lateral
22
24.
Capsule
Derived
from deep cervical fascia
Superficial
Deep
Layer is attached to base of mandible
layer attached to mylohyoid line of mandible
24
25.
Relations
Inferior- covered by
Skin
Supeficial fascia containing
platysma and cervical
branches of facial N
Deep Fascia
Facial Vein
Submandibular Nodes
Lateral surface
Related to submandibluar
fossa on the mandible
Madibular attachment of
Medial pterygoid
Facial Artery
25
26.
Medial surface
Anterior part is related to myelohyoid
muscle,nerve and vessles
Middle partHyoglossus,styloglossus,lingual nerve,
submandibular ganglion,hypoglossal
nerve and deep lingual vein.
Posterior Part-Styloglossus,stylohyoid
ligament,9th nerve and wall of pharynx
26
27.
Deep part
Small in size
Lies deep to mylohyoid
and superficial to
hyoglossus and
styloglossus
Posteriorly continuous
with superficial part
around the posterior
border of mylohyoid
27
28. Submandibluar
duct
Whartons duct
5 cm long
Emerges at the anterior end of deep
part of the gland
Runs forwards on hyoglossus b/w
lingual and hypoglossal N
At the ant. Border of hyoglossus it is
crossed by lingual nerve
Opens in the floor of mouth at the side
of frenulum of tongue
28
30. Blood Supply
Arteries
Branches
of facial and
lingual arteries
Veins
Drains
to the
corresponding veins
Lymphatics
Deep
Cervical Nodes via
submandibular nodes
30
31. Nerve
Supply
Branches
from
submandibular ganglion,
through which it receives
Parasymapthetic fibers
from chorda tympani
Sensory fibers from lingual
branch of mandibular
nerve
Sympathetic fibers from
plexus on facial A
31
32. Sublingual Salivary Glands
smallest of the three glands
weighs nearly 3-4 gm
Lies beneath the oral mucosa
in contact with the sublingual
fossa on lingual aspect of
mandible.
32
33.
Relations
Above
Mucosa of oral floor,
raised as sublingual fold
Below
Myelohyoid Infront
Anterior end of its fellow
Behind
Deep part of
Submandibular gland
33
34. Lateral
Mandible
above the
anterior part of
mylohyoid line
Medial
Genioglossus
and
separated from it by
lingual nerve and
submandibular duct
34
35.
Duct
Ducts of Rivinus
8-20 ducts
Most of them open directly into the
floor of mouth
Few of them join the submandibular
duct
35
36.
Blood supply
Arterial from sublingual and submental arteries
Venous drainage corresponds to the arteries
Nerve Supply
Similar to that of submandibular glands( via lingual nerve ,
chorda tympani and sympathetic fibers)
36
37.
Minor salivary glands are found throughout the
mouth:
– Lips
– Buccal mucosa (cheeks)
– Alveolar mucosa (palate)
– Tongue dorsum and ventrum
– Floor of the mouth
Together, they play a large role in salivary
production.
37
49.
Myoepithelial cells
Present in relation to alveoli and
intercalated ducts
Those on the alveoli are
branched-’Basket Cells’
Those on the ducts are fusiform
Contractile cells helps to squeeze
out secretions from alveoli
49
51.
Main function of Salivary
Gland-secretion of saliva
Daily secretion -800 to
1500 ml
pH : 6-7
51
52. Control of Salivary Secretion
Sup Salivatory Nu
Facial N
Otic Ganglion
Inf Salivatroy Nu
Parotid Gland
Chorda tympani N
Submandibular G
Under neural control
Mainly by parasympathetic signals from
Sup & Inf salivatory nuclei
52
53.
Parasympathetic stimulationprofuse secretion of watery saliva
Sympathetic stimulationscanty viscid secretion
Sympathetic supply comes from cervical
sympathetic chain along the blood vessels
53
54.
Salivatory nuclei are excited by
Taste and tactile stimuli from tongue
and other areas of mouth and
pharynx
Stimuli from esophagus and stomach
(due to stimulation of vagal afferent
fibers)
(unconditioned reflex)
Stimuli arising from higher centers
of brain due to sight, smell or
thought of food
(conditioned reflex).
54
Pavlov with his dog
56.
Complex fluid found lubricating the mucosa and teeth of the oral
cavity.
Salivary glands, their cells and ducts are greatly responsible for
the modification and kind of saliva being secreted
It is of three types:
Serous Saliva
Mucous Saliva
Mixed Saliva
56
57.
General characteristics:
Consistency - slightly cloudy due to presence of mucins and cells
Reaction - usually slightly acidic (pH 6.02-7.05).On standing or boiling, it
loses CO2 and becomes alkaline.
Specific gravity - 1.002-1.012
Freezing point - 0.07-0.34° Celsius
57
59. Unstimulated flow
Resting salivary flow―no external stimulus
o Typically 0.2 mL – 0.3 mL per minute
o Less than 0.1 mL per minute means the person has
hyposalivation
Hyposalivation – not producing enough saliva
59
60. Stimulated Flow
Response to a stimulus, usually taste, chewing, or
medication eg, at mealtime
o Typically 1.5 mL – 2 mL per minute
o Less than 0.7 mL per minute is considered hyposalivation
60
61. The average person produces approximately 0.5 L – 1.5 L per day
• Salivary flow peaks in the afternoon
• Salivary flow decreases at night.
• There is a difference in the quality between stimulated and
unstimulated saliva
61
62. Ions and salivary flow
As saliva passes
through the salivary
ducts, cations
(sodium and chloride)
are reabsorbed into
the adjacent
blood vessels.
62
63. As saliva passes through the salivary ducts, cations
(sodium and chloride) are reabsorbed into the adjacent
blood vessels. In exchange, bicarbonates and
potassium are transferred from the blood
63
64. Stimulated Salivary Flow
• Saliva passes through the salivary duct very rapidly
o It impedes the exchange of sodium and chloride for
potassium and bicarbonate
Unstimulated Salivary Flow
• Has a high content of potassium and bicarbonate
o The quality of unstimulated saliva will change when flow
increases because of a stimulus (chewing gum, thinking about
lemons, looking at a food you crave)
64
66.
Ionic Composition
Saliva
in the acini-isotonic with plasma
Under
resting condition ionic composition of saliva reaching
the mouth
During
Na+ and Cl- 15 mEq/l (1/7 to 1/10 conc of Plasma)
K+ 30 mEq/l (7 times that of Plasma)
HCO3- 50-70 mEq/l (2-3 times that of plasma)
maximal salivation
Na+ and Cl- (1/2 to 2/3 conc of Plasma)
K+ (4 times that of Plasma)
HCO3- 50-70 mEq/l (2-3 times that of plasma)
66
67. Functions of Saliva
Main function: maintaining the well-being of the mouth
Other important functions:
Protection
Buffering Action
Digestion
Facilitation of Taste
Defensive Action against Microbes
Ionic Exchange between Tooth Surface
67
68. Functions of Saliva
Effect
Active Constituent
Protection
Lubrication, lavage, pellicle
formation
Glycoprotein
Water
Buffering Action
Regulates pH
Phosphate and
Bicarbonate
Digestion
Digests starch
Digests lipids
Bolus formation
Amylase
Lingual Lipase
Facilitation of Taste
Taste bud growth and
maturation, dissolves
substances to carry to taste
buds
Gustin
Defensive Action Against
Microbes
Antibodies
Hostile Environment
Lysozyme
Lactoferrin
IgA
Ionic Exchange Between
Tooth Surface
Posteruptive Maturation of
Enamel
Repair
Calcium
Phosphate
68
69. Saliva and Dental Caries
Effect of desalivation and hyposalivation on dental caries
Salivary clearance from oral cavity
Flouride concentration of saliva
Salivary antibacterial substance
Protein inhibiting hydroxyapatite
Acquired salivary pellicle
69
70. Effect of desalivation and hyposalivation on dental caries
Total or partial aplasia is rare and accompanied by high caries
prevalence
Causes
Tumor growth
Radiation therapy
This condition is called as XEROSTOMIA
Reduced salivary secretion is called as HYPOSALIVATION
Causes
Drugs such as atropine and other anticholinergics
Fever or prolonged diarrhea
Diabetes
Anemia
Hypovitaminosis A or B
Uremia
Dehydrating disease of old age
70
71.
Patients with hyposalivation experience
Difficulty in mastication
Swallowing
Wearing dentures
Speaking
Sjogren’s syndrome is an autoimmune
Acinar cells are destroyed
Dry eyes as lacrimal gland cells are also destroyed
And symptoms of rheumatoid arthritis
71
72. Salivary clearance from oral cavity
Role of bacteria and food debris removal from oral
cavity
Bacteria
Bacteria is passed into stomach by salivary flow
Half life of any material in cavity is only few minutes
Despite
continuous flow dental plaque can accumulate at
rapid rate of 10-20mg/day
Rate of plaque accumulation is even more rapid in patients
with hyposalivation and xerostomia
72
73.
Food Debris
When retained in mouth act as substrate for metabolic
activities of microbes
Thus if clearance is retarded it will tend to promote the
development of caries
Caramel and other toffees show prolonged retention
Some studies show cariogenecity is not related to sugar
concentration
Sugar in non retentive forms as in soft drinks
73
74. Flouride concentration of saliva
The level of flouride ions in ductal saliva is as low as 0.010.03ppm.
Flouride level in saliva are independent of salivary flow rate and
determined by the amount ingested
Fluorapatite
Insoluble in saliva
Therefore beneficial to have high proportion of fluorapatite in surface
enamel as possible
Higher stable concentration of fluoride can accure slowly from saliva
But can be reached more rapidly by topical flourde applications
74
75. Flouride concentration of saliva
The importance of fluoride maintenance and augmentation of
fluoride in enamel surface
As the fluoride concentration is reduced protection against caries is also
decreased
75
76. Salivary antibacterial substance
A number of anti bacterial factors present in saliva
Lysozymes
Lactoperoxidase
Lactoferrin
Immunoglobulin A
It helps to prevent the establishment of more pathogenic
transient invaders
76
77. Lysozymes
Have property of cleaving cell walls of microbes causing there
lysis
Antibacterial action of lysozyme does not completely depend on
cell lysis
(Streptococcus mutans lose there viability in the presence of lysozyme
and some detergent or NaCl without lysis of cell wall
77
78. Lactoperoxidase
This factor exists in milk, saliva and tears and can inhibit the
growth and acid formation of some bacteria.
It oxidises thiocyanate (SCN-) in presence of hydrogen peroxide
Formed by microbes in hypothiocyanate(OSCN-)
To oxidize thiol group which leads to activation of many
bacterial enzymes
78
79. Lactoferrin
Bacteriocidal effects due to its strong iron binding capacity
Removing iron from solution and making it unavailable as an
essential bacterial nutrient
Lactoferrin has been shown to be antagonist to S.mutans
79
80. Immunoglobulins
There are two principal immunological mechanism involved in
protection against infectious diseases
Antibodies production (humoral immunity)
Involving cells (cell-mediated immunity)
Antibodies produced by plasma cells circulate in body (systemic immunity)
If produced by plasma cells with secretory tissues such as salivary gland (local
immunity)
Antibodies are
IgG
IgA
IgD
IgE
IgM
80
81. Immunoglobulins
In systemic circulation IgG dominates
In saliva IgA dominates in S-IgA form Secretory
Immunoglobulin A
Concentration of IgA in stimulated parotid and submandibular
saliva is 4mg/100ml
30mg/100ml in secretion from minor salivary glands
81
82. Protein inhibiting hydroxyapatite
Several salivary protein bind calcium and /or inhibit formation
of hydrooxyapatite these proteins are
Statherin
Proline-Rich Proteins
82
83. Protein inhibiting hydroxyapatite
Statherin
A polypeptide
Concentration in saliva 2-6 µM
Also prevents precipitation of calcium phosphate from supersaturated
solution by adsorbing onto early crystal nuclei
Causing demineralization of early carious lesion
Inhibition is due to the ability of the statherin to block crystal growth of
calcium phosphate
83
84. Protein inhibiting hydroxyapatite
Proline-Rich Proteins
A polypeptide
Concentration in saliva 2-6 µM
Also prevents precipitation of calcium phosphate from supersaturated
solution by adsorbing onto early crystal nuclei
Causing demineralization of early carious lesion
Inhibition is due to the ability of the statherin to block crystal growth of
calcium phosphate
84
86. Acquired salivary pellicle
Clinical relevance
Pellicle thickness
To prevent the contact of saliva prior to composite resin placement
Upon the etched enamel
Salivary protein tend to fill up defects in newly etched enamel
100nm after 2 hrs to about 400nm in 24-48 hrs
Pellicle is three layered
Subsurface :- has dendritic appearance penetrate in pores and
demineralized enamel
Centre :- uniformly forms a surface around tooth
Suprastructure :- variable thickness
86
87. Acquired salivary pellicle
This is predominantly bacteria free initially
Becomes highly insoluble with time due to protein denaturation
Coating becomes rapidly populated by mixed bacterial
aggregrates
Grow in number and coalesce to form bacterial dental plaque
87
88. Properties of salivary pellicle
Act as a lubricant prevent premature loss of enamel during
mastication
Reduces rate of demineralization of tooth surface by acidic food
and drinks
Act as a semi permeable membrane and reduces ion mobility
but the movement of water is unaffected.
Reduces mobility of calcium and phosphate from enamel to
fluid enviorment
Forms a surface for bacterial colonization leads to formation of
microbial dental plaque
Prevents continuous enlargement of tooth surface by crystal
growth of hydroxyapatite crystal
88
91. Reflex Activity
Resting flow: keeps the mouth and oropharynx moist
Food and the prospect of eating: are most saliva-inducing stimuli
Whole-mouth saliva contribution when stimulated:
Parotid gland: 50%
Submandibular gland: 30%
Sublingual and minor salivary glands: 20%
91
93. Reflexes
Visual and psychic salivary reflex
Stimuli:
thought and sight of food
Esophageal-salivary reflex
Waterbrush
phenomenon: sudden filling of the mouth with
fluids
93
95. Age Changes
the aging salivary glands are known to undergo
structural changes
The lobule structure becomes less ordered
The acini vary more in size and eventually atrophy
Interlobular ducts become more prominent and the
percentage of fibroadipose tissue increases
95
96. Age Changes
Changes in the salivary glands
(submandibular,parotid (less) and minor salivary
glands)
Shrinkage
of cells
Dilation of ducts
Oncocytic transformation
Increased adiposity
Fibrosis
Focal microcalcifications with obstruction
Chronic inflammation
96
98. Mucoceles
CAUSE: trauma to excretory ducts of the minor glands which
allows the spillage of mucus into the surrounding connective
tissue
PHYSIOLOGIC MANIFESTATION: formation of painless,
smooth surfaced, bluish lesions
TREATMENT:
self-limiting (acute) or
surgery (chronic)
98
100. Ranulas
Type of mucocele
CAUSE: blocked sublingual gland ducts
PHYSIOLOGIC MANIFESTATION: Unilateral, softtissue lesions, often with a bluish appearance.
Vary in size and may cross the midline of the mouth and cause
deviation of the tongue
TREATMENT:
self-limiting (acute)
surgery (chronic)
100
102. Sialolithiasis
CAUSE: inactivity of the glands
Metabolic conditions that promote salt precipitation in the glands
Predisposing factors: dehydration and poor oral hygiene
PHYSIOLOGIC MANIFESTATION: formation of caliculi
TREATMENT: massaged out by a specialist, surgery,
antibiotics
102
106. Mumps
Aka. epidemic parotitis (viral)
Occurs usually during childhood
CAUSE: paramyxovirus that infects the parotid glands
PHYSIOLOGIC MANIFESTATION: inflammation of the
parotid glands located on either side of the face
TREATMENT: warm compress,
warm, salt water rinses, antibiotics,
surgery, anti-inflammatory
medications
106
110. Irradiation Reaction (Xerostomia)
subjective complaint of dry mouth due to a lack of saliva
CAUSE: tumoricidal doses of ionizing radiation, excessive
clearance or breathing through the mouth, hyposalivation
(decreased saliva production)
PHYSIOLOGIC MANIFESTATION: dry oral mucosa
TREATMENT: frequent sips of water and frequent mouth
care
110
As saliva passes through the salivary ducts, cations (sodium and chloride) are reabsorbed into the adjacent blood vessels.
In exchange, the body releases bicarbonates and potassium.
Stimulated salivary flow causes rapid passage through the salivary duct and thus impedes the exchange of sodium and chloride for potassium and bicarbonate.
Unstimulated salivary flow is slower and thus has a high content of potassium and bicarbonate.
The quality of unstimulated saliva will change when flow increases because of a stimulus (chewing gum, thinking about lemons, looking at a food you crave).
Automatic, and predictable responses to stimuli.
Dependent on reflex activity .
Vary depending on the stimuli.
Sour: evokes the greatest salivary response.
Chew on the right side of the mouth- inc. in salivary response from the right parotid
Story of Pavlov and the Dog.
No significant evidence. When hungry, we become more aware of the presence of saliva in our mouth.
Trauma during tooth extraction or spicy food.
Experienced when one gets heartburn or the feeling of nausea. Believed to be due to the high levels of acidity in the esophagus.