
Recommandé
Contenu connexe
Tendances
Tendances (20)
Similaire à Megaloblastic Anemias: Causes and Treatment
Similaire à Megaloblastic Anemias: Causes and Treatment (20)
Dernier
Dernier (20)
Megaloblastic Anemias: Causes and Treatment
- 1. Megaloblastic Anemias BY DR IMRAN SULTAN
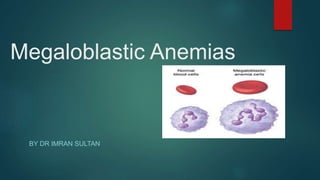
- 2. Concept Megaloblastic Anemias are group of disorders characterised by distinctive morphological appearances(large cells with an arrest in nuclear maturation) of the developing red cells of the bone marrow. Nuclear maturation is immature relative to cytoplasmic maturity ,hence cells can be seen in BM aspirates and in peripheral smears have been called megaloblasts. Mc causes are vit B12 and folate deficiency,they may occur bcoz of genetic or acquired abnormalities that affect the metabolism of these vitamins or bcoz of defects in DNA synthesis NOT related to cobalamin or folate.
- 3. Causes of megaloblastic anemia Cobalamin def. or abnormalities on cobalamin metabolism. Folate deficiency or abnormalities of folate metabolim. Therapy with anti-folate drugs (eg,methotrexate). Causes independent of either folate or cobalamin and refractory to cobalamin and folate therapy. Some cases of acute myeloid luekemia,myelodysplasia. Therapy with drugs interfering with synthesis of DNA(cytosine arabinoside,hydroxyurea,6-MP,AZT). Orotic aciduria(responds to uridine). Thiamine-responsive .
- 4. Cobalamin (vitamin B12) In nature mainly in 2-deoxyadenosyl (ado) form that is cofactor for enzyme methylmalonyl coenzyme A mutase and other is methylcobalamin in human plasma and in cell cytoplasm that is a cofactor for methionine synthase. It is solely synthesized by microorganisms and the only source for humans is food of animal origin like meat, fish and dairy products. Adult daily losses (mainly in urine and feces) are 1-3 ug and as body doesnot have the ability to degrade body store, so daily requirements are also 1-3 ug. Body stores are of the order of 2-3 mg, sufficient for 3-4 years if supplies are completely cut off. Because of appreciable amount undergoing enterohepatic circulation, cobalimin deficiency develop more rapidly in individuals who malabsorb B12 then it does in vegans, in whom reabsorption of biliary cobalamin is intact.
- 5. Metabolic functions of Vit B12
- 6. C: Cell growth & multiplication. D: Role in folate uptake & storage
- 7. ABSORPTION
- 8. CAUSES OF Sufficiently severe to cause megaloblastic anemia Malaabsorption of B12, not usually sufficiently severe & prolonged to cause anemia
- 9. Pernicious anemia of adults Gastric causes of Cobalamin malabsorption Severe lack of intrinsic factor due to gastric atophy. Man and women ratio is 1:1.6 . Peak age of onset is 60 years and with only 10% patients being < 40 years, blacks indivisuals and latin americans the age of onset generally is lower. Common in north europens but occur in all countries and ethnic groups. The disease occur more commenly than by chance in close relatives and in persons with other orgenic specific autoimmune diseases, e.g. Thyroid disease, vitiligo, hypoparathyrodism and addison’s disease. It also associated with hypogammaglobulinemia, with premature graying or blue eyes and person of blood group A. The serum gastrin level is raised and serum pepsinogen I level are low.
- 10. This usually show atrophy of all layers of the body and fundus with loss of glandular elements, an absence of parietal and chief cells and replacement of mucous cells, a mixed inflammatory cell infiltrate and prehaps intestinal metaplasia. The infiltrate of plasma cells and lymphocyetes contains an excess of CD4 cells. Gastric biopsy; histological features of stomach in pernicious anemia compared to normal
- 11. Juvenile pernicious anemia This occurs in old children and resembles PA of adults. Gastric atrophy, achlorhydria and serum IF antibofies are all present, although parietal cell antibodies are usually absent, About of patients show an associated endocrinopathy such as autoimmune thyroiditis, addison’s disease, or hypoparathyroidism; in some, mucocutaneous candidiasis occurs.
- 12. ABNORMALITIES OF COBALAMIN METABOLISM Congenital Transcobalamin II Deficiency or Abnormality- Infants with TCII deficiency usually present with megaloblastic anemia within a few weeks of birth. Serum cobalamin and folate levels are normal, but the anemia responds to massive (e.g., 1 mg three times weekly) injections of cobalamin. Some cases show neurologic complications. The protein may be present but functionally inert. Genetic abnormalities found include mutations of an intra- exonic cryptic splice site, extensive deletion, single nucleotide deletion, nonsense mutation, and an RNA editing defect. Congenital Methylmalonic Acidemia and Aciduria- Infants with this abnormality are ill from birth with vomiting, failure to thrive, severe metabolic acidosis, ketosis, and mental retardation. Anemia, if present,is normocytic and normoblastic. The condition may be due to a functional defect in either mitochondrial methylmalonyl CoA mutase or its cofactor adocobalamin. Mutations in the methylmalonyl CoA mutase are not responsive, or only poorly responsive, to treatment with cobalamin. Acquired Abnormality of Cobalamin Metabolism: Nitrous Oxide Inhalation Nitrous oxide (N2O) irreversibly oxidizes methylcobalamin to an inactive precursor; this inactivates methionine synthase. Megaloblastic anemia has occurred in patients undergoing prolonged N2O anesthesia
- 13. Folate Folic acid is parent compound of large family of natural folate compounds. Its highest concentration is found in liver, yeast, spinach, other greens and nuts. Folate easily destroyed by heating, particularly in large volumes of water. Total folate in adult is ~10mg with liver containing the largest store. Daily adult requirements are ~10ug and so stores are sufficient for 3-4 months in normal adult and severe folate deficiency may develop rapidly.
- 14. Folates absorption in small intestine & transport Folate polyglutamates Monoglutamates Lumen-mucosa 5-methyl THF Intestinal-mucosa Albumin bound 1/3 unbound 2/3 in plasma Cellular receptors; PCFT/HCPI, Clathrin-coated pits Membrane folate Transporter Cell cytoplasm Plasma,CSF, milk and bile have folate In malabsorption syndrome; due to loss of folate 60-90 ug in bile each day, with folate of sloughed intestinal cells, accelerate speed with which folate deficiency develop in malabsorption conditions.
- 16. Biochemical basis of megaloblastic anemia The folate is needed as coenzyme 5,10-methylene THF polyglutame for conversion of dUMP to dTMP. In deficiencies of folate or cobalamin, there is failure to convert of dUMP to dTMP; precursor of dTTP. The availablity of 5,10-MTHF is reduced in either cobalamin or folate deficiency. in cobalamin deficiency due to failure of formation of THF, the substrate on which folate polyglutame are build, MTHF accumulates in plasma and intracsellular concentration fall; termed as THF starvation or methylfolate trap.
- 17. The role of folates in DNA synthesis and formation of SAM which is involved in methylation reaction
- 18. CLINICAL PRESENTATION HISTORY- FINDINGS TO HELP B12 deficiency Evidence of achlorhydria such as abdominal discomfort,reflux,early satiety. Pernicious anemia:these patients may have signs of other autoimmune ds like thyroid ds,addison ds,or tye 1 DM. Family history HLA(HLA A2,A3,B7,B12) and Type A blood. History of gastrectomy History of megablastosis from childhood-hereditary cause. HISTORY- FINDINGS TO HELP FOLATE deficiency Poor nutriton,excessive heating and dilution of foods. Chronic alcoholism IBD/SPRUE/CELIAC DS. Pregnancy,lactation,hyperthyroidism.exfoliative dermatitis. medications
- 19. Physical examination Evidence of anemia-pallor,if severe patient will dyspnea,tachycardia,cp distress. Glossitis Dermatological signs-hyperpigmentation of skin and abnormal pigmentation of hair due to increased melanin synthesis. Mental changes-from irritability to psychosis. And peripheral neuropathy in both folate and B12 changes. SACD in cobalamin deficiency-Abnormal gait,loss of balance,speech impairment and loss of proprioceptive and vibratory sense. Abdominal scars Pts with non tropical and tropical sprue may have signs of malabsorption,weight loss, abdominal distension,diarrhoea,steatorrhea,.
- 20. Work up Initial workup for megaloblastic anemia should include a complete blood count (CBC), RBC indices, peripheral smear, reticulocyte count, lactate dehydrogenase (LDH), indirect bilirubin, iron and ferritin assays, serum cobalamin and serum folate, and possibly an RBC folate evaluation. LDH-usually markedly increased in severe meg.Anemia. Peripheral blood oval macrocytes usually with anisopoikilocytosis.MCV usually >100 fl Hypersegmented nuetrophils(5% withmore than 5 nuclear lobes and 1% with 6 lobes). Nucleated Rbcs and megaloblasts. Luekopenia but usually >1500 .decreased plt count rarely <40,000. Reticulocyte count low. Bone marrow:usually not needed however can help to rule out myelodysplasia and asess iron stores.
- 21. contd Hypercellular marrow Megaloblastic erythroid hyperplasia Giant metamyelocytes.
- 22. Lab testing for diagnosis Serum B12 Serum Folate MMA Homocysteine Normal >300 >4 70-270 5-14 Deficiency <200 <2 Confirm B12 200-300 High High Confirm folate 2-4 Normal High High amount of seaweed in the diet can interfere with the B12 assay as can a single meal. It is best to add-on tests to blood already in the lab, particularly for inpatients due to the variability of the test. Intrisic factor antibody assay can be falsely positive if pt has recently received a B12 shot with B12 >800, thus important to add-on.
- 23. Schilling Test 1. PART 1: Oral labeled B12 and IM unlabeled B12 at the same time to saturate tissue stores 2. 24h urine to assess absorption >5% normal <5% impaired 3. PART 2: Repeat w/oral IF if now normal =PA if abnormal = malabsorption 4. Can continue with antibiotics to look for bacterial overgrowth, pancreatic enzymes for exocrine insufficiency Part 1 patest result Part 2 test result Diagnosis Normal - Normal or vitamin B12 deficiency Low Normal Pernicious anemia Low Low Malabsorption
- 24. TREATMENT Once drug-induced megaloblastic changes and myelodysplasia-related megaloblastosis have been ruled out, most patients are treated with cobalamin or folate IM B12 1000mcg daily x 1 week then 1000mcg weekly x 1 month Then 1000mcg monthly for life for PA Oral high dose 1-2 mg daily As effective but less reliable than IM Currently only recommended after full parenteral repletion Sublingual, nasal spray and gel formulations available
- 25. Folate Deficiency Treatment Oral folate 5-15mg daily for 4 months or until hematologic recovery Rule out B12 deficiency prior to treament as folic acid will not prevent progression of neurologic manifestations of B12 deficiency Repeat testing for B12 deficiency may be reasonable for those on long-term folic acid therapy if hematologic (macrocytosis or ↑LDH) or neurologic sx persist
- 26. Monitoring response Elevated levels of LDH and indirect bilirubin should fall rapidly. A prolonged elevation of the LDH level indicates a failure of therapy, development of iron deficiency, or an error in diagnosis. Reticulocytosis should be evident within 3-5 days and peaks in 4-10 days. Leukocyte and platelets counts are usually restored to normal within days after therapy has been started, but hypersegmented neutrophils may persist for 10- 14 days. Hemoglobin should rise approximately 1 g/dL each week.normal within 2 months.
- 27. Treatment of Other Related Conditions Blind loop syndrome should be treated with antibiotics. Patients with transcobalamin II (TCII) deficiency may require higher doses of cobalamin. Tropical sprue should be treated with both cobalamin and folate. Acute megaloblastic anemias due to nitrous oxide exposure can be treated with folate and cobalamin. Fish tapeworm infection, pancreatitis, Zollinger -Ellison syndrome, and inborn errors should be treated with appropriate measures.