31. Cellular Mechanisms that Govern Sleep and Wakefulness Brainstem nuclei responsible Neurotransmitter involved Activity state of the brainstem neurons WAKEFULNESS Cholinergic nuclei of pons-midbrain junction Acetylcholine Active Locus coeruleus Norepinephrine Active Raphe nuclei Serotonin Active NON-REM SLEEP Cholinergic nuclei of pons-midbrain junction Acetylcholine Decreased Locus coeruleus Norepinephrine Decreased Raphe nuclei Serotonin Decreased REM SLEEP ON Cholinergic nuclei of pons-midbrain junction Acetylcholine Active (PGO waves) Raphe nuclei Serotonin Inactive REM SLEEP OFF Locus coeruleus Norepinephrine Active
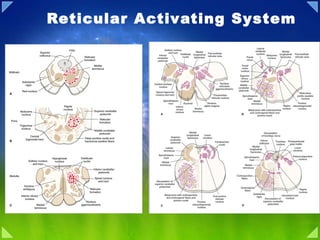
Figure 23-1 Position of the reticular formation in the brainstem. Diagrams illustrate the approximate positions of the reticular formation within the (A) midbrain, (B) pons, and (C) medulla as indicated by the dotted areas. Larger-sized dots represent magnocellular (large-celled regions), and smaller-sized dots represent parvocellular (small-celled regions). IN PRIMITIVE VERTEBRATES—reptiles, amphibians, and fish—the forebrain is only a small part of the brain. It is devoted mainly to olfactory processing and integrating autonomic and endocrine function with the basic behaviors necessary for survival: feeding, drinking, sexual reproduction, sleep, and emergency responses. These basic behaviors are organized by the brain stem and consist of relatively simple, stereotypic motor responses. Feeding, for example, involves coordination of chewing, licking, and swallowing, motor responses that are controlled by local ensembles of neurons in the brain stem. Although we are accustomed to thinking that human behavior originates mainly in the forebrain, many complex human responses, such as feeding, are made up of relatively simple, stereotyped motor responses governed by the brain stem. A striking indicator of this pattern of organization in humans is the rare infant born without a forebrain (hydrencephalus). It is surprisingly difficult to distinguish hydrencephalic infants from normal babies. They also cry, smile, suckle, and move their eyes, face, arms, and legs. As these sad cases illustrate, the brain stem can organize virtually the entire repertory of the newborn's behavior. In this chapter, we will examine the anatomical and functional organization of a region forming the core of the brainstem that is referred to as the reticular formation . The reticular formation of the brainstem differs from other regions of the brain in that it participates in a variety of processes. These functions include sensory, motor, and autonomic functions, sleep and wakefulness cycles, consciousness, and the regulation of emotional behavior. The questions that this chapter addresses are: (1) Which structures contribute to the processing of sensory information, and what are their contributions? (2) What are the regions of the reticular formation that contribute to motor functions, and what are their contributions? (3) How does the reticular formation contribute to autonomic functions? (4) How does the reticular formation help to regulate sleep and wakefulness cycles and states of consciousness? And, finally, (5) what is the role of the reticular formation in the regulation of emotional behavior? The remainder of this chapter attempts to answer these questions by analyzing the input-output relationships of the various regions of the reticular formation and their respective roles in mediating the different processes. Figure 23-3 Cross sections of the brainstem. Note the principal nuclei of the reticular formation as well as other (nonreticular) nuclei situated adjacent to them. Many of these (other) nuclei make synaptic connections with nuclei of the reticular formation. (A) Medulla at level of rostral aspect of inferior olivary nucleus. (B) Level of caudal pons at the level of the abducens and facial nerves. (C) Rostral pons at level of the nucleus locus ceruleus and superior cerebellar peduncle. (D) Oblique section in which the dorsal aspect is at the level of the inferior colliculus of the caudal midbrain and the ventral aspect is at the level of the rostral aspect of the basilar pons. (Modified with permission from Barr ML, and Kiernan JA: The Human Nervous System, 6th ed. Philadelphia: Lippincott Williams & Wilkins, 1993, p. 153.) Sensory Systems Somatosensory Signals from the Spinal Cord As described in Chapter 9, pain and temperature signals are contained within the lateral spinothalamic tract, which passes directly from the spinal cord to the contralateral ventral posterolateral nucleus (VPL) of the thalamus. It is now well established that fibers arising from parts of the spinal cord gray matter (lamina VII) give off collaterals that terminate in specific parvocellular regions of the reticular formation, mainly adjacent to the magnocellular nuclei of the medulla ( nucleus gigantocellularis ) and pons ( nucleus reticularis pontis caudalis and nucleus reticularis pontis oralis ) (Figs. 23- 3 and 23-4). In turn, these sensory signals are then transmitted from the parvocellular to the magnocellular nuclei. Neuronal groups with the reticular formation synapse with spinoreticular fibers and give rise to long ascending fibers. Accordingly, the fibers projecting from spinal cord to the brainstem may be thought of as the first neurons in a chain of fibers that innervate the intralaminar nuclei of the thalamus, and these nuclei ultimately supply the cerebral cortex. It is believed that the information transmitted to the thalamus from the reticular formation mediates affective components of pain. We should also note that, as mentioned in Chapters 9 and 15, other fibers associated with pain modulation also supply the midbrain periaqueductal gray (PAG). Nociceptive inputs into the PAG represent part of a circuit whose descending component serves to inhibit ascending pain signals to the cerebral cortex. The results of various studies have shown that other types of sensory signals can also produce cortical excitation by virtue of their connections with the brainstem reticular formation. On the basis of these studies dating back to the period of the 1940s and 1950s, the term reticular activating system was proposed as a mechanism by which sensory and other inputs to the reticular formation can modulate cortical neurons, cortical excitability, and states of consciousness. The importance of the reticular activating system is considered later in this chapter. Anatomical Organization of the Reticular Formation The reticular formation represents a phylogenetically older region of the brain because it is found in the core of the brainstem of lower forms of many species. Its appearance in lower forms is also similar to that found in humans. The reticular formation extends from the caudal medulla rostrally up to and including the midbrain (Fig. 23-1). At the upper end of the midbrain, the reticular formation becomes continuous with several nuclei of the thalamus, with which it is both anatomically and functionally related. These nuclei include the midline and intralaminar nuclei and are described later in this chapter. The reticular formation is surrounded laterally, dorsally, and ventrally by cranial nerve nuclei, which are the ascending and descending fiber pathways of the brainstem. The reticular formation, itself, consists of many cell groups situated among large numbers of fiber bundles. The name, reticular formation, was given to this region on the basis of its histological appearance, which can be described as a reticular network of fibers and cells. The brain stem and the motor and sensory components of the spinal cord are similar in structure. However, the portions of the brain stem concerned with the cranial nerves are much more complex than the corresponding portions of the spinal cord concerned with the spinal nerves because the cranial nerves mediate more complex regulatory systems. The core of the brain stem, the reticular formation , is homologous to the intermediate gray matter of the spinal cord and is likewise more complex. Nevertheless, like the spinal cord, the reticular formation of the brain stem also contains ensembles of local-circuit interneurons that generate motor patterns and coordinate reflexes and simple stereotyped behaviors.
Figure 23-7 Different types of neurons in reticular formation can influence other regions along the neuraxis of the CNS. (A) The long descending neuron on the left (shown in red) gives off a collateral that makes synaptic contact with another neuron (shown in blue) that contains a long ascending axon. (B) Alternatively, a single neuron may bifurcate, giving rise to both long ascending and descending branches. (Used with permission from Barr ML, and Kiernan JA: The Human Nervous System, 6th ed. Philadelphia: Lippincott Williams & Wilkins, 1993, p. 156.) Organizational Considerations As mentioned earlier, the reticular formation receives a variety of inputs from disparate regions of the central nervous system (CNS) that mediate different functions. The varied functions of the reticular formation are even more dramatically reflected by the nature of the outputs. Features concerning the basic organization of the neurons in the reticular formation should be pointed out before describing the output pathways of the reticular formation. (1) The reticular formation contains cells whose axons travel long distances. Some ascend to the forebrain, and others descend to the spinal cord or project to the cerebellum. (2) The efferent fibers that travel long distances arise from the medial two thirds of the reticular formation, and those that travel only short distances as interneurons lie mainly in the lateral third of the reticular formation. (3) The main dendritic branches of the neurons are oriented in a plane perpendicular to the long axis of the brainstem (Fig. 23-6). This arrangement increases the probability that ascending and descending fibers of the reticular formation will make synaptic contact with other regions of the CNS. (4) Cells situated in the medial two thirds of the reticular formation of the medulla and pons give rise to bifurcating axons that travel for long distances in both directions (Fig. 23-7). By virtue of axon collaterals, each of these neurons can make synaptic contact with the other, thus providing an additional (sensorimotor) integrating mechanism by which signals transmitted downstream from the reticular formation can be synchronized with those projecting upstream.
Figure 23-2 The positions of the magnocellular and parvocellular regions of the reticular formation. (Modified with permission from Barr ML, and Kiernan JA: The Human Nervous System, 6th ed. Philadelphia: Lippincott Williams & Wilkins, 1993, p. 150.) General Characteristics As a general rule, the nuclei of the reticular formation are arranged in the following manner. The lateral third of the reticular formation contains small-sized cells (called parvocellular regions) whose function is to receive afferent fibers from both neighboring regions of the brainstem as well as from distant structures. The medial two thirds of the reticular formation contains different groups of large-sized cells (called magnocellular regions), which, in most instances, serve as the effector regions (i.e., the cell groups that give rise to the efferent projections of the reticular formation) (Fig. 23-2). At least two distinct magnocellular regions in the pons and one large region in the medulla have been identified. Additional groups of cells, which lie along or adjacent to the midline of the upper medulla, pons, and midbrain, are also included in the reticular formation. These cell groups comprise the raphe system of neurons. These cells are important because they produce serotonin that is distributed to wide regions of the brain and spinal cord. As will be discussed later in this chapter, the other types of monoamine neurons that supply the brain and spinal cord, namely, norepinephrine and dopamine, are also located at different levels within the reticular formation. Afferent Connections Cranial nerve nuclei and secondary sensory fibers form an outer shell that surrounds the reticular formation (and particularly the parvocellular region) on its dorsal, lateral, and ventral sides (Figs. 23-2 and 23-3). Because of this arrangement, the reticular formation is strategically positioned so that the various sensory systems can easily provide inputs into it. In this manner, the reticular formation is endowed with a capacity to modulate a wide variety of sensory processes. The reticular formation receives inputs from brainstem and forebrain regions associated with sensory modalities, as well as from structures associated with motor functions, which include the cerebral cortex and cerebellum. Moreover, structures associated with autonomic and higher order visceral processes, such as the hypothalamus and limbic system, also contribute inputs to the reticular formation. The nature of these afferent sources to the reticular formation is considered in the following sections.
Brain Stem Modulation of Sensation, Movement, and Consciousness Clifford B. Saper IN THE LAST CHAPTER WE examined the groups of interneurons surrounding cranial nerve nuclei in the reticular formation of the brain stem. These reticular interneurons have local projections that mediate reflexes and simple stereotyped behaviors, such as chewing and swallowing. In this chapter we shall explore the long projection systems of the reticular formation: the neurons whose axons ascend to the forebrain or descend to the spinal cord. These neurons regulate complex functions of the central nervous system, including the perception of pain and the control of posture and wakefulness. Through these long projection systems the brain stem maintains the level of activity necessary for sensory awareness, motor responses, and arousal related to behavioral states. Cell Groups in the Brain Stem With Long Projections Can Be Defined by Their Neurotransmitters Although early neuroanatomists described the reticular formation as being poorly organized, modern methods have demonstrated that it is composed of systems of neurons with specific neurotransmitters and connections. Such systems often extend beyond the borders of the nuclei defined by traditional cell and fiber stains. To overcome this discrepancy, earlier researchers used a combination of letters and numbers to identify clusters of neurotransmitter-specific neurons: letters to identify the neurotransmitter and numbers to indicate the rostrocaudal order of the cell group. Although this nomenclature is convenient and still widely used, it tends to obscure functional relationships between these cell groups and Nissl-stained nuclei. Figure 45-1 Noradrenergic and adrenergic neurons in the medulla and pons. A. The catecholaminergic neurons in the dorsal medulla (the A2 noradrenergic and C2 adrenergic groups) are part of the nucleus of the solitary tract. Those in the ventrolateral medulla (the A1 noradrenergic and C1 adrenergic groups) are located near the nucleus ambiguus. B. The adrenergic projection to the spinal cord arises in the C1 neurons while the noradrenergic projection to the spinal cord comes from the A5 and A7 groups as well as the locus ceruleus (LC) (A6 group) in the pons. The ascending noradrenergic input to the hypothalamus stems from both the A1 and A2 cell groups while adrenergic input to the hypothalamus comes from the C1 cell group. The Major Modulatory Systems of the Brain Noradrenergic Cell Groups Noradrenergic neurons are located in two columns, one dorsal and one ventral (Figure 45-1). At the level of the medulla the ventral column contains neurons associated with the nucleus ambiguus (A1 group); those in the dorsal column are a component of the nucleus of the solitary tract and the dorsal motor vagal nucleus (A2 group). Both groups project to the hypothalamus and control cardiovascular and endocrine functions. In the pons the ventral column includes the A5 and A7 cell groups, located in the ventrolateral reticular formation of the pons. These A5 and A7 groups provide mainly projections to the spinal cord that modulate autonomic reflexes and pain sensation. Adrenergic Cell Groups Some neurons in the two columns of cells in the medulla identified as catecholaminergic were later found to synthesize epinephrine. The C1 adrenergic cell group forms a rostral extension from the A1 column in the rostral ventrolateral medulla (Figure 45-1). Many C1 neurons project to the spinal cord, particularly to the sympathetic preganglionic column, where they are thought to provide tonic excitatory input to vasomotor neurons. Other C1 neurons terminate in the hypothalamus, where they modulate cardiovascular and endocrine responses. The C2 adrenergic neurons, which are a component of the nucleus of the solitary tract , contribute to the ascending pathway to the parabrachial nucleus (Figure 45-1), which is thought to transmit gastrointestinal information . The C3 adrenergic group is located near the midline at the rostral end of the medulla. Neurons mixed in with the C3 and C1 groups provide a major input to the locus ceruleus, but most of the cells contributing to this pathway are not adrenergic.
The noradrenaline pathways in the brain Many regions of the brain are supplied by the noradrenergic systems. The principal centres for noradrenergic neurones are the locus coeruleus and the caudal raphe nuclei. The ascending nerves of the locus coeruleus project to the frontal cortex, thalamus, hypothalamus and limbic system. Noradrenaline is also transmitted from the locus coeruleus to the cerebellum. Nerves projecting from the caudal raphe nuclei ascend to the amygdala and descend to the midbrain. Figure 45-2 Noradrenergic neurons in the pons. A. Noradrenergic neurons are spread across the pons in three more or less distinct groups: the locus ceruleus (A6 group) in the periaqueductal gray matter, the A7 group more ventrolaterally, and the A5 group along the ventrolateral margin of the pontine tegmentum. B. The A5 and A7 neurons mainly innervate the brain stem and spinal cord, whereas the locus ceruleus provides a major ascending output to the thalamus and cerebral cortex as well as descending projections to the brain stem, cerebellum, and spinal cord. A = amygdala; AO = anterior olfactory nucleus; BS = brain stem; C = cingulate bundle; CC = corpus callosum; CT = central tegmental tract; CTX = cerebral cortex; DT = dorsal tegmental bundle; EC = external capsule; F = fornix; H = hypothalamus; HF = hippocampal formation; LC = locus ceruleus; OB = olfactory bulb; PT = pretectal nuclei; RF = reticular formation; S = septum; T = tectum; Th = thalamus. The A6 cell group, the locus ceruleus , sits dorsally and laterally in the periaqueductal and periventricular gray matter (Figure 45-2). The locus ceruleus, which maintains vigilance and responsiveness to unexpected environmental stimuli, has extensive projections to the cerebral cortex and cerebellum, as well as descending projections to the brain stem and spinal cord. NOREPINEPHRINE (NORADRENALIN) Norepinephrine (along with acetylcholine) is one of the two neurotransmitters in the peripheral nervous system. Norepinephrine is synthesized from dopamine by means of the enzyme D opamine B eta- H ydroxylase (DBH), with oxygen, copper and Vitamin C as co-factors. Dopamine is synthesized in the cytoplasm, but norepinephrine is synthesized in the neurotransmitter storage vesicles. Cells that use norepinephrine for formation of epinephrine use SAMe (S-AdenylMethionine) as a methyl group donor. Levels of epinephrine in the CNS are only about 10% of the levels of norepinephrine. The most prominent noradrenergic (ie, norepinephrine-containing) nucleus is the locus ceruleus in the pons, which account for over 40% of noradrenergic neurons in the rat brain. Most of the other noradrenergic neurons are clustered in a region described as the lateral tegmental area . The neocortex, hippocampus, and cerebellum receive noradrenergic stimulation exclusively from the locus ceruleus. Most of the dopaminergic innervation of the hypothalamus comes from the lateral tegmental nuclei. Electrical stimulation of the locus ceruleus produces a state of heightened arousal. The noradrenergic system is most active in the awake state, and it seems to be important for focused attention, in contrast to the motor arousal of dopamine. Although the locus ceruleus has been identified as a pleasure center, it also seems to contribute to anxiety. Increased neuronal activity of the locus ceruleus is seen upon the occurrence of unexpected sensory events. Brain norepinephrine turnover is increased in conditions of stress. Benzodiazepines, the primary antianxiety drugs, decrease firing in the locus ceruleus, thus reducing distribution of noradrenalin to the forebrain and amygdala . This is part of the explanation for the use of benzodiazepines for inducing sleep . Active projection of norepinephrine from the locus coeruleus of the reticular activating system to the forebrain is a key feature of awakeness-arousal as distinguished from sleep. Norepineprhine projection to the basal nucleus of the forebrain is low in sleep -- virtually absent in REM (Rapid Eye-Movement) sleep. The basal nucleus when stimulated by norepinephrine from the locus coeruleus sends neuromodulating acetylcholine to the cerebral cortex, thereby promoting alertness. The beta-adrenergic blocking drug propranolol has also been used to treat anxiety. By blocking the adrenergic inputs to the amygdala, beta-blockers inhibit the formation of traumatic memories. Cortisol stimulation of the locus coeruleus due to chronic stress exacerbates norepinephrine stimulation of the amygdala. Beta-noradrenergic receptors also apparently inhibit feeding, whereas alpha-receptors seem to stimulate feeding. Although MAO inhibitors reduce metabolism of all catecholamines, it is believed that the anti-depressant effect is more related to norepinephrine than to dopamine. Most MAO in the brain is of type-B, but drugs selective for inhibiting MAO-A have proven to be better anti-depressants. MAO-A preferentially metabolizes norepinephrine & serotonin. MAO-A inhibiting drugs given for depression have critically elevated blood pressure in patients eating tyramine-containing foods (such as cheese) due to the failure to metabolize tyramine (which can act as a pressor agent). These drugs (eg, phenelzine & pargyline) inactivate MAO by forming irreversible covalent bonds. More modern MAO inhibitors are safer because they form reversible bonds. MAO-B inhibitors like deprenyl are also less likely to cause the "cheese effect". (Alcohol also selectively inhibits MAO-B.) Tricyclic Antidepressants Tricyclic anti-depressants derive their name from their 3-ring structure. Desipramine only inhibits norepinephrine re-uptake, with little effect on dopamine. Imipramine & amitriptyline are inhibitors of norepinephrine and serotonin re-uptake by the presynaptic terminals, but are more potent for serotonin. Cocaine is also a potent inhibitor of catecholamine re-uptake, but it does not act as an anti-depressant. Weight gain due to increased appetite is a frequent side effect of tricyclic anti-depressants, particularly of amitrip- tyline. By contrast, both cocaine & amphetamine reduce appetite. Both MAO inhibitors and tricyclic anti-depressants have immediate effects on brain monoamines, but clinically anti-depressants require several weeks of administration before they produce a therapeutic effect. It is therefore believed that it is not the immediate effects on neurotransmitters that is producing the antidepression, but the long-term effects on modification of receptors. Excessive cortisol secretion is seen in 40-60% of depressed patients, associated with diminished noradrenergic inhibition of corticotropin-releasing hormone secretion in the hypothalamus. Corticotropin-releasing hormone induces anxiety in experimental animals.
The dopamine pathways in the brain Dopamine is transmitted via three major pathways. The first extends from the substantia nigra to the caudate nucleus-putamen (neostriatum) and is concerned with sensory stimuli and movement. The second pathway projects from the ventral tegmentum to the mesolimbic forebrain and is thought to be associated with cognitive, reward and emotional behaviour. The third pathway, known as the tubero-infundibular system, is concerned with neuronal control of the hypothalmic-pituatory endocrine system Figure 45-3 Dopaminergic neurons in the brain stem and hypothalamus. A. Dopaminergic neurons in the substantia nigra (A9 group) and the adjacent retrorubral field (A8 group) and ventral tegmental area (A10 group) provide a major ascending pathway that terminates in the striatum, the frontotemporal cortex, and the limbic system, including the central nucleus of the amygdala and the lateral septum. B. Hypothalamic dopaminergic neurons in the A11 and A13 cell groups, in the zona incerta, provide long descending pathways to the autonomic areas of the lower brain stem and the spinal cord. Neurons in the A12 and A14 groups, located along the wall of the third ventricle, are involved with endocrine control. Some of them release dopamine as a prolactin release inhibiting factor in the hypophysial portal circulation. . Dopaminergic Cell Groups The dopaminergic cell groups in the midbrain and forebrain were originally numbered as if they were a rostral continuation of the noradrenergic system because identification was based on histofluorescence, which does not distinguish dopamine from norepinephrine very well. The A8-A10 cell groups include the substantia nigra pars compacta and the adjacent areas of the midbrain tegmentum (Figure 45-3). They send the major ascending dopaminergic inputs to the telencephalon, including the nigrostriatal pathway that innervates the striatum and is thought to be involved in initiating motor responses. Mesocortical and mesolimbic dopaminergic pathways arising from the A10 group innervate the frontal and temporal cortices and the limbic structures of the basal forebrain. These pathways have been implicated in emotion, thought, and memory storage. The A11 and A13 cell groups, in the dorsal hypothalamus, send major descending dopaminergic pathways to the spinal cord. These pathways are believed to regulate sympathetic preganglionic neurons. The A12 and A14 cell groups, along the wall of the third ventricle, are components of the tuberoinfundibular hypothalamic neuroendocrine system. Dopaminergic neurons are also found in the olfactory system (A15 cells in the olfactory tubercle and A16 in the olfactory bulb) and in the retina (A17 cells). Once in the brain, tyrosine can be converted to D ihydr O xy P henyl A lanine ( DOPA ) by the tyrosine hydroxylase enzyme using oxygen, iron and T etra H ydro B iopterin (THB) as co-factors. High concentrations of dopamine inhibit tyrosine hydroxylase activity through an influence on the THB co-factor. DOPA is converted to dopamine by A romatic A mino A cid D ecarboxylase (which is fairly nonspecific insofar as it will decarboxylate any aromatic amino acid) using P yridoxa L P hosphate (PLP) as a co-factor. This reaction is virtually instantaneous unless there is a Vitamin B6 deficiency. Dopamine & epinephrine are primarily inhibitory neurotransmitters that produce arousal. This may sound paradoxical, but the most likely explanation for this effect is that the postsynaptic cells for catecholamines themselves are inhibitory. There are 3-4 times more dopaminergic cells in the CNS than adrenergic cells. Dopamine in the caudate nucleus facilitates posture, whereas dopamine in the nucleus accumbens is associated with an animal's speed (and pleasure ). There are two primary dopamine receptor-types: D1 (stimulatory) and D2 (inhibitory), both of which act through G-proteins. D2 receptors often occur on the dopaminergic neurons, partially for the purpose of providing negative feedback . These so-called autoreceptors can inhibit both dopamine synthesis and release. The binding of dopamine to D1-receptors stimulates the activity of Adenylyl Cyclase (AC), which converts ATP to cyclic AMP (cAMP), a second messenger which binds to Protein Kinase A (PKA). PKA then modulates the activity of various proteins by the addition of phosphate. There are 4 main dopaminergic tracts in the brain: (1) the nigrostriatial tract from the substantia nigra to the striatum accounts for most of the brain's dopamine (2) the tuberoinfundibular tract from the arcuate nucleus of the hypothalamus to the pituitary stalk, which has a controlling effect on the release of the hormones prolactin through tonic inhibition via D2 receptors (3) the mesolimbic tract from the ventral tegmental area to many parts of the limbic system and (4) the mesocortical tract from the ventral tegmental area to the neocortex, particularly the prefrontal area. Dopamine cells project topographically to the areas they innervate.
The serotonin pathways in the brain The principal centres for serotonergic neurones are the rostral and caudal raphe nuclei. From the rostral raphe nuclei axons ascend to the cerebral cortex, limbic regions and specifically to the basal ganglia. Serotonergic nuclei in the brain stem give rise to descending axons, some of which terminate in the medulla, while others descend the spinal cord. Figure 45-4 Serotonergic neurons along the midline of the brain stem. Neurons in the B1-3 groups, corresponding to the raphe magnus, raphe pallidus, and raphe obscurus nuclei in the medulla, project to the lower brain stem and spinal cord. Neurons in the B4-9 groups, including the raphe pontis, median raphe, and dorsal raphe nuclei, project to the upper brain stem, hypothalamus, thalamus, and cerebral cortex. CD = caudate nucleus; HF = hippocampal formation; H = hypothalamus; Th = thalamus. Serotonergic Cell Groups Most serotonergic neurons are located along the midline of the brain stem in the raphe nuclei (from raphé , French for seam ). Raphe neurons in the B1-B3 cell groups along the midline of the caudal medulla (Figure 45-4) send descending projections to the motor and autonomic systems in the spinal cord. The raphe magnus nucleus (B4) at the level of the rostral medulla projects to the spinal dorsal horn and is thought to modulate the perception of pain. The serotonergic groups in the pons and midbrain (B5-B9) include the pontine, dorsal, and median raphe nuclei and project to virtually the whole of the forebrain. Serotonergic pathways play important regulatory roles in hypothalamic cardiovascular and thermoregulatory control and modulate the responsiveness of cortical neurons. Serotonin seems to have distinctive actions contributing to anxiety and impulsive behavior . Patients with evidence of low serotonin levels have attempted suicide by very dramatic means, such as cutting the throat . This may explain some of the therapeutic effects of fluoxetine (Prozac), which selectively prevents the re-uptake of serotonin. Fluoxetine is also distinctive because it has a half-life of about four days. Fluoxetine has been used therapeutically for panic, obsessive-compulsive and eating disorders (such as bulimia). Unlike the tricyclic anti-depressants, which often stimulate appetite, fluoxetine more often reduces appetite. Fluoxetine may even enhance learning [PHARMACOLOGY BIOCHEMISTRY AND BEHAVIOR 52:341-346 (1995)]. Depression patients treated with tryptophan as well as fluoxetine show less sleep disturbance at the outset of treatment than patients treated with fluoxetine alone [ JOURNAL OF PSYCHIATRY & NEUROSCIENCE; Levitan,RD; 25(4):337-346 (2000) ]. Monkeys with high levels of testosterone & low levels of serotonin are both aggressive & lacking in restraints on impulsive/violent behavior. Arsonists who commit their crime for mercenary reasons show normal levels of serotonin, but those who commit the crime impulsively have low serotonin . Lead interferes with serotonin synapse formation. Monkeys experimentally exposed to lead became so dangerously aggressive that the study was halted early [ CHEMICAL & ENGINEERING NEWS 81(22):33-37 (2003) ]. Reserpine prevents the transport of all the monoamines (and acetylcholine) into storage vesicles in the presynaptic membrane -- leaving them vulnerable to destruction by monoamine oxidase. Reserpine (as extracts from the Rauwolfia plant) was used for centuries in India to treat "hysteria". Reserpine has been used as a potent tranquilizer, but it can produce serious depression that may lead to suicide attempts. LySergic acid Diethylamine (LSD) acts most strongly on the type-2 serotonin receptors, but it also has some effect on norepinephrine receptors. Serotonin seems to play a role in dreaming . During both dreaming and LSD intoxication, electrical activity in the visual cortex arises from the brain stem rather than from the eyes . LSD not only induces visual hallucinations, but it heightens sensory awareness while diminishing control of sensory input. The reduced ability to distinguish between sensory impressions can lead to feelings of being "in union with the universe". Artificial stimulation of the raphe simulates the actions of LSD, decreasing habituation to repetitive stimuli. Low doses of LSD & amphetamine, however, have been shown to enhance a form of associative learning. High-estrogen contraceptives may have contributed to depression by lowering serotonin levels in the brain. Low levels of growth hormone in depressed patients may be due either to low levels of norepinephrine, serotonin, or both.
Distribution of acetylcholine receptors in the brain There are two main types of cholinergic receptors widely distributed throughout in the brain. These receptors are classified as muscarinic and nicotinic receptors. In certain regions of the brain only the muscarinic subtype is found eg midbrain, medulla, and pons while in other regions eg substantia nigra, locus coeruleus and septum only the nicotinic receptor subtype is found. Both sub-types are located in the corpus striatum, cerebral cortex, hippocampus, thalamus, hypothalamus and cerebellum. Figure 45-5 Cholinergic neurons in the upper pontine tegmentum and basal forebrain diffusely innervate much of the brain stem and forebrain. The basal forebrain cholinergic groups include the medial septum (MS) (Ch1 group), nuclei of the vertical and horizontal limbs of the diagonal band (DBv and DBh) (Ch2 and Ch3 groups), and the nucleus basalis of Meynert (BM) (Ch4 group), which topographically innervate the entire cerebral cortex, including the hippocampus (Hi) and the amygdala (Am). The pontine cholinergic neurons, in the laterodorsal (LDT) (Ch5 group), and pedunculopontine (PPT) (Ch6 group), tegmental nuclei, innervate the brain stem reticular formation (RF) as well as the thalamus (Th). Ha = habenular nucleus; IPN = interpeduncular nucleus; LH = lateral hypothalamus; MaPo = magnocellular preoptic nucleus; OB = olfactory bulb; VTA = ventral tegmental area. Cholinergic Cell Groups Acetylcholine is the transmitter used by both somatic and autonomic motor neurons. Certain populations of cholinergic interneurons are found in the brain stem and forebrain, and large cholinergic neurons in the mesopontine tegmentum and basal forebrain give rise to long ascending projections (Figure 45-5). The mesopontine cholinergic neurons are divided into a ventrolateral column (Ch6 cell group, or the pedunculopontine nucleus ), close to the lateral margin of the superior cerebellar peduncle, and a dorsomedial column (Ch5 cell group, or the laterodorsal tegmental nucleus ), a component of the periaqueductal gray matter just rostral to the locus ceruleus. These two cell groups send a major descending projection to the pontine and medullary reticular formation and provide extensive ascending cholinergic innervation of the thalamus. These projections are thought to play an important role in regulating wake-sleep cycles (Chapter 47).
Figure 23-13 Descending motor pathways to the spinal cord from the pons and medulla. Note also that corticoreticular fibers from motor and premotor cortices modulate the activity neurons of the reticular formation that give rise to the reticulospinal tracts. In turn, reticulospinal tracts modulate the activity of alpha and gamma motor neurons. Activation of the lateral reticulospinal tract inhibits spinal reflexes (-), and activation of the medial reticulospinal tract facilitates (+) spinal reflexes. Motor Systems It is clear that the reticular formation plays an important role in the processing of sensory information. The likely mechanisms are discussed in the following sections. As noted in previous chapters concerning motor systems, the reticular formation also plays an important role in the regulation of motor responses. The magnocellular nuclei of the reticular formation of the medulla and pons receive significant inputs from two key regions associated with motor functions: the cerebellum and sensorimotor cortex. Cerebellum The reticular formation and cerebellum share reciprocal connections, which complete a circuit comprising feedback pathways between these two regions for the regulation of motor functions associated with each of these two structures. Cerebellar fibers that project to the reticular formation of the medulla and pons arise from the fastigial nucleus . The fibers are both crossed and uncrossed and use the uncinate fasciculus (the pathway that passes just dorsal to the superior cerebellar peduncle). Cerebral Cortex Fibers from the same region of the sensorimotor cortex (areas 4, 3, 1, and 2) that give rise to much of the corticospinal tract also give rise to corticoreticular fibers. Corticoreticular fibers terminate in the pons and medulla near cell groups that give rise to the reticulospinal tracts (nucleus reticularis pontis oralis and nucleus reticularis pontis caudalis for the pons, and nucleus gigantocellularis for the medulla) (Fig. 23-5). In this way, corticoreticular fibers can influence both voluntary as well as reflex motor functions by acting on those neurons of the reticular formation that control extensor motoneuron activity. Autonomic (and Higher Order Visceral Regulatory) Regions The reticular formation receives autonomic inputs from different sources. One set of sources includes primary afferent fibers contained in cranial nerves (CN) IX and X. The other source includes fibers arising from higher order autonomic integrative regions, which include the hypothalamus, as well as parts of the limbic system. Cranial Nerve (Autonomic) Nuclei As indicated in Chapter 14, fibers of the glossopharyngeal and vagus nerves (CN IX and X) transmit both chemoreceptor and baroreceptor afferent signals to the brainstem. The signals arise from the aortic and carotid bodies (chemoreceptors) and the aortic arch and carotid sinus (baroreceptors) and terminate in the solitary nucleus. Secondary neurons located in the solitary nucleus then project to the nucleus ambiguus and the ventrolateral medullary depressor areas located in the medullary reticular formation. As noted earlier, this information is important for reflex regulation of blood pressure and respiration. Autonomic regions of the brainstem reticular formation that provide basic mechanisms for the control of blood pressure, heart rate, and respiration were considered in Chapter 22. Forebrain Regions (Hypothalamus and Limbic System) Several different pathways that arise from both lateral and medial regions of the hypothalamus project downstream and make synaptic connections in different parts of the reticular formation, mainly the midbrain and pons. These regions of hypothalamus project most heavily to the midbrain PAG and neighboring regions of the dorsal and lateral tegmental fields of the reticular formation. Additional groups of fibers from the amygdala supply the PAG, tegmentum, and lower brainstem region (in and adjacent to the solitary nucleus). Other limbic structures also contribute fibers to the reticular formation. These include inputs from the prefrontal cortex and amygdala that are mainly directed to the midbrain PAG. These descending inputs provide a higher order control of central autonomic functions of the brainstem reticular formation. Pathways to Regions Mediating Motor Functions We have previously established that the reticular formation receives inputs from two regions that mediate motor functions: the sensorimotor cortex and cerebellum. Inputs from both of these regions modulate the activity of neurons in the reticular formation that project to the spinal cord. Recall that the afferents from both of these regions and, in particular, corticoreticular fibers terminate near the origins of these descending reticulospinal fibers. The primary motor outputs of the reticular formation are directed on the spinal cord as reticulospinal fibers. As indicated in Chapters 9, 19, and 21, these fibers arise from the pons and medulla. The fibers arising from the pons form the medial reticulospinal tract and issue from the nucleus reticularis pontis oralis and nucleus reticularis pontis caudalis. They pass in the ventral funiculus of the spinal cord and facilitate both alpha and gamma motor neurons of extensors. In contrast, fibers from the medulla arise from the magnocellular nuclei, such as the nucleus gigantocellularis, and descend in the ventral funiculus as the lateral reticulospinal tract, where they also terminate on alpha and gamma motor neurons of extensors. However, their action on these neurons is inhibitory. Collectively, the actions of the reticulospinal fibers serve to modulate muscle tone, regulate posture, and participate in automatic reflex mechanisms involving the extensor musculature (Figs. 23-13 and 23-14) (see also Chapter 19). Alterations in posture and muscle tone can be mediated by the corticoreticular pathways as part of the overall voluntary motor control system (see Chapter 19). The actions of the cerebellum are somewhat different. The reticular formation receives feedback signals from the fastigial nucleus as part of an automatic regulatory mechanism. The feedback message to the reticular formation is produced in response to signals that the cerebellar cortex receives from the reticular formation. Thus, the efferent connections of the reticular formation to the cerebellar cortex complete a feedback circuit linking these two important structures for the regulation of posture and muscle tone. The efferent pathways to the cerebellar cortex from the reticular formation arise from two nuclei of the medulla (the lateral and paramedian reticular nuclei) and one nucleus from the pons (reticulotegmental nucleus). The closely integrated response network between the cerebellum, cerebral cortex, and reticular formation is extremely important for the proper maintenance of postural mechanisms and standing erect, especially since there is a delicate balance between the excitatory and inhibitory actions of different regions of the reticular formation on extensor motor neurons. Disruption of any component of this network can lead to significant motor deficits. These deficits include spasticity if the inhibitory components of the reticulospinal pathways are disrupted by loss of corticoreticular inputs, rigidity if the inputs from the cerebellum to the inhibitory zones of the reticular formation are disrupted, and hypertonicity if cerebellar inputs on the excitatory components are disrupted. Other motor functions that involve the reticular formation include the control of horizontal eye movements. As described in Chapter 14, the horizontal gaze center is located in the reticular formation and adjacent to the abducens nucleus and is chiefly responsible for the organization of horizontal eye movements. This region integrates signals from the cerebral cortex (frontal eye fields) and vestibular nuclei. As a result, the horizontal gaze center enables conjugate horizontal movements of the eyes to occur, especially in response to changes in body posture and position of the head in space.
Figure 23-14 Effects of stimulation of reticular formation on spinal reflexes. Stimulation of the facilitory zone (+) (shown in green) of the reticular formation causes a dramatic increase in the patellar reflex as determined by EMG measurements, whereas marked suppression of this reflex follows stimulation of the inhibitory zone (-) (shown in red) of the reticular formation.
Descending Projections From the Brain Stem to the Spinal Cord Modulate Sensory and Motor Pathways Pain Is Modulated by Descending Monoaminergic Projections Monoaminergic projections to the dorsal horn of the spinal cord descend from the serotoninergic raphe magnus nucleus in the midline of the rostral medulla and from the noradrenergic cell groups in the pons. Activation of either of these monoaminergic pathways can inhibit the transmission of nociceptive information (see Chapter 24). The serotonergic neurons in the raphe magnus nucleus receive afferents from enkephalinergic neurons in the periaqueductal gray matter. Electrical stimulation of the periaqueductal gray matter produces analgesia that is blocked by administering the opiate antagonist naloxone into the raphe magnus, suggesting that the endogenous opiates released there activate the descending modulatory pathway. Other, nonserotonergic neurons in the medial medullary reticular formation adjacent to the raphe magnus have firing patterns that are correlated with reflex responses to painful stimuli. These neurons may also contribute to descending modulation of nociception.
Figure 45-7 Injuries to the ascending arousal system, from the rostral pons through the thalamus and hypothalamus (purple area), can cause loss of consciousness. Ascending Projections From the Brain Stem Modulate Arousal and Consciousness The ascending pathways from monoaminergic cell groups in the brain stem and hypothalamus to the cerebral cortex and thalamus increase wakefulness and vigilance, as well as the responsiveness of cortical and thalamic neurons to sensory stimuli, a state known as arousal. These pathways are joined by ascending cholinergic inputs from the pedunculopontine and laterodorsal tegmental nuclei and by other cell groups from the parabrachial nucleus through the paramedian midbrain reticular formation to form an ascending arousal system . The ascending arousal system divides into two major branches at the junction of the midbrain and diencephalon. One branch enters the thalamus, where it activates and modulates thalamic relay nuclei as well as intralaminar and related nuclei with extensive diffuse cortical projections. The other branch travels through the lateral hypothalamic area and is joined by the ascending output from the hypothalamic and basal forebrain cell groups, all of which diffusely innervate the cerebral cortex. Lesions that disrupt either of these two branches impair consciousness (Figure 45-7). Consciousness Represents the Summated Activity of the Cerebral Cortex The nature of consciousness has been a subject of intense philosophical concern at least since Plato's Meno. However, only within the past 100 years has speculation on the basis of consciousness been informed by scientific understanding of how the brain works. Currently, there is general agreement that consciousness is the property of being aware of oneself and one's place in the environment. Scientifically, this is a very difficult property to measure (see Chapter 20). As a result, clinicians generally rely on a pragmatic definition based on observation: the ability of the individual to respond appropriately to environmental stimuli. Careful clinical observations show that this ability to orient appropriately to stimuli is dependent upon the summated activity of the two cerebral hemispheres. When parts of the cerebral cortex are damaged a patient may be unable to process certain types of information, and thus the patient is not conscious of certain aspects of the environment. For example, a patient with a lesion in Wernicke's area in the dominant hemisphere may not be aware of the semantic content of speech, and thus would use and interpret language only for emotional gesturing. This type of “fractional” loss of consciousness is discussed in greater detail in Chapter 19. According to this view of conciousness, generalized impairment of consciousness implies diffuse dysfunction in both cerebral hemispheres. One problem with a definition of consciousness based on responsiveness to stimuli emerged at the beginning of the twentieth century, when clinicians began to report cases of patients with injuries to the brain stem but no injuries to the cerebral hemispheres who were unable to respond to stimuli. Most observers thought that the inability to respond reflected mainly impairment of sensory and motor pathways. In the absence of an independent measure of cortical activity, this view was difficult to disprove.
Figure 23-8 The ascending connections of the reticular formation and inputs into the reticular formation from lower levels of the CNS. The reticular formation receives spinoreticular fibers (shown in red). The ascending reticular fibers project either directly to the intralaminar nuclei (shown in red) or indirectly through an interneuron from the solitary nucleus to the dorsolateral pons first (shown in blue); neurons from intralaminar nuclei then project directly to the cortex (shown in red) or to specific thalamic nuclei, which then project to the cerebral cortex (not shown in this diagram). By either direct or indirect routes, inputs from the reticular formation can influence cortical activity and the transmission of sensory signals to the cortex. Pathways to Regions Mediating Sensory Functions and Effects on Cortical Excitability Levels There are at least three ways in which the reticular formation can modulate sensory functions and cortical excitability. The first two mechanisms involve projections from the reticular formation to the intralaminar nuclei of the thalamus, and the third mechanism involves direct projections from monoaminergic neurons of the reticular formation to the cerebral cortex. Consider first the projections from the reticular formation to the thalamus. Fibers from nuclei within the reticular formation project to nonspecific thalamic nuclei, including the centromedian (CM) and parts of the ventral anterior (VA) nucleus, whose properties mimic those of a nonspecific thalamic nucleus (for further discussion, see Chapter 26). In turn, these nonspecific thalamic nuclei project to wide regions of cortex directly or indirectly through a synapse in the ventral anterior nucleus (Fig. 23-8). Although the projection from the ventral anterior nucleus to the cortex is extensive, its projection is directed principally to the frontal lobe. Because of the widespread projections, activation of the nonspecific thalamic nuclei by the reticular formation can lead to changes in cortical neuron excitability levels. There is a second, alternative mechanism that could also be operative. Neurons in nonspecific thalamic nuclei are known to make synaptic contact with specific thalamic nuclei (Fig. 23-9). Here, nonspecific thalamic nuclei can modify sensory transmission at the level of the thalamus by interacting with specific thalamic nuclei before the signals can reach sensory regions of the cerebral cortex. Evidence for a functional relationship between the reticular formation and cerebral cortex comes from electrical stimulation studies in which low-frequency stimulation of nonspecific thalamic nuclei produces a distinctive cortical electrical pattern called a recruiting response . This response is characterized by a surface negative wave, which reaches a maximum amplitude rapidly and then slowly decreases in size. Additional stimulation results in a waxing and waning of the cortical wave. The behavioral response noted from such stimulation of the nonspecific thalamus is that the patient has a drowsy appearance. In contrast, electrical stimulation of the brainstem Figure 23-4 The connections of the lateral spinothalamic tract, including those made with the reticular formation. Other Secondary Sensory Systems All sensory systems contribute fibers that ultimately make their way into the reticular formation. Trigeminal (for somatosensory information), solitary (for taste information), auditory, and vestibular nuclei lie adjacent to the reticular formation. Information is thus transmitted to the reticular formation from these structures, either as a result of the dendritic arborizations of neurons whose cell bodies lie in the lateral aspect of the reticular formation but which extend into these regions or by short axons that arise from these sensory regions that pass into the lateral aspects of the reticular formation. In addition to these sensory inputs, impulses mediated from regions associated with olfactory and visual systems also contribute inputs to the reticular formation. Secondary olfactory signals are received by a number of limbic structures (amygdala, hippocampal formation, and septal area) that have known projections to the reticular formation (see page 415 and Chapters 24 and 25). Visual signals can reach the superior colliculus via optic tract fibers. From the superior colliculus, fibers project directly to the reticular formation of the midbrain and pons. Thus, it is evident that the reticular formation receives multiple sensory inputs from all sensory systems. The reticular formation cannot maintain the specificity of the information that it receives from each of these sensory systems. Therefore, information of a nonspecific nature is transmitted via ascending fibers to the thalamus; this is in contrast to the specific transmission lines characteristic of other ascending sensory systems such as the dorsal column-medial lemniscus pathway. As indicated earlier, an important function of these signals that enter the reticular formation is to allow the reticular activating system to alter excitability levels of target neurons in the thalamus.
Figure 45-8 The electroencephalogram measures electrical activity in the cerebral cortex. A. Transection of the lower brain stem at the level shown in the drawing isolates the brain from incoming sensory signals through the spinal cord, a preparation the Belgian neurophysiologist Frederic Bremer called the encephale isolé. Animals with this lesion are awake, respond to trigeminal sensory as well as visual and auditory cues, and move their faces and eyes in a normal fashion. The electroencephalogram (EEG) of such animals is typically low voltage and fast, a desynchronized pattern typical of waking. B. When a cut is made at the level indicated in the drawing, between the superior and inferior colliculi, the cat appears to be sleeping, with no eye movement responses to visual stimuli. In animals the EEG pattern is typically high voltage and slow, a synchronized pattern consistent with sleep. Fortunately, in the late 1920s Hans Berger, a Swiss psychiatrist, invented the electroencephalogram (EEG) to assess the electrical activity of the cerebral cortex (see Box 46-1). During alert wakefulness the EEG shows a pattern of low-voltage, fast (>12 Hz) electrical activity called desynchronized. During deep sleep the EEG is dominated by high-voltage, slow (<3 Hz) electrical activity called synchronized (Figure 45-8). These patterns are discussed in detail in Chapter 47.
Figure 23-11 Electrical stimulation of the reticular formation. EEG recordings from the studies of Moruzzi and Magoun of the activating patterns of the brainstem reticular formation on the cortex. The four tracings are recorded over different parts of the cerebral cortex of the cat. The arrows pointing up and down indicate the onset and offset of electrical stimulation. Note the desynchronization of the EEG during stimulation followed by a return to a synchronized pattern after stimulation is terminated. Thus, one role of the reticular formation is to provide activation of the cerebral cortex (Fig. 23-11). The process of arousal is highly important because it serves to change excitability levels (i.e., prime the sensory [and other] neurons) of the cortex so that they will become more receptive to other sensory inputs that reach the cerebral cortex through the classical ascending sensory pathways. For example, upon awaking to the sound of fire engines, there is activation of the reticular formation by descending cortical fibers and additional auditory signals (i.e., the continued sounding of the fire engines). This produces cortical desynchronization ( beta rhythm ) and enables the individual to respond in an appropriate way that generates conscious awareness of these stimuli. It should further be pointed out that the reticular formation can also provide inhibitory modulation of sensory signals. In Chapter 15 ( Somatosensory System ), we indicated that the reticular formation comprises part of a descending pain-inhibitory pathway. This pathway originates in the midbrain PAG; it is enkephalinergic, and an enkephalinergic neuron synapses on serotonin neurons in the raphe magnus. This nucleus gives rise to a descending serotonin neuron that reaches the dorsal horn of the spinal cord and synapses on another enkephalin neuron, which ultimately modulates the primary afferent nociceptive pathway at this level of the spinal cord. It is possible that the reticular formation further modulates other sensory inputs, thus enabling us to â€oefilter out†unwanted sensory information so that we can more clearly focus on more critical stimuli.
Figure 45-9 Thalamic relay neurons have transmission and burst modes of signaling activity. Left. Burst mode. When thalamic neurons are hyperpolarized by inhibitory postsynaptic potentials they respond to brief depolarizations with a burst of action potentials (left). Each burst of action potentials causes a barrage of synchronized excitatory postsynaptic potentials in the dendrites of cortical neurons, producing an EEG slow-wave pattern known as synchronized activity. Right. Transmission mode. When thalamic neurons are in a more depolarized state, incoming excitatory potentials produce single action potentials. In this mode the thalamic neuron faithfully transmits sensory impulses to the cerebral cortex but the complex patterning of thalamic firing produces nearly constant, small-scale alterations in the dendritic potentials of cortical neurons. The resulting EEG pattern of fast, low-voltage waves is termed desynchronized. The EEG Reflects Two Modes of Firing of Thalamic Neurons The EEG is important in assessing wakefulness because electrical activity in the cerebral cortex reflects the firing patterns in the thalamocortical system, a necessary component of maintaining a waking state. As we shall learn in the next two chapters, electrical activity measured from the surface of the skull reflects the summated activity of synaptic potentials in the dendrites of cortical neurons. The specific rhythmic pattern of the EEG waveform thus reflects synchronized waves of excitatory synaptic potentials reaching the cerebral cortex from the thalamus. The rhythmic nature of the thalamic activity is due, in turn, to two important properties of the thalamic relay neurons. First, the thalamic relay neurons have two distinct physiological states: a transmission mode and a burst mode (Figure 45-9). When the resting membrane potential of the thalamic relay neuron is near the firing threshold, the neuron is in transmission mode: incoming excitatory synaptic potentials can drive the neuron to fire in a pattern that reflects the sensory stimulus. When the thalamic neuron is hyperpolarized by inhibitory input, it is in burst mode. As we shall learn in detail in Chapter 46, the thalamic relay neurons have a special voltage-gated calcium channel that is inactivated when the membrane potential is near threshold. When the relay cell is hyperpolarized incoming excitatory synaptic potentials can trigger transient opening of the calcium channels. These channels produce a calcium current that brings the neuron's membrane potential above threshold for firing action potentials. The cell now fires a burst of action potentials that produce further calcium channel openings, until sufficient calcium has entered the cell to trigger a calcium-activated potassium current. This potassium current hyperpolarizes the cell, resetting it for another cycle of burst firing. This raises some questions. How do the thalamic relay cells become hyperpolarized in the first place? What is the nature of the inhibitory input? The thalamic relay neurons have a strong reciprocal interaction with GABA-ergic inhibitory interneurons in the reticular nucleus of the thalamus. The reticular nucleus forms a sheet of GABA-ergic neurons that sits along the outer surface of the thalamus. Their dendrites receive collaterals from both thalamocortical and corticothalamic axons that pass through it. The reticular nucleus is topographically organized, and its neurons project back to relay nuclei from which they receive their inputs. When the reticular nucleus neurons fire, they hyperpolarize thalamic relay neurons, thereby determining whether the thalamic relay neurons will be able to reach firing threshold in response to sensory inputs. Both the thalamic relay nuclei and the inhibitory neurons of the reticular nucleus enter burst mode when they are hyperpolarized. The input from the reticular neurons produces inhibitory synaptic potentials in the relay neurons that are mediated by GABAB receptors. This inhibitory input removes inactivation of the calcium channels, and the rebound of the membrane potential sets off a burst of action potentials. In turn, the thalamic relay neurons provide excitatory inputs to the reticular neurons, which trigger another burst of firing in the reticular neurons. The resulting rhythmic and synchronous firing of thalamic relay neurons produces waves of excitatory postsynaptic potentials in dendrites of cortical neurons. These waves of depolarization show up on the EEG as rhythmic slow waves, a pattern indicating that the thalamus is unable to relay sensory information to the cortex (Figure 45-9). This synchronized pattern of EEG activity is associated with deep sleep (Chapter 47) and is also seen in pathological states in which thalamocortical transmission is blocked, such as coma or during certain types of seizures (see Chapter 46). In contrast, when the thalamus is in transmission mode (eg, during wakefulness), the desynchronized pattern of the EEG reflects ongoing sensory stimuli. During normal wakefulness the thalamus is kept in the transmission mode by the action of cholinergic inputs from the rostral pons and basal forebrain. The major cholinergic input to the thalamic relay nuclei is from the pedunculopontine and laterodorsal tegmental nuclei in the brain stem. These same nuclei, along with cholinergic neurons in the basal forebrain, innervate the reticular nucleus of the thalamus, reducing its activity and thus preventing it from hyperpolarizing the thalamic relay neurons during wakefulness.
Figure 45-10 The ascending arousal system consists of the axons of cell populations in the upper brain stem, hypothalamus, and basal forebrain. These pathways diffusely innervate the thalamus and cerebral cortex and keep the thalamus and cortex in a state in which they can respectively transmit and respond appropriately to incoming sensory information. Damage to either the main pathway in the brain stem or its branches in the thalamus or hypothalamus can cause loss of consciousness. RT = reticular nucleus of the thalamus; ILT = intralaminar thalamic nuclei. Damage to Either Branch of the Ascending Arousal System May Impair Consciousness Experimental lesion studies and clinical experience indicate that injury to either branch of the ascending arousal system—the pathway through the thalamus or the pathway through the hypothalamus—can impair consciousness (Figure 45-10). Transection of the brain stem below the level of the rostral pons does not affect the level of consciousness. Acute transections rostral to the level of the inferior colliculus invariably result in coma, a state of profound unarousability. Smaller lesions involving just the paramedian reticular formation of the midbrain are sufficient to produce this result, whereas large lesions of the lateral tegmentum of the upper brain stem do not cause coma. Lesions of the paramedian reticular formation up to the junction of the midbrain and the diencephalon damage axons arising from all components of the ascending arousal system and result in impairment of consciousness. Lesions of the posterior lateral hypothalamus interrupt the pathway through the hypothalamus. This injury results in profound slowing of the EEG and behavioral unarousability, even though the branch through the thalamus remains intact. Conversely, injury to the thalamus or its reticular input prevents the brain from achieving a desynchronized or wakeful state. If the injury is sufficiently severe, the EEG rhythm itself is lost. Bilateral Forebrain Damage May Cause Coma or Persistent Vegetative State or Be Symptomatic of Brain Death Coma may also be caused by bilateral impairment of the cerebral hemispheres. For example, bilateral subdural hematomas (blood clots in the space between the dura and the arachnoid membranes, usually as a result of head trauma) or multiple (or very large) brain tumors or associated areas of swelling can compress both hemispheres. More often, bilateral forebrain impairment results from a diffuse metabolic process, such as an imbalance of electrolytes or a lack of oxygen. If metabolic imbalance persists, permanent diffuse cortical injury may result. The large pyramidal neurons in the hippocampal formation and cerebral cortex (particularly laminae III and V) are the cells most severely damaged by inadequate oxygenation ( hypoxia ) or insufficient blood flow ( ischemia ). If many of these neurons are damaged there may not be sufficient numbers of remaining normal neurons to maintain a conscious state. After a period of 1 or 2 weeks of coma these patients enter a contentless wake-sleep cycle called a persistent vegetative state. They appear wakeful and may even eat food placed in the mouth, smile or cry, and fixate objects in the environment, similar to a hydrencephalic infant. Their actions, however, have no cognitive content and bear little relationship to events that surround them. The persistent vegetative state must be distinguished from brain death , in which all brain functions cease. Brain dead patients may have spinal level motor responses, which may include patterned activity such as withdrawal movements or even in rare instances sitting up or moving the arms (the Lazarus syndrome). Even so, there are no purposeful movements of the limbs, face, or eyes; no brain stem reflex responses to sensory stimulation (see below); and no respiratory movements.
Figure 28.1. The duration of sleep. (A) The duration of sleep each night in adults is normally distributed with a mean of 7.5 hours with a standard deviation of about 1.25 hours. Thus, about two-thirds of the population sleeps between 6.25 and 8.75 hours each night. (B) The duration of daily sleep as a function of age. (After Hobson, 1989 .) Sleep and Wakefulness Overview Sleep—which is defined behaviorally by the normal suspension of consciousness and electrophysiologically by specific brain wave criteria—consumes fully a third of our lives. Sleep occurs in all mammals, and probably all vertebrates. We crave sleep when deprived of it, and, to judge from animal studies, continued sleep deprivation can ultimately be fatal. Surprisingly, however, this peculiar state is not the result of a simple diminution of brain activity; rather, sleep is a series of precisely controlled brain states, and in some of these the brain is as active as it is when people are awake. The sequence of sleep states is governed by a group of brainstem nuclei that project widely throughout the brain and spinal cord. The reason for high levels of brain activity during some phases of sleep, the significance of dreaming, and the basis of the restorative effect of sleep are all topics that remain poorly understood. The clinical importance of sleep is obvious from the prevalence of sleep disorders (insomnias). Each year about 40 million Americans suffer from chronic sleep disorders and an additional 20 million experience occasional sleeping problems
Figure 28.2. The consequences of total sleep deprivation in rats. (A) In this apparatus, an experimental rat is kept awake because the onset of sleep (detected electroencephalographically) triggers movement of the cage floor. The control rat can thus sleep intermittently, whereas the experimantal animal cannot. (B) After two to three weeks of sleep deprivation, the experimental animals begin to lose weight, fail to control their body temperature, and eventually die. (After Bergmann et al., 1989.) Why Do Humans and Many Other Animals Sleep? To feel rested and refreshed upon awaking, most adults require 7–8 hours of sleep, although this number varies among individuals (Figure 28.1A). As a result, a substantial fraction of our lives is spent in this mysterious state. For infants, the requirement is much higher (about 16 hours a day), and teenagers need on average about 9 hours of sleep. As people age, they tend to sleep more lightly and for shorter times, although often needing about the same amount of sleep as in early adulthood (Figure 28.1B). Getting too little sleep creates a “sleep debt” that must be repaid in the following days. In the meantime, judgment, reaction time, and other functions are impaired. Drivers who fall asleep at the wheel are estimated to cause some 56,000 traffic accidents annually and 1,500 highway deaths. Sleep (or at least a physiological period of quiescence) is a highly conserved behavior that occurs in animals ranging from fruit flies to humans (Box A). This prevalence not withstanding, why we sleep is not well understood. Since animals are particularly vulnerable while sleeping, there must be advantages that outweigh this considerable disadvantage. Shakespeare characterized sleep as “nature's soft nurse,” noting the restorative nature of sleep. From a perspective of energy conservation, one function of sleep is to replenish brain glycogen levels, which fall during the waking hours. In keeping with this idea, humans andmany other animals sleep at night. Since it is generally colder at night, more energy would have to be expended to keep warm were we nocturnally active. Furthermore, body temperature has a 24-hour cycle, reaching a minimum at night and thus reducing heat loss. As might be expected, human metabolism measured by oxygen consumption decreases during sleep. Whatever the reasons for sleeping, in mammals sleep is evidently necessary for survival. For instance, rats completely deprived of sleep die in a few weeks (Figure 28.2). Sleep-deprived rats lose weight despite increasing food intake, and progressively fail to regulate body temperature. They also develop infections, suggesting an impairment of the immune system. In humans, lack of sleep leads to impaired memory and reduced cognitive abilities, and, if the deprivation persists, mood swings and even hallucinations. The longest documented period of voluntary sleeplessness is 264 hours (approximately 11 days), a record achieved without any pharmacological stimulation. The young man involved recovered after a few days, during which he slept only somewhat more than normal, and seemed none the worse for wear
Figure 28.3. Rhythm of waking (blue lines) and sleeping (red lines) of a volunteer in an isolation chamber with and without cues about the day-night cycle. Numbers represent the mean ± standard deviation of a complete waking/sleeping cycle during each period (blue triangles represent times when the rectal temperature was maximum). (After Aschoff, 1965, as reproduced in Schmidt et. al., 1983.) The Circadian Cycle of Sleep and Wakefulness Human sleep occurs with circadian ( circa = about, and dia = day) periodicity, and biologists interested in circadian rhythms have explored a number of questions about this daily cycle. What happens, for example, when individuals are prevented from sensing the cues they normally have about night and day? This question has been answered by placing volunteers in an environment (caves or bunkers have sometimes been used) without external cues about time ( Figure 28.3 ). During a five-day period of acclimation that included social interactions, meals at normal times, and temporal cues (radio, TV), the subjects arose and went to sleep at the usual times and maintained a 24-hour sleep-wake rhythm. After removing these cues, however, the subjects awakened later each day, and the cycle of sleep and wakefulness gradually lengthened to about 28 hours instead of the normal 24. When the volunteers were returned to a normal environment, the 24-hour cycle was rapidly restored. Thus, humans (and many other animals; see Box B ) have an internal “clock” that continues to operate in the absence of any external information about the time of day; under these conditions, the clock is said to be “free running.”
Figure 28.4. Anatomical underpinnings of circadian rhythms. (A) The hypothalamus, showing the location of the suprachiasmatic nucleus (SCN), which in mammals is the primary “biological clock.” The name “suprachiasmatic” derives from the location of the nucleus just above the optic chiasm. (B) Diagram of the pathway from the suprachiasmatic nucleus to the pineal gland. Presumably, circadian clocks evolved to maintain appropriate periods of sleep and wakefulness in spite of the variable amount of daylight and darkness in different seasons and at different places on the planet. To synchronize physiological processes with the day-night cycle (called photoentrainment), the biological clock must detect decreases in light levels as night approaches. The receptors that sense these light changes are, not surprisingly, in the outer nuclear layer of the retina; although removing the eye abolishes photoentrainment. The detectors are not, however, the rods or cones. Rather, these poorly understood cells lie within the ganglion and amacrine cell layers of the primate and murine retinas, and project to the suprachiasmatic nucleus (SCN) of the hypothalamus, the site of the circadian control of homeostatic functions generally (Figure 28.4A). These peculiar retinal photoreceptors contain a novel photopigment called melanopsin. Perhaps the most convincing evidence of the SCN's role as a sort of master biological clock is that its removal in experimental animals abolishes their circadian rhythm of sleep and waking. The SCN also governs other functions that are synchronized with the sleep-wake cycle, including body temperature (see Figure 28.3), hormone secretion, urine production, and changes in blood pressure. The cellular mechanisms of circadian control are summarized in Box B. Activation of the superchiasmatic nucleus evokes responses in neurons whose axons descend to the preganglionic sympathetic neurons in the lateral horn of the spinal cord (Figure 28.4B). These cells, in turn, modulate neurons in the superior cervical ganglia whose postganglionic axons project to the pineal gland(pineal means shaped like a pinecone) in the midline near the dorsal thalamus. The pineal gland synthesizes the sleep promoting neurohormone melatonin ( N -acetyl-5-methoxytryptamine) from tryptophan, and secretes it into the bloodstream to help modulate the brainstem circuits that ultimately govern the sleep-wake cycle (see p. 615 ff.). Predictably, melatonin synthesis increases as light decreases and reaches it maximal level between 2:00 and 4:00 a.m. In the elderly, the pineal gland calcifies and less melatonin is produced, perhaps explaining why older people sleep fewer hours and are more often afflicted with insomnia
Figure 28.5. EEG recordings during the first hour of sleep. The waking state with the eyes open is characterized by high-frequency (15–60 Hz), low-amplitude activity (~30 μV) activity. This pattern is called beta activity. Descent into stage I non-REM sleep is characterized by decreasing EEG frequency (4–8 Hz) and increasing amplitude (50–100 μV), called theta waves. Descent into stage II non-REM sleep is characterized by 10–15 Hz oscillations (50–150 μV) called spindles, which occur periodically and last for a few seconds. Stage III non-REM sleep is characterized by slower waves at 2–4 Hz (100–150 μV). Stage IV sleep is defined by slow waves (also called delta waves) at 0.5–2 Hz (100–200 μV). After reaching this level of deep sleep, the sequence reverses itself and a period of rapid eye movement sleep, or REM sleep, ensues. REM sleep is characterized by low-voltage, high-frequency activity similar to the EEG activity of individuals who are awake. (Adapted from Hobson, 1989 .) Stages of Sleep The normal cycle of sleep and wakefulness implies that, at specific times, various neural systems are being activated while others are being turned off. A key to the neurobiology of sleep is therefore to understand the various stages of sleep. For centuries—indeed up until the 1950s—most people who thought about sleep considered it a unitary phenomenon whose physiology was essentially passive and whose purpose was simply restorative. In 1953, however, Nathaniel Kleitman and Eugene Aserinksy showed, by means of electroencephalographic (EEG) recordings from normal subjects, that sleep actually comprises different stages that occur in a characteristic sequence ( Figures 28.5 and 28.6 ). Humans descend into sleep in stages that succeed each other over the first hour or so after retiring ( Figure 28.5 ). These characteristic stages are defined primarily by electroencephalographic criteria ( Box C ). Initially, during “drowsiness,” the frequency spectrum of the electroencephalogram (EEG) is shifted toward lower values and the amplitude of the cortical waves slightly increases. This drowsy period, called stage I sleep , eventually gives way to light or stage II sleep , which is characterized by a further decrease in the frequency of the EEG waves and an increase in their amplitude, together with intermittent high-frequency spike clusters called sleep spindles . Sleep spindles are periodic bursts of activity at about 10–12 Hz that generally last 1 or 2 seconds and arise as a result of interactions between thalamic and cortical neurons. In stage III sleep , which represents moderate to deep sleep, the number of spindles decreases, whereas the amplitude of low-frequency waves increases still more. In the deepest level of sleep, stage IV sleep , the predominant EEG activity consists of low frequency (1–4 Hz), high-amplitude fluctuations called delta waves , the characteristic slow waves for which this phase of sleep is named. The entire sequence from drowsiness to deep stage IV sleep usually takes about an hour. These four sleep stages are called non-rapid eye movement (non-REM) sleep , and its most prominent feature is the slow-wave (stage IV) sleep . It is most difficult to awaken people from slow-wave sleep; hence it is considered to be the deepest stage of sleep. Following a period of slow-wave sleep, however, EEG recordings show that the stages of sleep reverse to reach a quite different state called rapid eye movement , or REM, sleep . In REM sleep, the EEG recordings are remarkably similar to that of the awake state (see Figure 28.5 ). After about 10 minutes in REM sleep, the brain typically cycles back through the non-REM sleep stages. Slow-wave sleep usually occurs again in the second period of this continual cycling, but not during the rest of the night (see Figure 28.6 ). On average, four additional periods of REM sleep occur, each having longer durations. In summary, the typical 8 hours of sleep experienced each night actually comprise several cycles that alternate between non-REM and REM sleep, the brain being quite active during much of this supposedly dormant, restful time. For reasons that are not clear, the amount of REM sleep each day decreases from about 8 hours at birth to 2 hours at 20 years to only about 45 minutes at 70 years of age.
Figure 28.6. Physiological changes in a male volunteer during the various sleep states in a typical 8-hour period of sleep (A). The duration of REM sleep increases from 10 minutes in the first cycle to up to 50 minutes in the final cycle; note that slow-wave (stage IV) sleep is attained only in the first two cycles. (B) The upper panels show the electro-oculogram (EOG) and the lower panels show changes in various muscular and autonomic functions. Movement of neck muscles was measured using an electromyogram (EMG). Other than the few slow eye movements approaching stage I sleep, all other eye movements evident in the EOG occur in REM sleep. The greatest EMG activity occurs during the onset of sleep and just prior to awakening. The heart rate (beats per minute) and respiration (breaths per minute) slow in non-REM sleep, but increase almost to the waking levels in REM sleep. Finally, penile erection occurs only during REM sleep. (After Schmidt et al., 1983.) Physiological Changes in Sleep States A variety of physiological changes take place during the different stages of sleep (see Figure 28.6). Periods of non-REM sleep are characterized by decreases in muscle tone, heart rate, breathing, blood pressure, and metabolic rate. All these parameters reach their lowest values during slow-wave sleep. In non-REM sleep, body movements are reduced compared to wakefulness, although it is common to change sleeping position (tossing and turning). Periods of REM sleep, in contrast, are characterized by increases in blood pressure, heart rate, and metabolism to levels almost as high as those found in the awake state. In addition, REM sleep, as the name implies, is characterized by rapid, rolling eye movements, paralysis of large muscles, and the twitching of fingers and toes. Penile erection also occurs during REM sleep, a fact that is clinically important in determining whether a complaint of impotence has a physiological or psychological basis. Interestingly, REM sleep is found only in mammals (and juvenile birds) Despite the similar EEG recordings obtained in REM sleep and wakefulness, the two conditions are clearly not equivalent brain states. Unlike wakefulness, REM sleep is characterized by dreaming, visual hallucinations, increased emotion, lack of self-reflection, and a lack of volitional control. Since most muscles are inactive during REM sleep, the motor responses to dreams are relatively minor (sleepwalking actually occurs during non-REM sleep and is not accompanied or motivated by dreams). This relative paralysis arises from increased activity in GABAergic neurons in the pontine reticular formation that contact lower motor neuron circuitry in the spinal cord. Similarly, activity of descending inhibitory projections from the pons to the dorsal column nuclei causes a diminished response to somatic sensory stimuli during REM sleep. Taken together, these observations have led to the aphorism that non-REM sleepis characterized by an inactive brain in an active body, whereas REM sleep is characterized by an active brain in an inactive body.m
Figure 28.7. Activation of specific neural circuits triggers sleep and wakefulness. (A) Electrical stimulation of the cholinergic neurons near the junction of pons and midbrain (the reticular activating system) causes a sleeping cat to awaken. (B) Electrical stimulation of the thalamus causes an awake cat to fall asleep. Graphs show EEG recordings before and during stimulation. Neural Circuits Governing Sleep From the descriptions of the physiological changes that occur during sleep, it is clear that periodic excitatory and inhibitory changes occur in many neural circuits. What follows is a brief overview of the still incompletely understood circuits and their interactions that govern sleeping and wakefulness. One of the first clues about the circuits involved in the sleep-wake cycle was provided in 1949 by Horace Magoun and Giuseppe Moruzzi. They found that electrically stimulating a group of cholinergic neurons that lies near the junction of the pons and midbrain causes a state of wakefulness and arousal (the name “reticular activating system” was therefore given to this region of the brainstem) ( Figure 28.7A ). This observation implied that wakefulness requires a special mechanism, not just the presence of adequate sensory experience. About the same time, the Swiss physiologist Walter Hess found that stimulating the thalamus with low-frequency pulses in an awake animal produced a slow-wave sleep as measured by cortical EEG activity ( Figure 28.7B ). These important experiments showed that sleep entails a patterned interaction between the thalamus and cortex. The saccade-like rapid eye movements that define REM sleep arise because, in the absence of external visual stimuli, endogenously generated signals from the pontine reticular formation are transmitted to the motor region of the superior colliculus. As described in Chapter 20 , collicular neurons project to the paramedialpontine reticular formation (PPRF), which coordinates timing and direction of eye movements. REM sleep is also characterized by EEG waves that originate in the pontine reticular formation and propagate through the lateral geniculate nucleus of the thalamus to the occipital cortex. These pontine-geniculo-occipital (PGO) waves therefore provide a useful marker for the beginning of REM sleep; they also indicate yet another neural network by which brainstem nuclei can activate the cortex. As already noted, the function of these eye movements is not known. Human MRI and PET studies have also been used to compare the activity in the awake state and in REM sleep. Activity in the amygdala, parahippocampus, pontine tegmentum, and anterior cingulate cortex are all increased in REM sleep, whereas activity in the dorsolateral prefrontal and posterior cingulate cortices is decreased ( Figure 28.8 ). The increase in limbic system activity, coupled with a marked decrease in the influence of the frontal cortex during REMsleep, presumably explains some characteristics of dreams (e.g., their emotionality and the often inappropriate social content; see Chapter 26 for the normal role of the frontal cortex in determining behavior that is appropriate to circumstances in the waking state). Most investigators now agree that a key component of the reticular activating system is a group of cholinergic nuclei near the pons-midbrain junction , which project to thalamocortical neurons. The relevant neurons in these nuclei are characterized by high discharge rates during waking and in REM sleep, and by quiescence during non-REM sleep. When stimulated, they cause “desynchronization” of the electroencephalogram (that is, a shift of EEG activity from high-amplitude, synchronized waves to lower-amplitude, higher-frequency, desynchronized ones) (see Figure 28.7A ). These features imply that activity of cholinergic neurons in the reticular activating system is a primary cause of wakefulness and REM sleep, and that their relative inactivity is important for producing non-REM sleep. Activity of these neurons is not, however, the only cellular basis of wakefulness; also involved are noradrenergic neurons of the locus coeruleus and serotonergic neurons of the raphe nuclei . The cholinergic and monoaminergic networks responsible for the awake state are periodically inhibited by neurons in the ventrolateral preoptic nucleus (VLPO) of the hypothalmus (see Figure 28.4 ). Thus, activation of VLPO neurons contributes to the onset ofsleep, and lesions of VLPO neurons produce insomnia. These complex interactions and effects are summarized in Table 28.1 . Both monoaminergic and cholinergic systems are active during the waking state and suppress REM sleep. Thus, decreased activity of the monoaminergic and cholinergic systems leads to the onset of non-REM sleep. In REM sleep, the monoaminergic and serotonin neurotransmitter levels markedly decrease, while the cholinergic levels increase to approximately the levels found in the awake state. With so many systems and transmitters involved in the different phases of sleep, it is clear that a variety of drugs can influence the sleep cycle
Figure 28.8. Diagram showing cortical regions whose activity is increased or decreased during REM sleep. (After Hobson et al., 1998.)
Figure 28.10. Thalamocortical feedback loop and the generation of sleep spindles. (A) Diagram showing excitatory (+) and inhibitory (-) connections between thalamocortical cells (Th-Cx), pyramidal cells in the cortex (Cx), and thalamic reticular cells (RE), which provide the basis for sleep spindle generation. Inputs into Th-Cx and RE cells are not shown. (B) EEG recordings illustrating sleep spindles. The bottom trace is filtered to illustrate these spindles. (C) The responses from individual RE, Th-Cx, and Cx cells during the generation of the middle spindle [box in (B)]. Note that when the GABAergic RE cells are in the bursting mode they hyperpolarize the Th-Cx cells (arrows), causing them to burst (arrowheads) (see Figure 28.9 ). This bursting behavior is apparent as spikes in Cx cells, and as spindles in EEG recordings. (After Steriade et al., 1997.) Thalamocortical Interactions More generally, these effects on mental status are achieved by modulating the rhythmicity of interactions between the thalamus and the cortex. Thus, the activity of several ascending systems from the brainstem decreases both the rhythmic bursting of the thalamocortical neurons and the related synchronized activity of cortical neurons (hence the diminution and ultimate disappearance of high-voltage, low-frequency slow waves during waking and REM sleep). To appreciate how different sleep states reflect modulation of thalamocortical cell activity, some understanding of the electrophysiological responses of these neurons is useful. As might be expected from the summary in Table 28.1 , thalamocortical neurons receive ascending projections from the locus coeruleus (noradregeneric), raphe nuclei (serotonin), and reticular activating system (acetylcholine), and, as their name implies, project to cortical pyramidal cells. The primary characteristic of thalamocortical neurons is that they can be in one of two stable electrophysiological states ( Figure 28.9 ): an intrinsic oscillatory state , and a tonically active state that is generated when neurons are depolarized, as occurs when the reticular activating system generates wakefulness(see Figure 28.7 ). In the tonic firing state, thalamocortical neurons transmit information to the cortex that matches the spike trains encoding peripheral stimuli. In contrast, when thalamocortical neurons are in the oscillatory/bursting mode, the neurons in the thalamus become synchronized with those in the cortex, essentially “disconnecting” the cortex from the outside world. During slow-wave sleep, when EEG recordings show the lowest frequency and the highest amplitude, this disconnection is maximal. The oscillatory state of thalamocortical neurons can be transformed into the tonically active state by activating the cholinergic or monoaminergic projections from the brainstem nuclei ( Figure 28.10 ). Moreover, the oscillatory state is stabilized by hyperpolarizing the relevant thalamic cells. Such hyperpolarization can occur as a consequence of stimulation by GABAergic neurons in the thalamic reticular nucleus. These neurons receive ascending information from the brainstem and descending projections from cortical neurons, and they contact the thalamocortical neurons. When neurons in the reticular nucleus undergo a burst of activity, they cause thalamocortical neurons to generate short bursts of action potentials, which in turn generate spindle activity in cortical EEG recordings (indicating a lighter sleep state; see Figure 28.5 ). These admittedly complex interactions between the cortex and the relevant subcortical systems are summarized in Figure 28.11 . In brief, the control of sleepand wakefulness depends on brainstem and hypothalamic modulation of the thalamus and cortex. It is this thalamocortical loop that generates the EEG signature of mental function along the continuum of deep sleep to high alert. The major components of the brainstem modulatory system are the cholinergic nuclei of the pons-midbrain junction, the noradrenergic cells of the locus coeruleus in the pons, the serotonergic raphe nuclei, and GABAergic neurons in the VLPO. All of these nuclei can exert direct as well as indirect effects on the overall cortical acitivity that determines sleep and wakefulness
Figure 47-3 The patterns of activity of key cell groups during waking and slow wave and REM sleep are illustrated in these samples of electrode recordings from a cat. Each vertical line represents an action potential. EEG = sensorimotor electroencephalogram; EMG = dorsal neck electromyogram; EOG = eye movement; LGN = lateral geniculate nucleus electrode showing ponto-geniculo-occipital (PGO) spike activity during REM sleep. Cortical and thalamic cells. The rate of firing of cortical and thalamic cells increases slightly during non-REM sleep and again in REM sleep. These bursts are synchronized with individual waves of the EEG (sleep spindles and slow waves). Non-REM-on cells. These cells are located in the anterior hypothalamus and the basal forebrain region and participate in the generation of non-REM sleep. REM-waking-on cells. These cells predominate in the brain stem reticular formation and are active in both waking and REM sleep. Many excite motor neurons; others control the EEG. PGO-on cells. These pontine cells fire in high-frequency bursts before PGO waves recorded in the lateral geniculate nucleus. REM-off cells. These cells include noradrenergic, adrenergic, and serotonergic cells in the brain stem and histaminergic cells in the forebrain. Most skeletal motor neurons have a similar pattern. REM-on cells. These cells are maximally active in REM sleep and are involved in various aspects of this state. Different Neural Systems Promote Arousal and Sleep In their classic study, Moruzzi and Magoun demonstrated that electrical stimulation of the midbrain reticular formation promotes the waking state. Conversely, damage to this region produces a comatose state followed by a long-term reduction in waking. Moruzzi and his colleague also found that the midbrain reticular formation is normally inhibited by a system in the medulla. Disconnecting this medullary inhibitory region, by transecting the brain stem at the level of the pons just behind the midbrain (the midpontine-pretrigeminal transection), produces an animal whose forebrain spends most of its time “awake.” Stimulation of the posterior hypothalamus, rostral to the midbrain, produces an arousal resembling that produced by stimulation of the midbrain. This hypothalamic arousal is partly mediated by histaminergic neurons that connect with cells in the brain stem below and with cells in the forebrain above. Destruction of the histaminergic neurons in the posterior hypothalamus increases sleep. Similarly, blockade of histaminergic outputs with antihistaminic drugs promotes sleep. Whereas the posterior hypothalamus induces arousal, electrical stimulation of the anterior hypothalamus and the adjacent basal forebrain region rapidly induces sleep, and lesions produce a long-lasting reduction in sleep. The sleep-inducing action of these regions is thought to be mediated by GABA-ergic inhibitory neurons called the non-REM-on cells (Figure 47-3). These cells are thought to produce sleep by inhibiting the histaminergic cells in the posterior hypothalamus as well as cells of the nucleus reticularis pontis oralis in the midbrain that mediate arousal. They are maximally active in non-REM sleep and inactive during waking and REM sleep. Many non-REM-on cells are activated by heat and thus may mediate the sleep-inducing effects of elevated temperature. Non-REM Sleep Is Regulated by Interacting Sleep-Inducing and Arousal Mechanisms Non-REM sleep is characterized by EEG spindles and slow waves that are produced by synchronized synaptic potentials in cortical neurons. These synchronized synaptic potentials are generated by the rhythmic firing of thalamic relay neurons that project to the cortex. The rhythmic firing of the relay neurons is a result of the actions of GABA-ergic inhibitory neurons in the nucleus reticularis, a nucleus that forms a shell around the thalamus (Chapter 45). The GABA-ergic neurons of the nucleus reticularis generate a novel type of action potential that is a key event in the sequence of membrane currents generating EEG spindles. Calcium is admitted into the reticularis cells through voltage-sensitive membrane channels that open only when the cells are hyperpolarized. During the calcium spike the cells produce a burst of action potentials. After the calcium spike the membrane currents return the cells to the hyperpolarized state, restarting the process. This cycle of calcium influx followed by hyperpolarization results in rhythmic firing. The GABA released by the reticularis neurons hyperpolarizes thalamocortical neurons, and this hyperpolarization results in a rebound low-threshold calcium spike in the thalamocortical cells. The rhythmic firing of the thalamocortical cells (Figure 47-3) produces synchronized postsynaptic potentials in cortical neurons and it is these potentials that cause the spindle waves seen in the sleep EEG. The rhythmic firing of thalamic and cortical cells occludes the transmission of sensory information through the thalamus and the cortex. REM Sleep Is Regulated Primarily by Nuclei Located at the Junction of the Midbrain and Pons During both REM sleep and waking the EEG spindles and slow waves are blocked. During REM sleep there also are PGO waves, muscle atonia, and phasic motor action. How do these events come about? We first consider EEG voltage reduction, the phenomenon whereby EEG spindles and slow waves are blocked. An important component of the midbrain arousal system arises from cholinergic neurons in the midbrain and the adjacent dorsal pons (Chapter 45). Many of these cholinergic cells and cells adjacent to them are maximally active during waking and REM sleep, and their activity contributes to the blocking of the slow waves of the EEG (Figure 47-3). Acetylcholine (ACh) and other transmitters released by these cells depolarize the GABA-ergic inhibitory neurons in the reticularis nucleus. This depolarization prevents the hyperpolarization that activates the low-threshold Ca2+ channels, which in turn initiate the rhythmic firing of the reticular neurons. In the absence of rhythmic firing of the reticular neurons, the thalamocortical relay cells fire only asynchronously, and this asynchronous activity results in the low-voltage EEG characteristic of waking and REM sleep. Other neuronal machinery important for REM sleep resides in the nucleus reticularis pontis oralis , which extends from the rostral pons to the caudal midbrain (Figure 47-4). Bilateral destruction of this nucleus eliminates REM sleep for extended periods. Many of the neurons in the nucleus reticular pontis oralis critical for REM sleep receive input from cholinergic cells located dorsal and lateral to them. Microinjection of the ACh agonist carbachol into the nucleus elicits extended periods of REM sleep Three classes of neurons in the nucleus reticularis pontis oralis are of particular interest. The cholinergic PGO-on cells fire in bursts to initiate PGO spikes in cells of the lateral geniculate nucleus. Destruction of PGO-on cells blocks the PGO spikes but does not interfere with other aspects of REM sleep. Conversely, stimulation of this area produces PGO spikes even in the absence of REM sleep. The PGO-on cells are regulated by serotonergic REM-off cells in the raphe nuclei of the brain stem. The firing of the REM-off cells during waking activity (Figure 47-3) is thought to hyperpolarize and thereby block the burst firing of PGO-on cells. In the transition from non-REM to REM sleep the cessation of activity in the REM-off cells allows the PGO cells to begin discharging in bursts, generating PGO waves. Noradrenergic neurons in the locus ceruleus and histaminergic neurons in the posterior hypothalamus have a pattern of activity that is similar to that of the serotonergic REM-off cells. Cessation of activity in these three cell groups may contribute to changes in autonomic tone, EEG, and muscle tone during REM sleep. Another class of cells in the nucleus reticularis pontis oralis, the REM-waking-on cells , fire during active waking as well as during REM sleep (Figure 47-3) and fire at lower rates during non-REM sleep. Some of these cells project to the motor neurons in the spinal cord, and others project to the motor neurons that drive the extraocular muscles. The burst firing of these cells during waking mediates movements of the head, the neck, the limbs, and the eyes. Their firing during REM sleep produces rapid eye movements and muscle twitches, breaking through the concurrent inhibition of motor neurons. The third class of cells in the nucleus reticularis pontis oralis, the REM-on cells , show little or no activity during waking and non-REM sleep but have high levels of activity in REM sleep (Figure 47-3). Although few in number, these cells play a key role in REM sleep control. One subtype of these cells is GABA-ergic and is responsible for the inhibition of activity in serotonergic and noradrenergic cells during REM sleep; another subtype, possibly glutamatergic, is responsible for the loss of muscle tone in REM sleep.
Figure 47-4 The major regions of the brain stem and forebrain involved in sleep control are shown in this sagittal section. Nuclei in the pontine region critical for triggering REM sleep are shown in a coronal section through the center of the region (upper right). Stimulation of neurons in the nucleus reticularis pontis oralis/caudalis (RPO/RPC) region produces various characteristics of REM sleep. Depending on their exact size and location, bilateral lesions within this region completely block REM sleep or block components of REM sleep. CG = central gray; LC = locus ceruleus; LDT = lateral-dorsal tegmental nucleus; PPN = pedunculopontine nucleus; PT = pyramidal tract; 5ME = mesencephalic nucleus of the trigeminal nerve; 7G = genu of the seventh cranial nerve; 6 = nucleus of the sixth nerve.
Figure 47-5 A simplified model of the possible connections between the key neuronal groups that control REM sleep. These cell groups are shown on a sagittal section of the brain stem of the cat. Muscle tone is lost during REM sleep because motor neurons are actively inhibited. The circuitry mediating inhibition of muscle tone resides in the pons and medulla. A small lesion within a portion of the nucleus reticularis pontis oralis critical for REM sleep releases motor activity during REM sleep. Cats with this lesion have normal non-REM sleep episodes, but when they enter REM sleep they raise their heads, walk, and engage in a variety of vigorous motor activities. A similar syndrome can be produced by lesions of the medial medulla. The suppression of muscle tone in REM sleep is mediated by interconnections between several types of REM-on neurons. Abnormal activity in these neurons during waking is believed to cause a sudden loss of muscle tone ( cataplexy ), one of the primary symptoms of narcolepsy. Excessive activity in these neurons during sleep may contribute to a collapse of the airway resulting from reduction in muscle tone ( sleep apnea ). Insufficient activity in these neurons during sleep may cause a release of motor activity during REM sleep, during which dreams are acted out (the REM sleep behavior disorder). We shall consider these sleep disorders in greater detail in the next chapter. The connections thought to mediate the interactions between the key groups of neurons that mediate REM sleep are illustrated in Figure 47-5. During REM sleep these cell groups cause muscle tone to be turned off and the high-voltage electroencephalogram (EEG) of slow wave sleep to be replaced by the low-voltage EEG of REM sleep. A key event in this process is the activation of GABA-ergic neurons in the pons. The reason for the activation of GABA-ergic cells is not known. The GABA activation causes the inhibition of noradrenergic and serotonergic neurons and the activation (or disinhibition) of cholinergic neurons in the pons. Muscle tone is turned off by a descending system. The cholinergic neurons of the pons excite glutamatergic neurons in the pons. The glutamatergic neurons project to the medulla, where they terminate on interneurons that release glycine onto motor neurons. This release of glycine hyperpolarizes the motor neurons, producing the motor paralysis of REM sleep. Reduced release of serotonin and norepinephrine may also contribute to muscle tone reduction by disfacilitating motor neurons. A pontine system with ascending connections causes the reduction in EEG voltage during REM sleep. Some cholinergic cells and adjacent noncholinergic cells activated during REM sleep project to GABA-ergic cells in the thalamus. The release of acetylcholine by these cells blocks the burst firing mode of these neurons. It is the burst firing mode that produces high voltage waves in the EEG. ACh = acetylcholine; NE = norepinephrine; 5-HT = serotonin.
The Possible Functions of REM Sleep and Dreaming Despite this wealth of descriptive information about the stages of sleep, the functional purposes of the various sleep states are not known. Whereas most sleep researchers accept the idea that the purpose of non-REM sleep is at least in part restorative, the function of REM sleep remains a matter of considerable controversy. A possible clue about the purposes of REM sleep is the prevalence of dreams during these epochs of the sleep cycle. The occurrence of dreams can be tested by waking volunteers during either non-REM or REM sleep and asking them if they were dreaming. Subjects awakened from REM sleep recall elaborate, vivid, hallucinogenic and emotional dreams, whereas subjects awakened during non-REM sleep report fewer dreams, which, when they occur, are more conceptual, less vivid and less emotion-laden. Dreams have been studied in a variety of ways, perhaps most notably within the psychoanalytic framework of revealing unconscious thought processes considered to be at the root of neuroses. Sigmund Freud's The Interpretation of Dreams , published in 1900, speaks eloquently to the complex relationship between conscious and unconscious mentation. It is by no means agreed upon, however, that dreams have the deep significance that Freud and others have given them, and the psychoanalytic interpretation of dreams has recently fallen into disfavor. Nevertheless, most people probably give some credence to the significance of dream content, at least privately. In more recent studies of dreams, about 65% are associated with sadness, apprehension, or anger; 20% with happiness or excitement; and, somewhat surprisingly, only 1% with sexual feelings or acts. Adding to the uncertainty about the purposes of REM sleep and dreaming is the fact that deprivation of REM sleep in humans for as much as two weeks has little or no obvious effect on behavior. Such studies have been done by waking volunteers whenever their EEG recordings showed the characteristic signs of REM sleep. Although the subjects in these experiments compensate for the lack of REM sleep by having more of it after the period of deprivation has ended, they suffer no obvious adverse effects. Similarly, patients taking certain antidepressants (MAO inhibitors) have little or no REM sleep, yet show no obvious ill effects, even after months or years of treatment. The apparent innocuousness of REM sleep deprivation contrasts markedly with the effects of total sleep deprivation (see earlier). The implication of these several findings is that we can get along without REM sleep, but need non-REM sleep in order to survive. Several general hypotheses about dreams and REM sleep have been advanced. Francis Crick (of DNA fame) and Grahame Mitchison suggested that dreams act as an “unlearning” mechanism, whereby certain modes of neural activity are erased by random activation of cortical connections. The hypothesis is based on the idea that the human brain represents information by the activity of sets of neuronal networks that are widely distributed and overlapping. In computers, neural network architectures are subject to unwanted patterns of activity that can indeed degrade rather than enhance the information content of the system. By analogy, these “parasitic” modes of activity might be unwanted thoughts or erroneous information, which, if not expunged, could become the basis for obsession, paranoia, or other pathologies of thought that prevent the “system” from working as efficiently as it should. In a different vein, Michel Jouvet proposed that dreaming reinforces behaviors not commonly encountered during the awake state (aggression, fearful situations) by rehearsing them while dreaming. Yet another hypothesis is that REM sleep and dreams are involved in the transfer of memories between the hippocampus and neocortex. Finally, it has been suggested that dreaming is simply an incidental consequence of REM sleep. None of these ideas are generally accepted. In short, the questions of why we have REM sleep and why we dream remain unanswered, as are questions about consciousness per se (Box D). The Functions of Sleep and Dreaming Are Not Yet Known Various Theories of the Function of Sleep Have Been Proposed It is likely that sleep is functionally important because it has persisted throughout the evolution of mammals and birds (and is perhaps present in lower forms as well). Its importance is also indicated by the rebound of sleep after total sleep deprivation and the rebound of slow-wave or REM sleep after selective deprivation of these stages, as well as by the functional impairments after sleep loss. Rats that have been chronically deprived of sleep for 2-3 weeks die. Rats deprived only of REM sleep survive about twice as long. Despite these considerations, there is no agreement on why sleep is important. Several ideas have been advanced, but they all have been challenged by contrary evidence or shown to have limited generality. Conservation of Metabolic Energy The idea that sleep conserves energy is supported by the fact that humans and laboratory animals increase their food intake during sleep deprivation. However, the metabolic rate during sleep is only 15% less than during quiet wakefulness; the energy loss of a sleepless night could be compensated by only a small amount of food. The idea that sleep enforces body rest is supported by the fact that small mammals tend to sleep the most. These animals have high energy demands for thermoregulation and locomotion but low energy reserves. However, rest is possible during wakefulness. Why suffer a form of rest with impaired vigilance? Nevertheless, rest without sleep leaves us sleepy. Because we feel refreshed after sleep, the idea that sleep is restitutive is intuitively appealing, but precisely what may get restored during sleep has not been identified. Cognition Humans show little or no physiological impairment after several days of sleep deprivation but do show impaired intellectual performance. Thus, it has been proposed that sleep serves higher mental functions. However, the performance deficit could result from a homeostatic pressure to enter sleep rather than from impaired intellectual capacity. Most of the deficits can be reversed by strong motivation or analeptic drugs. Thermoregulation There are strong indications that sleep has thermoregulatory functions. Body and brain temperatures are usually reduced during sleep. Heating the hypothalamus induces sleep in animals, and body heating prior to sleep increases subsequent slow wave sleep in humans. Rats that are chronically deprived of sleep show an increase in preferred ambient temperature of 10°C or more. These facts suggest that sleep has cooling functions. On the other hand, rats deprived of sleep for two weeks show a significant drop in body temperature in spite of a doubling of metabolic rate, suggesting that sleep may also have a role in heat retention. Modern Research Has Increased Our Knowledge About Dreaming When Kleitman, Aserinsky, and Dement studied the REM and non-REM phases of sleep they also studied the relation of each phase to dreaming. They awakened subjects during REM and non-REM sleep and asked them to describe any dreams they were having. Dreams were far more likely to be recalled when subjects were awakened from REM sleep (74% or more of awakenings) than from non-REM sleep (less than 10% of awakenings). The preponderance of reports after REM sleep led to the belief that dreaming occurs exclusively during REM sleep (the non-REM reports were dismissed as recall from earlier REM sleep). It was widely believed that the physiological basis of dreaming would soon be discovered. This expectation has not yet been realized. Although REM sleep is the phase from which dreams may be most reliably elicited, REM sleep is not necessary for dreaming. In almost all more recent studies the frequency of dream recall after non-REM sleep is higher than in the earliest studies—as high as 70% in some studies. Many dream reports are elicited on awakenings from non-REM sleep that occurs before the first REM phase of the night; these dream reports do not represent recall from REM periods earlier in the night. In fact, dream reports have also been elicited from subjects at the onset of sleep and from subjects lying quietly awake in a darkened room. Reports of non-REM dreams tend to be shorter, less vivid, less emotional, and more coherent than reports of REM dreams. But there are no qualitative differences between REM and non-REM reports of the same length. Thus, the major difference is that REM dreams tend to be longer than non-REM dreams. REM sleep is not sufficient for dreaming, which varies with cognitive abilities as well as sleep stages. Even though children have abundant REM sleep, they rarely report thematically organized dreams before ages 7-9 years; appearance of organized dreams is correlated with the development of visuospatial skills. Dreaming may be absent in a variety of patients with neurological damage who nevertheless show REM sleep. According to Sigmund Freud, dreams are disguised manifestations of strong, unacceptable, unconscious wishes. Much of the impetus for modern dream research was motivated by the interest in the psychoanalytic interpretation of dream content. Although modern dream research has identified the phases of sleep when dreams are likely to occur—and has thus facilitated fresh recall of dreams—it has no special procedures for uncovering hidden meanings and has therefore contributed little to identifying unconscious determinants of dreams. Nor has it had much success in specifying other sources of dream content. However, it has shown that dream content is not greatly influenced by external environmental stimuli during sleep. Even on the relatively infrequent occasions when external stimuli are incorporated into dreams, they usually appear to be incidental to the dream narrative. In one study subjects had P.946 their eyelids taped open and had various objects presented to them during REM sleep. None of the objects appeared in any of the subsequently reported REM dreams. Systemic stimulation of one or another internal homeostatic system also does not have a consistent effect on dream content. For example, restricting fluid intake over a 24-hour period does not routinely lead to the appearance of thirst in REM dream reports, and only one-third of dream reports following fluid restriction contain any references to drinking. Although full or partial penile erections occur in 80-95% of REM periods, only 12% of men's dreams contain manifestly sexual content. Moreover, patients with spinal cord transections that preclude genital sensations report dreams with orgasmic imagery. Even experiences that immediately precede sleep do not appear to affect our dreams consistently. For example, viewing violent films does not reliably produce violent dreams, nor do pornographic films increase sexual dreams substantially. Although modern dream research has contributed relatively little to uncovering hidden meanings in dreams, it has greatly enlarged the empirical information on the phenomenology and correlates of dreams by systematically collecting detailed dream reports in the laboratory. Dreams are not kaleidoscopic jumbles of visual fragments, but are organized thematically and perceptually. The old view that dreams occur in an instant is not consistent with the correlation between the duration of the REM period, the length of the dream report, and the actual time taken by subjects to reenact a dream experience after they have been awakened. Although threads of specific content or personal concerns may appear in several discrete dreaming periods during a single night, dreams do not appear as successive chapters in a book, but rather as separate short stories. Dreams and waking mentation are similar in several respects. Most dreams collected over the course of a night are quite ordinary. Dreams have an undeserved reputation for being extremely bizarre because our spontaneous recall of dreams is usually limited to the longer, more exciting dreams that typically occur before morning awakening. In general a person's mood, anxiety, imaginativeness, and expressiveness in dreams are positively correlated with these traits in their waking experience. Except for some decrease in the clarity of background detail and color saturation, visual dream imagery resembles waking visual imagery. Like waking imagery, most dreams are in color; the mystery is why 20-30% of dreams are achromatic. Perhaps the greatest difference between dreaming and ordinary wakefulness is that we are able to differentiate between real and imagined images only when we are awake. Except for the relatively rare lucid dreams in which we know we are dreaming, all dream images seem real at the time. In spite of a lifetime of discriminating between dreams and reality, we can make the discrimination only after awakening. Identifying the neural substrates that are responsible for critical selfreflection during wakefulness, and that fail us while dreaming, is a major challenge for sleep and dream research. An Overall View The circadian rhythm of sleep is controlled by the suprachiasmatic nucleus of the hypothalamus. Non-REM sleep is generated by the interaction of neurons in the basal forebrain and medulla with neurons in the midbrain and diencephalon. REM sleep is generated by the interaction of neurons in the caudal midbrain and pons with neurons in the medulla and forebrain. Thus, sleep is actively generated by the interplay of several neuronal populations using different transmitters. Sleep serves important functions, as is indicated by its ubiquitous persistence in different environments and throughout evolution, by the rebound of sleep after sleep loss, and by the functional impairments (to the point of death) produced by sleep deprivation. No theory of sleep, however, has yet succeeded in explaining the exact function of sleep or providing a unified way of integrating the wealth of data now available on sleep. The discovery of a relationship between REM sleep and dreaming was a major impetus for modern sleep research. However, we now know that REM sleep is not necessary for dreaming, that dreaming can also occur during non-REM sleep, and that dreamlike experiences can be elicited during quiet wakefulness. REM sleep is also not sufficient for dreaming, since the integrity of certain cognitive skills is also necessary. Nevertheless, REM sleep is the state from which long vivid dreams are retrieved most reliably. As a result, studies of REM sleep have greatly increased knowledge about the number of dreams per night and their temporal characteristics, perceptual features, stimulus determinants, and cognitive features. The sources of specific dream content and an understanding of why we are usually unaware that we are dreaming while the dream is in progress still remain a mystery.
Figure 28.11. Summary of subcortical/cortical interactions that generate wakefulness and sleep. A variety of brainstem nuclei using several different neurotransmitters determine mental status on a continuum that ranges from deep sleep to a high level of alertness. These nuclei, which include the cholinergic nuclei of the pons-midbrain junction, the locus coeruleus, and the raphe nuclei, all have widespread ascending and descending connections (arrows) to other regions, which explain their numerous effects. Curved arrows along the perimeter of the cortex indicate the innervation of lateral cortical regions not shown in this plane of section. Summary All animals have a restorative cycle of rest following activity, but only mammals divide the period of rest into distinct phases of non-REM and REM sleep. Why mammals (and many other animals) need a restorative phase of suspended consciousness accompanied by decreased metabolism and lowered body temperature is not known. Even more mysterious is why the human brain is periodically active during sleep at levels not appreciably different from the waking state (that is, the neural activity during REM sleep). Despite the electroencephalographic similarities, the psychological states of wakefulness and REM sleepare obviously different. The highly organized sequence of human sleep states is actively generated by nuclei in the brainstem, most importantly the cholinergic nuclei of the pons-midbrain junction, the noradrenergic cells of the locus coeruleus, and the serotonergic neurons of the raphe nuclei. The activity of the relevant cell groups controls the degree of mental alertness on a continuum from deep sleep to waking attentiveness. These brainstem systems are in turn influenced by a circadian clocks located in the suprachiasmatic nucleus and VLPO of the hypothalamus. The clock adjusts periods of sleep and wakefulnessto appropriate durations during the 24-hour cycle of light and darkness that is fundamental to life on Earth. Several Endogenous Substances Affect Sleep For nearly a century sleep researchers have searched for substances that accumulate during waking and are metabolized in sleep. An understanding of how soluble substances might determine sleepiness would provide an important insight into sleep function, as well as the development of potent “natural” sleeping pills. However, no endogenous substance is yet widely accepted as causing sleep. Among the substances that have been identified as having hypnogenic properties are mura-myl peptides (a chemical related to substances found in bacterial cell walls), interleukin-1 (a cytokine that may mediate the effects of muramyl peptides as well as immune responses), adenosine, delta sleep-inducing peptide (a substance isolated from the blood of sleeping rabbits), prostaglandin D2, and a long-chain fatty acid primary amide, cis -9,10-octadecenoamide. Melatonin, a hormone synthesized in the brain, stimulates wakefulness when given to rats during the daytime and has a powerful hypnotic effect in birds. Human studies have not shown a consistent hypnotic effect, although recent studies have indicated that it can facilitate sleep onset in old people who are deficient in melatonin and may be of value in treating jet lag. It remains unclear whether it is effective as a treatment for insomnia, despite its popular promotion as a safe, natural sleeping pill. Sleep Periods Change Over the Life Span In humans daily sleep declines sharply from a peak of 17-18 hours at birth to 10-12 hours at age 4 and then more gradually to a fairly stable duration of 7-8.5 hours by age 20. The initial pattern of infancy, consisting of 3- to 4-hour bouts of sleep alternating with brief feedings, is gradually replaced by more continuous sleep. By age 4 sleep becomes consolidated into a single long nocturnal period and sometimes a daytime nap. In the newborn, REM phases constitute about 50% of sleep, but these REM phases differ from their adult form. The atonia is very irregular, and rapid eye movements and muscle twitches occur on a background of low muscle tone and a relatively undifferentiated EEG. The proportion of time spent in REM sleep declines rapidly until about 4 years of age, when it stabilizes near the level of young adults (20-25%). With increasing age, REM declines gradually to 15-20% (Figure 47-2). The high-amplitude, slow EEG waves of the non-REM phase are absent at birth. In humans these slow waves appear during the first year of life and their amplitudes greatly increase, reaching a stable, high plateau between 3-11 years of age. These developmental changes in sleep are accelerated in animals that mature rapidly. For example, in rats a mature sleep pattern is achieved 30 days after birth. In humans slow-wave activity begins to decline during adolescence and continues to decline for the rest of life. Like newborns, many people over age 50 show almost no high-amplitude EEG activity (Figure 47-2). Also, the nocturnal sleep of the elderly tends to be interrupted by many short awakenings. Neural Maturation and Mental Health The idea that REM sleep aids neural maturation is strongly supported by the association of REM sleep and immaturity at birth both across and within species. But why would REM sleep then persist and rebound after its selective deprivation in adults? Early anecdotal reports of disturbed behavior after REM sleep deprivation suggested that REM sleep is important for mental health, but none of several controlled studies has demonstrated that mental health is impaired as a result of REM deprivation. In fact, severely depressed patients improve after extended REM deprivation. Some reports indicate that REM sleep facilitates learning or memory, but the effects of REM sleep deprivation on learning and memory have not always been very strong or very consistent. In fact, learning can occur without sleep. The fact that REM sleep follows non-REM sleep suggests that REM sleep compensates for the cerebral inactivation or temperature declines of non-REM sleep. However, even when wakefulness (with its cerebral activation and increased temperature) follows selective REM sleep deprivation, compensatory increases of REM sleep follow later. In light of the many ideas about the function of sleep, sleep may have many functions. Alternatively, it may serve a single, as yet unidentified, cellular function important to a variety of processes: maturational processes in the young, temperature regulation in small animals, and cognitive processes in adult humans.