Hiv & pregnancy
•Download as PPTX, PDF•
26 likes•14,736 views

HIV stands for Human Immunodeficiency Virus and can be transmitted through sexual contact, blood transmission, or from mother to child. There are two types of HIV, HIV-1 being more prevalent. HIV progresses to AIDS by weakening the immune system over time. Prevention of mother-to-child transmission (PMTCT) aims to prevent HIV transmission from mother to child during pregnancy, birth, or breastfeeding through testing, treatment, and replacement feeding. Antiretroviral therapy can suppress HIV and slow disease progression.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (18)
Similar to Hiv & pregnancy
Similar to Hiv & pregnancy (20)
More from Mesfin Mulugeta
Recently uploaded
Recently uploaded (20)
Hiv & pregnancy
- 1. HIV AND PREVENTION OF MOTHER-TO-CHILD TRANSMISSION (PMTCT) By Gebremaryam T.
- 2. Cont… HIV stands for Human Immunodeficiency Virus. • Human: Infecting human beings • Immunodeficiency: Decrease or weakness in the body’s ability to fight off infections and illnesses • Virus: A pathogen having the ability to replicate only Inside a living cell
- 3. Types of HIV Virus There are two types of HIV virus: • HIV 1 is most common in sub-Saharan Africa and throughout the world. HIV 1 can be divided into groups M, N, and O. The pandemic is dominated by Group M, which is composed of subtypes A – J. • HIV 2 is most often found in West Central Africa, parts of Europe and India. Both produce the same patterns of illness. Both are RNA viruses with single strand of genetic materials. HIV 2 causes a slower progression of disease than HIV 1. It is important for tests to detect the HIV subtypes that are present in the region. • Otherwise, testing may lead to false negative results.
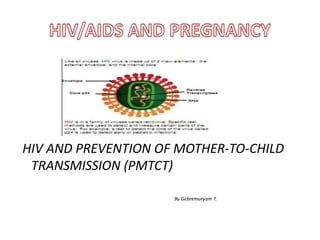
- 4. Structure of HIV cell
- 5. Cont… • Like all viruses, HIV virus is made up of 2 main elements: the external envelope, and the internal core. • Core p24 • RNA Reverse Transcriptase • Envelope • HIV is in a family of viruses called retrovirus
- 6. AIDS stands for: Acquired: To come into possession of something new Immune Deficiency: Decrease or weakness in the body’s ability to fight off infections and illnesses Syndrome: A group of signs and symptoms that occur together and characterize a particular abnormality AIDS is the final stage of the disease caused by infection with the virus.
- 7. Cont… • HIV is the virus that causes AIDS. Not everyone who is infected with HIV has AIDS. • AIDS is the result of progression of HIV Infection. Anyone infected with HIV, although healthy, can still transmit the virus to another person. • HIV infection leads to a weakened immune system. This makes a person with HIV vulnerable to infections.
- 8. Cont… • AIDS results when HIV infection progresses to an advanced stage, damaging the immune system to a point at which the body can no longer fight illness.. • Drugs treat HIV and AIDS are called antiretro virals (ARVs). • They prevent the virus from replicating and slow the progress of the disease.
- 9. 9 Modes of HIV Transmission • Sexual intercourse • Accidental exposure to blood/blood products (e.g., blood transfusions, shared needles, contaminated instruments) • Mother to child during: – pregnancy – birth – breastfeeding
- 10. 10 HIV Transmission Through Sexual Contact • Of every 100 HIV infected adults, 75-85 have been infected through unprotected intercourse – 70% of these infections are from heterosexual intercourse • STDs, especially ulcerative lesions in genitalia, increase risk of transmission Source: UNAIDS/WHO 1996.
- 11. HIV Transmission from Mother to Infant • Antenatal – In utero by transplacental passage • Intranatal – Exposure to maternal blood and vaginal secretions during labor and delivery • Postnatal – Postpartum through breastfeeding
- 12. 12 HIV Transmission HIV cannot be transmitted by: – Casual person to person contact at home or work or in social or public places – Food, air, water – Insect/mosquito bites – Coughing, sneezing, spitting – Shaking hands, touching, dry kissing – Swimming pools, toilets, etc.
- 13. 13 Women and HIV Social Risk Factors – Illiteracy – Lack of awareness of preventive measures Biological risk factors – Twice as easy for women to contract HIV from men – Physiology of women (e.g., menstruation, intercourse) – Pregnancy-associated conditions (e.g., anemia, menorrhagia and hemorrhage) increase the need for blood transfusion Economic Cultural Behavioral factors
- 14. 14 HIV and Contraception • Contraception with protection – Male condom (latex and vinyl) – Female condom – Nonoxynol-9 (antiviral spermicidal cream)1 – Diaphragm1 • Methods appropriate for use by women with HIV. They should use a condom for their partner’s protection. – Hormonals (COCs, Implants) – Voluntary sterilization 1Partial protection if used without condom
- 15. 15 Effect of AIDS on Pregnancy • Infertility • Repeated abortions • Prematurity • Intrauterine growth retardation • Stillbirths • Congenital abnormalities • Embryopathies
- 16. BENEFITS TO HIV TESTING • Early counseling and treatment of hiv infection • Ability to make decisions regarding pregnancy • Implementation of strategies to attempt to prevent transmission to fetus WHO SHOULD WE SCREEN • ALL: pregnant women • TARGETED TESTING FAILS TO IDENTIFY A SUBSTANTIAL PROPORTION OF HIV POSITIVE WOMEN
- 17. HIV infection can be measured in terms of: • The amount of virus circulating in the body – called the viral load • The amount of antigen – p24 antigen circulating in the body • Proteins or cells that protect the body against infection – IgG and IgM antibodies, and CD4 cells
- 18. Measuring human response to HIV infection: B and T cells • T and B cells are types of white blood cells called lymphocytes that provide protection against infection. • B cells are responsible for producing antibodies. • There are three types of T cells. Helper T-Cells (also called CD4+ cells) help other cells destroy infective organisms. Suppressor T-Cells (also called CD8+ cells) suppress the activity of other lymphocytes so they don’t destroy normal tissue.
- 19. Cont….. • Killer T-Cells (also called cytotoxic T lymphocytes, or CTLs, and are another kind of or CD8+ cell) recognize and destroy abnormal or infected cells. Over a period of time, HIV infects and kills white blood cells called CD4 lymphocytes or (T cells), leaving the body unable to fight off certain kinds of infections.
- 21. Window period • the phase when individual infected with HIV, but antibody levels are not detectable. • One may test false-negative for HIV antibodies, and can still pass the virus to others during this period. • What occurs during the window period is called seroconversion:
- 22. Cont… • Seroconversion” is a term used to describe the change from non-detectable to detectable antibody levels. • Specimen may test initially non-reactive, but change to testing reactive after a certain time period. • Seroconversion occurs generally 3-8 weeks after the initial infection
- 24. progression may be delayed by: • Prevention and early treatment of opportunistic infections (OIs) • Antiretroviral therapy • Positive living
- 25. The HIV Life Cycle 1 . Binding and Fusion HIV begins its life cycle when it binds to a CD4 receptor and one of two co-receptors on the surface of a CD4+ T-lymphocyte. The virus then fuses with the host cell. After fusion, the virus releases RNA, its genetic material, into the host cell
- 26. Life cycle cont… 2 . Reverse Transcription: An HIV enzyme called reverse transcriptase converts the singlestranded HIV RNA to double-stranded HIV DNA
- 27. Life cycle cont… 3 . Integration: The newly formed HIV DNA enters the host cell's nucleus, where an HIV enzyme called integrase "hides" the HIV DNA within the host cell's own DNA. The integrated HIV DNA is called provirus. The provirus may remain inactive for several years, producing few or no new copies of HIV
- 28. Life cycle cont… 4 . Transcription When the host cell receives a signal to become active, the provirus uses a host enzyme called RNA polymerase to create copies of the HIV genomic material, as well as shorter strands of RNA called messenger RNA (mRNA). The mRNA is used as a blueprint to make long chains of HIV proteins
- 29. Life cycle cont… 5 . Assembly An HIV enzyme called protease cuts the long chains of HIV proteins into smaller individual proteins. As the smaller HIV proteins come together with copies of HIV's RNA genetic material, a new virus particle is assembled
- 30. Life cycle cont… 6 . Budding: The newly assembled virus pushes out ("buds") from the host cell. During budding, the new virus steals part of the cell's outer envelope. This envelope, which acts as a covering, is studded with protein/sugar combinations called HIV glycoprotein. These HIV glycoprotein are necessary for the virus to bind CD4 and co receptors. The new copies of HIV can now move on to infect other cells
- 31. WHO Staging System for HIV in Adults and Adolescents Clinical stage I • Asymptomatic • Persistent generalized lymphadenopathy Performance scale 1: asymptomatic, normal activity
- 32. Clinical Stage 2 Recurrent bacterial RTI (two or more in any six-month period)Symptom complex, e.g. unilateral face pain with nasal discharge (sinusitis) or painful swollen eardrum (otitis media), cough with purulent sputum (bronchitis), sore throat (pharyngitis). Two or more documented occurrences of antibiotic responsive URTI. Herpes zoster Painful rash of small fluid filled blisters in distribution of a nerve supply, can be hemorrhagic on erythematous background, and does not cross midline. Current or in the last two years. Severe or frequently recurrent herpes zoster is usually associated with more advanced HIV disease.
- 33. Stage 2 cont… Angular cheilitis • Splits or cracks on lips at the angle of the mouth with depigmentation, usually responds to antifungal treatment but may recur. Also common in nutritional deficiency, e.g. of B vitamins. • Recurrent oral ulcerations occurring twice or more in six months Aphthous ulceration, typically with a halo of inflammation and a yellow-grey pseudomembrane.
- 34. Papular pruritic eruptions • Papular pruritic vesicular lesions. Also common in uninfected adults. Note: scabies and obvious insect bites should be excluded. Seborrhoeic dermatitis Itchy scaly skin condition, particularly affecting scalp, face, upper trunk and perineum. Also common in uninfected adults. Fungal nail infections of fingers Fungal paronychia (painful red and swollen nail bed) or onycholysis (separation of the nail from the nail bed) of the fingernails. Also common in uninfected adults. Proximal white subungual onchomycosis is uncommon without immunodeficiency.
- 35. Clinical Stage 3 • Unexplained chronic diarrhoea for longer than one month Chronic diarrhoea. • Unexplained persistent fever (intermittent or constant and for longer than one month)Reports of fever or night sweats for more than one month, either intermittent or constant with reported lack of response to antibiotics or antimalarials. No other obvious foci of disease reported or found on examination.
- 36. Cont…. • Oral candidiasis Persistent creamy white to yellow soft small plaques on red or normally colored mucosa which can often be scraped off (pseudo membranous), or red patches on tongue, palate or lining of mouth, usually painful or tender (erythematous form), not responding to local antifungal treatment.
- 37. Stage 3…. • Oral hairy leukoplakia Fine small linear patches on lateral borders of the tongue, generally bilaterally, which do not scrape off. • Acute necrotizing ulcerative • gingivitis or necrotizing ulcerative periodontitis Severe pain, ulcerated gingival papillae, loosening of teeth, spontaneous bleeding, bad odour, and rapid loss of bone and/or soft tissue. • Unexplained anaemia (<8g/dl), neutropenia (<1000/mm3) or thrombocytopenia (<50 000/ mm3) for more than one month
- 38. Stage four • Extrapulmonary/disseminated TB • Systemic illness usually with prolonged fever, night sweats, weakness and weight loss. • Clinical features of organs involved, e.g. focal lymphadenopathy, cold abscess, sterile pyuria, pericarditis, ascites, pleural effusion, meningitis, arthritis, CXR may reveal diffuse uniformly distributed small miliary shadows Response to standard anti-TB treatment in one month.
- 39. Stage four cont… • Kaposi’s sarcoma Typical appearance in skin or oropharynx of persistent, initially flat, patches with a pink or blood-bruise colour, skin lesions that usually develop into nodules. Can be confused clinically with bacillary angiomatosis, non-Hodgkin lymphoma and cutaneous fungal or bacterial infections. • CMV (retinitis or CMV infection of an organ other than liver, spleen or lymph nodes) • Retinitis only.
- 40. Stage four cont… • CNS toxoplasmosis Fever, headache, focal neurological signs, convulsions. • Rapid response (within 10 days) to high-dose co-trimoxazole, or pyrimethamine and sulphadiazine or clindamycin. • Cryptococcal meningitis or other extrapulmonary Cryptococcus infection Meningitis: usually subacute, fever with increasing severe headache, meningism, confusion, behavioural changes. • Responds to antifungal therapy.
- 41. Cont… • HIV encephalopathy Clinical finding of disabling cognitive and/or motor dysfunction interfering with activities of daily living, progressing over weeks or months in the absence of a concurrent illness or condition other than HIV infection which might explain the findings. Sever HSV © Slice of Life and Suzanne S. Stensaas
- 42. Clinical management Clinical events pre-ART Action • Stage 1 No action required • Stage 2 Requires cotrimoxazole • Stage 3 Or Stage 4 Requires cotrimoxazole if not already started Consider ART
- 43. Diagnosis • ELISA test with a sensitivity of >99.5 percent. • Western blot or immuno fluorescence assay (IFA), both of which have high specificity. • According to the Centers for Disease Control and Prevention, antibody can be detected in most patients within 1 month of infection, and thus, antibody serotesting may not exclude early infection. • For acute primary HIV infection, identification of viral p24 core antigen or viral RNA or DNA is possible. False-positive confirmatory results are rare
- 44. Dx cont… • “rapid” HIV test performed to women with limited prenatal care or with undocumented HIV status. These tests can detect HIV antibody in 60 minutes or less and have sensitivities and specificities comparable with those of conventional ELISAs. A negative rapid test result does not need to be confirmed. A positive rapid test result should be confirmed with a Western blot or IFA test.
- 45. Pharmacology
- 46. Classes of Antiretrovirals • NRTIs – Nucleoside reverse transcriptase inhibitors – Nucleotide reverse transcriptase inhibitors (NtRTI) • NNRTIs – non-nucleoside reverse transcriptase inhibitors • PIs – protease inhibitors • Fusion Inhibitors and entry inhibitors Enfuvirtide Maraviroc 46
- 47. ARVs and the HIV Lifecycle 47
- 48. Nucleoside Reverse Transcriptase Inhibitors (NRTIs) 48 RNA DNA Nucleus Host Cell
- 49. Types of NRTIs • Zidovudine (AZT) • Stavudine (d4T) • Lamivudine (3TC) • Didanosine (ddI) • Abacavir (ABC) • Zalcitabine (ddC) • Emtricitabine (FTC) • Tenofovir (TDF)-Nucleotide RTI 49
- 50. Non-Nucleoside Reverse Transcriptase Inhibitors (NNRTIs) 50
- 51. Non-Nucleoside Reverse Transcriptase Inhibitors • NNRTIs – Nevirapine (NVP) – Efavirenz (EFV) – dilavirdine 51
- 52. Protease Inhibitors (PIs) 52 DNA Host Cell
- 53. Protease Inhibitors (2) • Lopinavir + Ritonavir • Nelfinavir • Saquinavir-HGC • Indinavir • Fosamprenavir • Atazanavir • Ritonavir 53
- 54. Antiretroviral Drugs First Line Second Line AZT or d4T and 3TC and NVP or EFV ABC, TDF, or AZT and ddI and Lop/r, SQV/r, NFV, IND/r 54
- 55. 2003 vs. 2005 WHO Guidelines 55
- 56. PMTCT • PMTCT is a term used to describe a package of services comprehensive cares intended to reduce the risk of mother-to-child transmission of HIV in intrauterine, labor and delivery, post partum and breast feeding. • With out intervention the risk of MTCT is 20-45%
- 57. • approximately 600,000 HIV-infected infants are born every year–at least 1,600 every day–in resource-constrained countries. • Transmission occurs during pregnancy, labor and delivery, and breastfeeding. • The rate of mother to child transmission has been reduced to less than 5 percent among the limited number of HIV-infected women in developed countries.
- 58. • high rates are largely due to the lack of access to: –HIV voluntary counseling and testing – replacement feeding –selective caesarean section –antiretroviral drug therapy
- 59. 59 AIDS and Infants • Symptoms generally develop by 6 months of age – Diarrhea – Failure to thrive • Most of these children die before their second birthday • Children born to HIV-infected parents are likely to become orphans
- 60. Reducing pediatric HIV infection and disease involves three stages: • preventing HIV infection among women of childbearing age • preventing unwanted pregnancy among HIV-positive women • preventing mother to child transmission during pregnancy, labor and delivery, and breastfeeding
- 61. Risk factors for MTCT; contd… Obstetrical • Prolonged rupture of membrane (longer than 4 hours) • Mode of delivery • Intrapartum hemorrhage • Obstetrical procedures • Invasive fetal monitoring Fetal • Prematurity • Genetic • Multiple pregnancy Infant • Breastfeeding • Gastrointestinal tract factors • Immature immune system 61
- 62. PMTCT…. Estimated Risk of MTCT Timing Transmission Rate Without Any Interventions • During pregnancy 5-10% • During labor and delivery 10-15% • During breastfeeding 5-20% • Overall without breastfeeding 15-25% • Overall with breastfeeding to six months 20-35% • Overall with breastfeeding to 18-24 months 30-45% Note: Rates vary because of differences in population characteristics such as maternal CD4+ cell counts, RNA viral load and duration of breastfeeding.
- 63. PMTCT with Antiretroviral drugs All pregnant and breastfeeding women infected with HIV should initiate triple ART, which should be maintained for life long.
- 64. EVOLUTION OF WHO PMTCT ARV RECOMMENDATIONS 2001 2004 2006 2010 Launch July 2013 PMTCT 4 weeks AZT; AZT+ 3TC, or SD NVP AZT from 28 wks + SD NVP AZT from 28wks + sdNVP +AZT/3TC 7days Option A (AZT +infant NVP) Option B (triple ARVs) Option B or B+ Moving to ART for all PW/BF ART No recommendation CD4 <200 CD4 <200 CD4 <350 CD4 <500 Move towards: more effective ARV drugs, extending coverage throughout MTCT risk period, and ART for the mother’s health
- 65. When to Start ART
- 66. Rationale: Shift from Option A to B+ or B BENEFITS FOR MOTHER AND CHILD BENEFITS FOR PROGRAM DELIVERY & PUBLIC HEALTH Ensures all ART eligible women initiate treatment Reduction in number of steps along PMTCT cascade Prevents MTCT in future pregnancies Same regimen for all adults (including pregnant women) Potential health benefits of early ART for non-eligible women Simplification of services for all adults Reduces potential risks from treatment interruption Simplification of messaging Improves adherence with once daily, single pill regimen Protects against transmission in discordant couples Reduces sexual transmission of HIV Cost effective Major issue now is not “when to start” or “what to start” but “whether to stop”
- 67. Programmatic considerations for B+ • Initiate all HIV+ pregnant and breastfeeding women on ART • Operational and programmatic advantages to lifelong ART for pregnant and breastfeeding women (“B+”), particularly in settings with: – Generalized epidemics – High fertility (though need to strengthen FP) – Long duration of breastfeeding – Limited access to CD4 to determine ART eligibility – High partner serodiscordance rates
- 68. ARVs and breastfeeding 2013 (no change from 2010) National agencies should decide between promoting mothers with HIV to either breastfeed and receive ARV interventions or to avoid all breastfeeding Where the national choice is to promote BF, mothers whose infants are HIV uninfected or of unknown HIV status should: • exclusively breastfeed their infants for the first six months of life • introduce appropriate complementary foods thereafter, and continue breastfeeding for the first 12 months of life • breastfeeding should then only stop once a nutritionally adequate and safe diet without breast-milk can be provided (strong recommendation, high-quality evidence for the first 6 months; low-quality evidence for the recommendation of 12 months)
- 69. Summary of Changes in Recommendations: What to Start in Adults FIRST-LINE REGIMENS (PREFERRED ARV REGIMENS) TARGET POPULATION 2010 ART GUIDELINES 2013 ART GUIDELINES STRENGTH & QUALITY OF EVIDENCE HIV+ ARV-NAIVE ADULTS AZT or TDF + 3TC (or FTC) + EFV or NVP TDF + 3TC (or FTC) + EFV (as fixed-dose combination) Strong, moderate-quality evidence HIV+ ARV-NAIVE PREGNANT WOMEN AZT + 3TC + NVP or EFV HIV/TB CO-INFECTION AZT or TDF + 3TC (or FTC) + EFV HIV/HBV CO-INFECTION TDF + 3TC (or FTC) + EFV
- 70. QUESTION ??? • What points are important when counseling a pregnant women with HIV? 72
- 71. Ante natal care • ANC allows interaction between the health facility and sexually active women to: – provide information on HIV – promote safer sex practices, – provide opportunity for the pregnant woman to know her HIV status – Identify and treat STIs – Advice on use of ITN • Provides opportunities to discuss the interventions for reducing the risk of MTCT 73
- 72. Counseling HIV positive pregnant women??? • Effect of pregnancy on HIV infection • Effect of HIV on pregnancy outcome • Risk of transmission to fetus and infant • Treatment options in pregnancy • Interventions to prevent mother to infant transmission • Infant feeding options • Disclosure of results to partner • Need for follow up of mother and child • Future fertility and contraceptive options 74
- 73. Question • What measures can you take during antenatal care (ANC) of an HIV-positive woman to reduce the risk of transmission of HIV? 75
- 74. Antenatal interventions to reduce MTCT • HIV testing and counseling services • Behavior change communication: – Sexual – Injection drug use – Alcohol use and smoking • Prevention of new infections in pregnancy • Identification and treatment of STIs (genital ulcers and abnormal vaginal discharge) • Use ITN for malaria prevention 76
- 75. Antenatal interventions to reduce MTCT contd • Prevention and treatment of anemia (balanced diet and nutritional supplementation) • Avoiding invasive testing procedures in pregnancy – Amniocentesis – Chorionic villus sampling – External cephalic version • Multivitamin supplementation • Tetanus toxoid immunization 77
- 76. Antenatal interventions to reduce MTCT contd • Antiretroviral Treatment – Initiate HAART to all HIV positive pregnant women identified according to the national guideline (option B+): • During pregnancy • In labour • Postpartum (ART’s should be provided to the mother for her health as well as for the health of the baby.) • Physical examination to detect any signs of HIV-related illness 78
- 77. Antenatal interventions to reduce MTCT cont’d • Use ITN for malaria prevention • Mebendazole at first visit in areas of high worm prevalence • Isoniazid (INH) prophylaxis for tuberculosis (TB) if indicated • Pneumocystis carinii pneumonia (PCP) prophylaxis, in women with clinical signs of AIDS or CD4 counts of below 200 mm3 • Psychological support 79
- 78. QUESTION ??? • What measures can you take during labor and delivery to reduce the risk of transmission of HIV? 80
- 79. Intrapartum interventions to reduce MTCT • Application of good infection prevention practices during pelvic examinations and delivery • Avoiding unnecessary artificial rupture of membranes • Avoiding prolonged labour and prolonged rupture of membranes 81
- 80. Intrapartum interventions to reduce MTCT contd • Avoid unnecessary trauma during delivery: –Unnecessary episiotomy –Forceps delivery –Vacuum extraction 82
- 81. Vaginal versus Caesarean Risk concern Vaginal Caesarean Blood loss - Increased Infection - Increased in HIV+ women; antibiotic prophylaxis recommended MTCT No evidence of increased MTCT with ARV Rx and adequate viral load Reduces risk of MTCT if performed before labor onset Mortality - Increased Resource issues - Requires greater resources (supplies, equipment, staff) 83
- 82. Intrapartum interventions to reduce MTCT (cont.) • Minimize risk of PPH (to protect mother’s health and decrease provider exposure to blood) – Active management of 3rd stage • Administer oxytocin immediately after delivery • Controlled cord traction • Check for contraction of the uterus – Repair any genital tract lacerations – Make sure placenta is complete 84
- 83. HARRT regimen to HIV +pregnant women • Initiate HAART to all HIV women identified during pregnancy, labour and postpartum period as follows – TDF, 3TC, and EFV ( single tab combination one tablet daily) ARV for New born : Daily Neverapiine for six weeks 85
- 84. Feeding options for the HIV exposed infant “A little bit of this and a little bit of that is not best for the baby! ” Avoid mixed feeding ! 86 Exclusive breast Feeding Exclusive formula Feeding
- 85. Breastfeeding • Exclusive breastfeeding should be encouraged among all women regardless of HIV status • For HIV free survival, all women for whom replacement feeding is not acceptable, feasible, affordable, sustainable and safe (AFASS) should be encouraged to exclusively breastfeed their infant for six months • A woman should be supported in her infant feeding decision; the choice is hers 87
- 86. Ongoing care • HARRT is initiated for HIV positive mothers in ANC will continue during post partum period until graduated from PMTCT services • All HIV infected mothers should be linked to care and support to help keep them in the best health possible 88
- 87. Fig. 6.1: PMTCT as an Entry Point for Care and Support Palliative care Income support PMTCT Planning for the future (including FP) Psychosocial support Basic clinical care (mother, infant) Prevention and Rx of OIs Access to ARVs Nutritional Support 89
- 88. Newborn • Irrespective of the HIV status handle with gloves until maternal blood and secretions have been washed off • Avoid hypothermia • Give antiretroviral agents according to the recommendation ( Neverapiine for six weeks), if available • Watch for anaemia • Follow up infant for infection 90
- 89. Immediate care of the neonate • Cut cord under cover of a lightly wrapped gauze swab, to prevent blood spurting. • Handle all babies regardless of the mother’s HIV status with gloves until maternal blood and secretions are washed off. • All babies irrespective of HIV status should be kept warm post-delivery. 91
- 90. Immediate care of the neonate (cont) • Do not suction the newborn with a nasogastric (NG) tube unless there has been meconium-stained liquid. • Where suctioning is required: – use a mechanical suction unit (at a pressure below 100mm Hg) or bulb suction, if possible, rather than the mouth operated suction. Do not use the bulb syringe for another baby before high level disinfection done . • Attach the baby to the mother’s breast only if the mother has made a prior decision to breastfeed. 92
- 91. Immediate care of the neonate (cont) • If the mother has decided not to breastfeed, place the baby on the mother’s body for skin-to-skin contact. Provision should be made to provide the mother with infant formula • Vitamin K should be administered as per national guidelines • BCG should be administered according to the national/WHO immunization guideline. • Antibiotic or 1% silver nitrate eye ointment should be administered as prophylaxis against ophthalmia neonatorum according to the national/WHO immunization guideline. 93
- 92. QUESTION ??? • What breastfeeding issues must be considered when helping an HIV-positive mother to decide whether or not to breastfeed? 94
- 93. Breastfeeding Issues • Warmth for newborn • Nutrition for newborn • Protection against other infections • Risk of HIV transmission • Contraception for mother • AFASS - the mother who is infected with HIV should breastfeed unless replacement feeding is acceptable, feasible, affordable, safe, and sustainable (AFASS). 95
- 94. Breastfeeding Recommendations • If the woman is: – HIV-positive and chooses to breastfeed, promote exclusive breastfeeding for 6 months – HIV-negative or does not know her HIV status, promote exclusive breastfeeding for 6 months – HIV-positive, meets AFASS criteria, and chooses to use replacement feedings, counsel on the safe and appropriate use of formula – HIV-positive and chooses to breastfeed, promote exclusive breastfeeding for 6 months 96
- 95. Goals of FP for HIV infected women • Prevention of unintended pregnancy • Appropriate child spacing to reduce maternal and infant morbidity and mortality 97
- 96. Special considerations for choosing FP method • Effectiveness • Safety/side effects • Effect on HIV transmission or progression • Effect on STI transmission or acquisition • Ease of use • Non-contraceptive benefits • Potential interactions with other medications 98
- 97. CONDOMS and HIV 99 Pregnancy! STDs! HIV re-infection! Male or female condoms combine protection from...
- 98. Key take-away points • Women with HIV infection require focused antenatal care provided in accordance with national protocols. • HIV can be transmitted from an infected mother to her child during pregnancy, labour and delivery, or through breastfeeding. • Antiretroviral therapy regimens reduce the risk of MTCT and improve maternal survival in both breastfeeding and non-breastfeeding women. 100
- 99. Key take-away points (cont.) • Women should be monitored for signs or symptoms of progressive HIV/AIDS, and opportunistic infections, particularly tuberculosis (TB). • Exclusive breastfeeding should be recommended to reduce the risk of MTCT during the postnatal period unless the mother chose to give Replacement feeding . • Decisions about infant feeding options should be made before delivery. 101
- 100. HIV FREE SERVIVAL WITH THE HELP OF COMPITENT MIDWIFES