Presentació "Real-Life VR Integration for Mild Cognitive Impairment Rehabilit...
Cns Presentatio
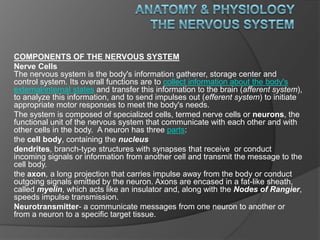
1. Anatomy & Physiology The Nervous System COMPONENTS OF THE NERVOUS SYSTEM Nerve CellsThe nervous system is the body's information gatherer, storage center and control system. Its overall functions are to collect information about the body's external/internal states and transfer this information to the brain (afferent system), to analyze this information, and to send impulses out (efferent system) to initiate appropriate motor responses to meet the body's needs. The system is composed of specialized cells, termed nerve cells or neurons, the functional unit of the nervous system that communicate with each other and with other cells in the body. A neuron has three parts: the cell body, containing the nucleus dendrites, branch-type structures with synapses that receive or conduct incoming signals or information from another cell and transmit the message to the cell body. the axon, a long projection that carries impulse away from the body or conduct outgoing signals emitted by the neuron. Axons are encased in a fat-like sheath, called myelin, which acts like an insulator and, along with the Nodes of Rangier, speeds impulse transmission. Neurotransmitter- a communicate messages from one neuron to another or from a neuron to a specific target tissue.
2. Major Divisions of the Nervous System The nerves of the body are organized into two major systems: the central nervous system (CNS), consisting of of the brain and spinal cord, the peripheral nervous system (PNS), the vast network of spinal and cranial nerves linking the body to the brain and spinal cord. The PNS is subdivided into: the autonomic nervous system (involuntary control of internal organs, blood vessels, smooth and cardiac muscles), consisting of the sympathetic NS and parasympathetic NS the somatic nervous system (voluntary control of skin, bones, joints, and skeletal muscle). Brain Structures The brain, the body's "control central," is one of the largest of adult organs, consisting of over 100 billion neurons and weighing about 3 pounds. It is typically divided into four parts: the cerebrum; the cerebellum; the diencephalons (thalamus, hypothalamus, sometimes classed as cerebral structures); and the brain stem(medulla oblongata, pons, midbrain), which is an extension of the s spin spinal cord. Parts of the Brain CerebrumThe largest division of the brain, the cerebrum, consists of two sides, the right and left cerebral hemispheres, which are interconnected by the corpus callosum. The two hemispheres are "twins," each with centers for receiving sensory (afferent) information and for initiating motor (efferent) responses. The left side sends and receives information to/from the right side of the body, and vice versa. Various intellectual functions are concentrated in either the left or right hemispheres. CerebellumThe cerebellum, the second largest brain structure, sits below the cerebrum. Like the cerebrum, the cerebellum has an outer cortex of gray matter and two hemispheres. It receives/relays information via the brain stem. The cerebellum performs 3 major functions, all of which have to do with skeletal-muscle control:
3. Diencephalons The diencephalons, located between the cerebrum and the midbrain, consists of several important structures, two of which are the: Thalamus: large, bilateral (right thalamus/left thalamus) egg-shaped mass of gray matter serving as the main synaptic relay center. Receives/relays sensory information to/from the cerebral cortex, including pain/pleasure centers. Hypothalamus: a collection of ganglia located below the thalamus and intimately associated with the pituitary gland. It has a variety of functions: senses changes in body temperature; controls autonomic activates and hence regulates the sympathetic and parasympathetic nervous systems; The four lobes perform specific functions: frontal – largest lobe, located in the front of the skull, functions are for concentration, abstract thinking, information storage or memory, and motor function. It also contains Boca's area, critical for motor control of speech. Responsible also in large part for a person’s affect, judgment, personality, and inhibitions. parietal - a predominantly sensory lobe located near crown of the head. Coordinates afferent information dealing with pain, temperature, form, shape, texture, pressure, and position. temporal - located around the temples that handles dreams, memory, and emotions. Center for auditory function. occipital - posterior lobe of the cerebral hemisphere located at the lower back of the head governs vision interpretation.
11. ASSESSMENT: THE NEUROLOGIC EXAMINATION The following is a widely accepted format for the neurologic exam, consisting of six subdivisions: 1. Mental Status2. Cranial Nerves3. Motor Exam 4. Reflexes5. Coordination and Gait6. Sensory Exam Equipment Needed Reflex Hammer 128 and 512 (or 1024) Hz Tuning Forks A Snellen Eye Chart or Pocket Vision Card Pen Light or Otoscope Wooden Handled Cotton Swabs Paper Clips General Considerations Always consider left to right symmetry Consider central vs. peripheral deficits
12. MENTAL STATUS A mental status examination (MSE) is an assessment of a patient's level of cognitive (knowledge-related) ability, appearance, emotional mood, and speech and thought patterns at the time of evaluation. It is one part of a full neurologic (nervous system) examination and includes the examiner's observations about the patient's attitude and cooperativeness as well as the patient's answers to specific questions. The purpose of a mental status examination is to assess the presence and extent of a person's mental impairment. A complete MSE is more comprehensive and evaluates the following ten areas of functioning: Appearance. The examiner notes the person's age, race, sex, civil status, and overall appearance. These features are significant because poor personal hygiene or grooming may reflect a loss of interest in self-care or physical inability to bathe or dress oneself. Movement and behavior. The examiner observes the person's gait (manner of walking), posture, coordination, eye contact, facial expressions, and similar behaviors. Problems with walking or coordination may reflect a disorder of the central nervous system. Affect. Affect refers to a person's outwardly observable emotional reactions. It may include either a lack of emotional response to an event or an overreaction. Mood. Mood refers to the underlying emotional "atmosphere" or tone of the person's answers. Speech. The examiner evaluates the volume of the person's voice, the rate or speed of speech, the length of answers to questions, the appropriateness and clarity of the answers, and similar characteristics. Thought content. The examiner assesses what the patient is saying for indications of hallucinations, delusions, obsessions, symptoms of dissociation, or thoughts of suicide. Dissociation refers to the splitting-off of certain memories or mental processes from conscious awareness. Thought process. Thought process refers to the logical connections between thoughts and their relevance to the main thread of conversation. Irrelevant detail, repeated words and phrases, interrupted thinking (thought blocking), and loose, illogical connections between thoughts, may be signs of a thought disorder. Cognition. Cognition refers to the act or condition of knowing. The evaluation assesses the person's orientation with regard to time, place, and personal identity; long- and short-term memory; ability to perform simple arithmetic; general intellectual level or fund of knowledge; ability to think abstractly; ability to name specified objects and read or write complete sentences; ability to understand and perform a task; ability to distinguish between right and left. Judgment. The examiner asks the person what he or she would do about a commonsense problem, such as running out of a prescription medication. Insight. Insight refers to a person's ability to recognize a problem and understand its nature and severity.
13. CRANIAL NERVES I - Olfactor To discern smells. The patient is asked to identify the odor. II - Optic Examine the Optic Fundi Test Visual Acuit Screen Visual Fields by Confrontation Test Pupillary Reactions to Light III - Oculomotor Observe for Ptosis Test Pupillary Reactions to Light IV - Trochlear Test Extraocular Movements (Inward and Down Movement) V - Trigeminal Test Temporal and Masseter Muscle Strength Test the Three Divisions for Pain Sensation If you find and abnormality then: Test the Corneal Reflex VI - Abducens Test Extraocular Movements (Lateral Movement) VII - Facial Observe for Any Facial Droop or Asymmetry Ask Patient to do the following, note any lag, weakness, or assymetry Test the Corneal Reflex VIII - Acoustic Screen Hearing Test for Lateralization (Weber test) Compare Air and Bone Conduction (Rinne test) Vestibular Function is Not Normally Tested
14. IX - GlossopharyngealSee Vagus NerveX - VagusListen to the patient's voice, is it hoarse or nasal?Ask Patient to Swallow Ask Patient to Say "Ah"Test Gag Reflex (Unconscious/Uncooperative Patient)XI - AccessoryFrom behind, look for atrophy or assymetry of the trapezius muscles. Ask patient to shrug shoulders against resistance. Ask patient to turn their head against resistance. Watch and palpate the sternomastoid muscle on the opposite side. XII - HypoglossalListen to the articulation of the patient's words. Observe the tongue as it lies in the mouth Ask patient to: Motor Observation Involuntary Movements Muscle Symmetry Left to Right Proximal vs. Distal Atrophy Pay particular attention to the hands, shoulders, and thighs. Gait Muscle Tone Ask the patient to relax. Flex and extend the patient's fingers, wrist, and elbow. Flex and extend patient's ankle and knee. There is normally a small, continuous resistance to passive movement. Observe for decreased (flaccid) or increased (rigid/spastic) tone.
15. Muscle Strength Test strength by having the patient move against your resistance. Always compare one side to the other. Grade strength on a scale from 0 to 5 "out of five": Grading Motor StrengtH Grade Description 0/5 - No muscle movement 1/5 - Visible muscle movement, but no movement at the joint 2/5 - Movement at the joint, but not against gravity 3/5 - Movement against gravity, but not against added resistance 4/5 - Movement against resistance, but less than normal 5/5 - Normal strength Test the following: Flexion at the elbow (C5, C6, biceps) [p513] Extension at the elbow (C6, C7, C8, triceps) Extension at the wrist (C6, C7, C8, radial nerve) Squeeze two of your fingers as hard as possible ("grip," C7, C8, T1) Finger abduction (C8, T1, ulnar nerve) Oppostion of the thumb (C8, T1, median nerve) Flexion at the hip (L2, L3, L4, iliopsoas) Adduction at the hips (L2, L3, L4, adductors) Abduction at the hips (L4, L5, S1, gluteus medius and minimus) Extension at the hips (S1, gluteus maximus) Extension at the knee (L2, L3, L4, quadriceps) Flexion at the knee (L4, L5, S1, S2, hamstrings) Dorsiflexion at the ankle (L4, L5) Plantar flexion (S1)
16. REFLEXES Deep Tendon Reflexes The patient must be relaxed and positioned properly before starting. Reflex response depends on the force of your stimulus. Use no more force than you need to provoke a definite response. Reflexes should be graded on a 0 to 4 "plus" scale: Tendon Reflex Grading Scale Grade Description 0 Absent 1+ or + Hypoactive 2+ or ++ "Normal“ 3+ or +++ Hyperactive without clonus 4+ or ++++ Hyperactive with clonus Biceps (C5, C6) The patient's arm should be partially flexed at the elbow with the palm down. Place your thumb or finger firmly on the biceps tendon. Strike your finger with the reflex hammer. You should feel the response even if you can't see it. Triceps (C6, C7) Support the upper arm and let the patient's forearm hang free. Strike the triceps tendon above the elbow with the broad side of the hammer. If the patient is sitting or lying down, flex the patient's arm at the elbow and hold it close to the chest. Brachioradialis (C5, C6) Have the patient rest the forearm on the abdomen or lap. Strike the radius about 1-2 inches above the wrist. Watch for flexion and supination of the forearm.
17.
18. Note the contraction of the abdominal muscles and deviation of the umbilicus towards the stimulus. Knee (L2, L3, L4) Have the patient sit or lie down with the knee flexed. Strike the patellar tendon just below the patella. Note contraction of the quadraceps and extension of the knee. Ankle (S1, S2) Dorsiflex the foot at the ankle. Strike the Achilles tendon. Watch and feel for plantar. Point-to-Point Movements Ask the patient to touch your index finger and their nose alternately several times. Move your finger about as the patient performs this task. Hold your finger still so that the patient can touch it with one arm and finger outstretched. Ask the patient to move their arm and return to your finger with their eyes closed. Romberg Be prepared to catch the patient if they are unstable. Ask the patient to stand with the feet together and eyes closed for 5-10 seconds without support. The test is said to be positive if the patient becomes unstable (indicating a vestibular or proprioceptive problem). Gait Ask the patient to: Walk across the room, turn and come back Walk heel-to-toe in a straight line Walk on their toes in a straight line Walk on their heels in a straight line Hop in place on each foot
19. DIAGNOGTIC EVALUATION. Neurological tests to evaluate patients may include: computerized tomography (CT ) or computer assisted tomography (CAT) scans -- forms of radiology or imaging that use computers to construct two-dimensional pictures of selected parts of the body. Dye may be injected into a vein to obtain a better picture. electroencephalogram (EEG) -- a procedure that records the brain's continuous electrical activity by means of electrodes attached to the scalp. magnetic resonance imaging (MRI) -- an advanced method of imaging the brain using a very strong magnet, without radiation. electromyogram (EMG) -- a procedure that measures and records electrical activity from the muscles and nerves with mild electrical shocks to stimulate the nerves. arteriogram (angiogram) -- a procedure that provides a scan of arteries going to and through the brain. cerebral spinal fluid analysis (spinal tap) -- a procedure used to make an evaluation or diagnosis by examining the fluid withdrawn from the spinal column. evoked potentials -- procedures that record the brain's electrical response to visual, auditory, and sensory stimuli. myelogram -- a procedure that uses dye injected into the spinal canal to make the structure clearly visible on x-rays. neurosonography -- a procedure that uses ultra high frequency sound waves that enable the physician to analyze blood flow in cases of possible stroke. other procedures