2. Sinoatrial Block
• the impulse from the sinus node is blocked before
it enters the atrial muscle
• sudden cessation of P waves, with resultant
standstill of the atria.
• the ventricles pick up a new rhythm, the impulse
usually originating spontaneously in the
atrioventricular (A-V) node
• the rate of the ventricular QRS-T complex is slowed
3.
4. Atrioventricular Block
• The only means by which impulses ordinarily can
pass from the atria into the ventricles is through
the A-V bundle, also known as the bundle of His
• 1. Ischemia of the A-V node or A-V bundle fibers
• 2. Compression of the A-V bundle
• 3. Inflammation of the A-V node or A-V bundle
• 4. Extreme stimulation of the heart by the vagus
nerves
5. Incomplete Atrioventricular
Heart Block
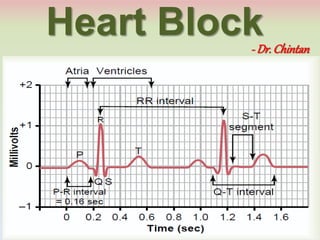
• Prolonged P-R Interval - First Degree Block
• time between beginning of the P wave and
beginning of the QRS complex is about 0.16
second
• P-R interval usually decreases in length with faster
heartbeat and increases with slower heartbeat
• when the P-R interval increases to greater than
0.20 second, the P-R interval is said to be prolonged
6. Incomplete A-V Heart Block
• First degree block is defined as a delay of
conduction from the atria to the ventricles but not
actual blockage of conduction
7. Incomplete A-V Heart Block
• Second Degree Block
• increase the P-R interval to 0.25 to 0.45 second,
• the action potential sometimes is strong enough to
pass through the bundle into the ventricles and
sometimes is not strong enough
• atrial P wave but no QRS-T wave, and it is said that
there are “dropped beats” of the ventricles
• “2:1 rhythm”, 3:2 or 3:1
8.
9. Complete A-V Block
• Third Degree Block
• ventricles spontaneously establish their own signal,
usually originating in the A-V node or A-V bundle
• P waves become dissociated from the QRS-T
complexes
• rate of rhythm of the atria in ECG is about 100 beats
per minute, whereas the rate of ventricular beat is less
than 40 per minute
• Ventricles have “escaped” from control by the atria
12. Incomplete Intraventricular
Block
• electrical alternans
• Tachycardia
• when the rate of the heart is rapid, it is impossible
for some portions of the Purkinje system to
recover from the previous refractory period quickly
enough to respond
• ischemia, myocarditis or digitalis toxicity
13.
14. Grading of exercise
WHO grading of muscular exercise:
VO2 Max: Maximum amount of O2 that can be
consumed during a severe exercise.
Resting VO2 ( O2 consumption ) = 250 ml/min.
Grade HR (bpm) O2 consumption
(L/min)
RLI MET
i. Light (mild) < 100 0.4 – 0.8 < 25 < 3
ii. Moderate 100 - 125 0.8 – 1.6 25 - 50 3.1 – 4.5
iii. Heavy 125 - 150 1.6 – 2.4 51 - 75 4.6 - 7
iv. Severe > 150 > 2.4 > 75 > 7
15. Causes of ↑ HR during exercise
(1) Increased sympathetic activity – anticipatory
tachycardia.
(2) Decrease in Vagal tone.
(3) Increased activity of the limbic system and motor
cortex due to psychic stimuli directly acting on
medulla – anticipatory tachycardia.
(4) Increased Peripheral reflexes originating from
(i) Muscle spindle
(ii) Muscle tendon receptors
(iii) Joint receptors
(iv) Organ of Corti
16. Causes of ↑ HR during exercise
(5) Liberation of hormones into circulation (Centrally
acting)
(i) Catecholamines from Adrenal Medulla
(ii) Thyroxin (T4) from thyroid gland in response to stress
(6) Increase in body temperature
(7) Chemical changes occurring in the blood
Hypoxia - arterial PO2
Hypercapnia - arterial PCO2
Lactic Acidosis - pH