Important disorders of colon
•Télécharger en tant que PPSX, PDF•
20 j'aime•9,024 vues

This is a powerpoint slideshow discussing some of the commonest disorders of colon; namely Hirschsprung's disease, Diverticular diseases of colon, ulcerative colitis, pseudomembranous colitis and ischemic colitis.

Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
En vedette (20)
Similaire à Important disorders of colon
Similaire à Important disorders of colon (20)
Plus de Department of Health & Family Welfare, Government of West Bengal
Plus de Department of Health & Family Welfare, Government of West Bengal (20)
Dernier
Dernier (20)
Important disorders of colon
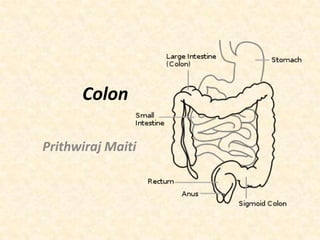
- 3. • Last part of the digestive system in most vertebrates. • Length = 135 cm. • Colon consists of four sections: – Ascending colon, – Transverse colon, – Descending colon, – Sigmoid colon. • Proximal colon= (Ascending colon + Transverse colon). • The cecum, colon, rectum and anal canal - the large intestine.
- 4. • Wall– Mucosa – Submucosa – Inner circular muscle layer – Outer longitudinal muscle layer
- 5. Identification of colon 3 taenia coli. Appendices epiploicae: Small pocket of fat filled peritoneum- except appendix, caecum and rectum. Haustra: Sacculations between taeniae.
- 7. Endoscopic appearance of the caecum. The characteristic trefoil appearance of the confluence of the three taeniae is usually obvious. Endoscopic appearance of the transverse colon. The characteristic triangular appearance of the haustrations when viewed collectively is obvious.
- 8. Blood supply Typical pericolic arrangement of arterial vasculature.
- 10. • Superior Mesenteric Artery (Caecum to splenic flexure)1. Right colic, 2. Middle colic. 3. Ileocolic. • Inferior Mesenteric Artery (Descending and sigmoid colon)1. Left colic, 2. Sigmoid, 3. Superior rectal. • Arc of Riolan: Anastotic arcade of SMA & IMA. • Venous drainage: SMV- Portal vein, IMV-Spenic vein.
- 11. Lymphatic drainage • Epicolic- Located in colonic wall. • Paracolic- Located along the inner margin. • Intermediate- Located near mesenteric vessel. • Principal- Located near main mesenteric vessel.
- 12. Nerve supply • Under autonomic nervous system. • Parasympathetic- Vagi and pelvic nerves. • Sympathetic- Superior and inferior mesenteric ganglia.
- 13. HIRSCSPRUNG’S DISEASE/ CONGENITAL MEGA COLON • Congenital, familial (10%). • Absence of ganglion cells- Auerbach’s plexus and Meissner’s plexus of colon. • Always involve anus, internal sphincter & rectum (partly/entirely). • Gene mutation in chromosome 10 occasionally 13.
- 14. HIRSCSPRUNG’S DISEASE/ CONGENITAL MEGA COLON Zones: 1. Distal immobile spastic segment .i.e. aganglionic zone. 2. Proximal middle transitional zone. 3. More proximal hypertrophied dilated segment- Normal.
- 15. HIRSCSPRUNG’S DISEASE/ CONGENITAL MEGA COLON Types: 1. Ultra short segment HD, 2. Short segment HD, 3. Long segment HD, 4. Total colonic HD.
- 16. HIRSCSPRUNG’S DISEASE/ CONGENITAL MEGA COLON Clinical features • • • • PresentationAcute, recurrent and chronic. Male- 80% Infant and children also adult (Down’s syndrome most common association). • 90% within 3 days of birth- fails to pass stool- After introduction of finger tooth paste like stool- feature of intestinal obstruction. • Children- Goat pellet like stool, malnutrition, abdominal distension– chronic type constipation-pass stool once in 3-4 days – • PR- TIGHT SPHINCTER + EMPTY RECTUM- PASS LOT OF GAS AND MECONIUM.
- 17. HD Complication– Colitis, – Intestinal obstruction, – Growth retardation, – Constipation, – Perforation, – Peritonitis, – Septicaemia.
- 18. HIRSCSPRUNG’S DISEASE/ CONGENITAL MEGA COLON • M/t • Diagnosis– History – X ray abdomen – Biopsy from all 3 zones- Starting from 2 cm above dentate line- Full thickness rectal biopsy. – Barium enema- Extent. – Anorectal manometry- Absence of rectoanal reflex. – Acetylcholenesterase staining- Hypertrophied nerve bundle.
- 19. • D/d – Total neuronal dysplasia, – Acquired megacolon, – ARM, – Hypothyroidism, – Meconium plug syndrome.
- 20. T/t -surgery – Colostomy-nutritional supplement-definitive procedure – Excision of aganglionic segment – Maintenance of continuity – Closure of colostomy Duhamel’s operation Soave’s
- 21. DIVERTICULAR DISEASE OF COLON • Acquired herniations of colonic mucosa through circular muscles at the points where blood vessels penetrate. • Raised intraluminal pressure results in pulsion diverticula. • Most common- Sigmoid. • Rectum not affected. • Etiology– Low fibre diet, – Female, – Non-veg, – NSAID, STEROID, immunocompromised; – Smoking, alcohol; – Long standing constipation.
- 22. DIVERTICULAR DISEASE OF COLON Types • Diverticulosis- Primary initial asymptomatic or painful stage (muscular incoordination, increased intraluminal pressure). • Diverticulitis: Second stage with inflammation of diverticula with pericolitis→ Persistent pain in LIF, fever, loose stool recurrent constipation, tender LIF, palpable thickened colon, P/R= tender mass.
- 23. DIVERTICULAR DISEASE OF COLON
- 24. Hinchey’s classification of diverticulitis
- 25. DIVERTICULAR DISEASE OF COLON • Investigation– Barium enema- Saw teeth appearance, Champagne glass sign – Sigmoidoscopy- Not in acute stage – Colonoscopy – CT scan • D/D – CA colon, amebic colitis, ulcerative colitis, ischaemic colitis, crohn’s disease, TB.
- 26. Diverticulitis Barium Enema (showing spasm)
- 27. Treatment • Medical – – – – High fiber diet. Antibiotic. Bulk purgative- Avoid constipation. Acute- Bowel rest, antispasmodic, antibiotic. • Abscess-guided aspiration • Surgery – Resection anastomosis of sigmoid/ colostomyanastomosis. – Reilly’s myotomy.
- 28. ULCERATIVE COLITIS • Ulcerative colitis (Colitis ulcerosa, UC) is a form of inflammatory bowel disease (IBD). • Etiological factor: – Western diet, red meat – Defective mucin production in colonic mucosa and mucosal immunological reaction – Autoimmune factors – Appendicectomy and smoking protects – Familial – Allergy to milk – Psychological aspects- stress, life style, personality disorders.
- 29. • Pathology– Multiple minute ulcer with proctitis and colitis→ – – – – – – Ulcer extend to deeper layer→ Spasm→ Stricture→ Pipe stem colon→ In between ulcer inflamed epithelium→ Pseudopolyp.
- 30. • Ulcerative colitis is normally continuous from the rectum up the colon. • Classification by the extent of involvement. • Distal colitis, potentially treatable with enemas: – – – – Proctitis: limited to the rectum. Proctosigmoiditis: rectosigmoid colon, Left-sided colitis: descending colon, Extensive colitis: inflammation extending beyond the reach of enemas: – Pancolitis: Involvement of the entire colon, extending from the rectum to the cecum, beyond which the small intestine begins.
- 31. ULCERATIVE COLITIS • Clinical features: – Abdominal pain – Diarrhea- watery, mucous or blood stained – Loss of appetite – Weight loss – Weakness or fatigue • Fulminant • Chronic
- 32. Clinical grading • Mild disease – – – – – <4 stools daily, with or without blood. No systemic signs of toxicity. Normal ESR/ CRP. Mild abdominal pain or cramping. Tenesmus. Rectal pain is uncommon. • Moderate disease – – – – – – >4 stools daily. Minimal signs of toxicity. Anemia (not requiring transfusions), weight loss. Moderate abdominal pain, Low grade fever, 38 to 39 °C (100 to 102°F). ESR↑.
- 33. • Severe disease – – – – > 6 bloody stools/ day. Massive and significant bloody bowel movement. Evidence of toxicity - fever, tachycardia, anemia. Elevated ESR or CRP. • Fulminant disease – – – – – – – >10 bowel movements/day. Continuous bleeding. Toxicity. Abdominal tenderness and distension. Blood transfusion requirement . Colonic dilation (expansion). Inflammation may extend beyond just the mucosal layer→ impaired colonic motility→ toxic megacolon. – Serous membrane may involved → colonic perforation. – Unless treated, fulminant disease will soon lead to death.
- 34. Extraintestinal features Frequency: 6 - 47%. • Aphthous ulcer of the mouth. • Ophthalmic (involving the eyes): – Iritis or uveitis, episcleritis. • Musculoskeletal: – Seronegative arthritis, – Ankylosing spondylitis, – Sacroiliitis.
- 35. • • • • • Extraintestinal features Cutaneous (related to the skin): – Erythema nodosum- panniculitis inflammation of subcutaneous tissue involving the lower extremities. – Pyoderma gangrenosum, which is a painful ulcerating lesion involving the skin. Deep venous thrombosis and pulmonary embolism. Autoimmune hemolytic anemia. Clubbing. Primary sclerosing cholangitis.
- 36. Complication • Pseudopolyposis, stricture, fistula, perforation, m alignancy, toxic megacolon, haemorrhage, severe malnutrition, cirrhosis. • Toxic megacolon (megacolon toxicum): – – – – Acute form of colonic distension. Very dilated colon-megacolon> 6 cm. Abdominal distension, fever, abdominal pain or shock. Toxic megacolon is usually a complication of UC and rarely of crohn's disease and some infections ex.: Clostridium difficile, Entamoeba histolytica and Shigella. – Wall thinned out-immediate intervention.
- 37. ULCERATIVE COLITIS • Factors involved for Carcinoma in UC – Extent of involvement –more in total colonic – Duration of disease- 5%-15yr, 25%-25yr, 35%30yr, 65%-40yr. – Site of involvement- Left more. – Sex - Equal in both sex. – Carcinoma in UC are aggressive, poorly differentiated, multicentric, synchronous , infiltrative and schirrous.
- 38. ULCERATIVE COLITIS • • • • Investigation Barium enema Blood and stool tests Visual examination – Sigmoidoscopy – Colonoscopy
- 39. • • • • • • • • • • CBC-Hb↓; Platelet↑ Electrolyte- Hypokalemia, Hypomagnesemia. Renal function tests- Pre-renal failure. Liver function tests- Primary sclerosing cholangitis. ESR↑ CRP↑ X-ray, Barium enema, Urinalysis. Stool culture- Rule out parasites and infectious causes.
- 40. • Endoscopy- Best test for diagnosis. • Full colonoscopy - If diagnosis is unclear. • Flexible sigmoidoscopy- It is sufficient to support the diagnosis. • Endoscopic findings: – – – – – Loss of the vascular appearance of the colon. Erythema and friability of the mucosa. Superficial ulceration, which may be confluent, and Pseudopolyps. Rectum almost universally being involved. Rarely perianal disease.
- 41. • Endoscopic image of a bowel section (the sigmoid colon) affected with ulcerative colitis. • The internal surface of the colon is blotchy and broken in places.
- 42. Histologic Appearance Biopsy sample (H&E stain) – Disease confined to mucosa and sub mucosa. – Increase in substance P in nerve fibers. – Decreased goblet cell mucin. – Marked lymphocytic infiltration (blue/purple) of the intestinal mucosa and architectural distortion of the crypts. – Inflammation of crypts (cryptitis), frank crypt abscesses and hemorrhage or inflammatory cells in the lamina propria.
- 44. D/D • Crohn's disease • Infectious colitis- detected on stool cultures • Pseudomembranous colitis, or Clostridium difficile-associated colitis, • Ischemic colitis• Radiation colitis- previous pelvic radiotherapy • Chemical colitis- harsh chemicals into the colon from an enema or other procedure.
- 45. ULCERATIVE COLITIS: TREATMENT • • • • General: Correction of Hb, fluid, electrolyte, nutrition. Sedative, tranquiliser, psychological counseling. Drugs: – Sulfasalazine/salazopyrine- 2-4 gm/day- induce remissionactive disease. – 5ASA (5-Amino Salicylic Acid/Mesalamine)- Oral/retention enema. – Steroid- In refractory case-oral prednisolon 60mg/d tapering in 4 weeks. – IV hydrocortisone. – Immunmodulators- Azathioprine , 6 mercaptopurine (6MP), Cyclosporin.
- 46. ULCERATIVE COLITIS • Indication for surgery– – – – – – – – – – – Intractability Toxic dilatation Perforation Haemorrhage Risk of malignant transformation Onset at early age Progressive disease Steroid dependency- persistent active disease Malignancy Severe extraintestinal feature Growth retardation in children
- 47. Differentiating features Crohn’s disease Terminal ileum involvement Commonly Ulcerative colitis Seldom Colon involvement Usually Always Rectum involvement Seldom Usually Involvement around the anus Common Seldom Bile duct involvement No increase in rate of primary sclerosing cholangitis Higher rate Distribution of Disease Patchy areas of inflammation (Skip lesions) Continuous area of inflammation Endoscopy Deep geographic and serpiginous (snake-like) ulcer Continuous ulcer May be transmural Shallow, mucosal Common Seldom Depth of inflammation Stenosis Granulomas on biopsy May have non-necrotizing non-peri- Non-peri-intestinal crypt granulomas intestinal crypt granuloma not seen
- 48. ISCHAEMIC COLITIS • • • • • Splenic flexure- watershed area- blood supply precarious. Female. Aged patient. Atherosclerosis ,emboli, vasculitis. Types (Marston’s classification)– Gangrenous- Full thickness. – Stricture- Muscular layer. – Transient- Mucosal involvement.
- 49. • Clinical features: – Pain LIF, LHC. – Vomiting , diarrhoea. – Blood in stool. • Inv– Plain x ray- Thumb print sign – CT • T/t • Conservative-fail-surgery
- 50. The arrow is pointing to thumbprinting in a patient with ischemic colitis. Thumbprinting is a nonspecific finding of mucosal edema, which may be found with inflammatory bowel disease, pseudomembranous colitis, or ischemic bowel. As the edema worsens, the haustral markings may disappear completely, leaving a hoselike appearance to the colon. Narrowing and stricturing are other common findings.
- 51. PSEUDOMEMBRANOUS COLITIS • Toxin of Clostridium difficile– After antibiotic therapy. – Immunocompromised. • Diarrhoea, toxemia, perforation, haemorrhage. • Mortality 30%. • Investigations: – Stool cytotoxin assay, – ELISA, – Colonoscopy. • T/T – Vancomycin, – Metronidazole.
- 52. THANK YOU