Iron deficiency in heart failure

Iron deficiency is an extremely common comorbidity in patients with heart failure, affecting up to 50% of all ambulatory patients. It is associated with reduced exercise capacity and physical well-being and reduced quality of life. Cutoff values have been identified for diagnosing iron deficiency in heart failure with reduced ejection fraction as serum ferritin, <100 μg/l, or ferritin, 100 to 300 μg/l, with transferrin saturation of <20%. Oral iron products have been shown to have little efficacy in heart failure, where the preference is intravenous iron products. Most clinical studies have been performed using ferric carboxymaltose with good efficacy in terms of improvements in 6-min walk test distance, peak oxygen consumption, quality of life, and improvements in New York Heart Association functional class. Data from meta-analyses also suggest beneficial effects for hospitalization rates for heart failure and reduction in cardiovascular mortality rates. A prospective trial to investigate effects on morbidity and mortality is currently ongoing. This paper highlights current knowledge of the pathophysiology of iron deficiency in heart failure, its prevalence and clinical impact, and its possible treatment options

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Iron deficiency in heart failure
Similar to Iron deficiency in heart failure (20)
More from Ramachandra Barik
More from Ramachandra Barik (20)
Recently uploaded
Recently uploaded (20)
Iron deficiency in heart failure
- 1. STATE-OF-THE-ART REVIEW Iron Deficiency in Heart Failure An Overview Stephan von Haehling, MD, PHD,a Nicole Ebner, PHD,a Ruben Evertz, MD,a Piotr Ponikowski, MD, PHD,b Stefan D. Anker, MD, PHDc,d ABSTRACT Iron deficiency is an extremely common comorbidity in patients with heart failure, affecting up to 50% of all ambulatory patients. It is associated with reduced exercise capacity and physical well-being and reduced quality of life. Cutoff values have been identified for diagnosing iron deficiency in heart failure with reduced ejection fraction as serum ferritin, <100 mg/l, or ferritin, 100 to 300 mg/l, with transferrin saturation of <20%. Oral iron products have been shown to have little efficacy in heart failure, where the preference is intravenous iron products. Most clinical studies have been performed using ferric carboxymaltose with good efficacy in terms of improvements in 6-min walk test distance, peak oxygen consumption, quality of life, and improvements in New York Heart Association functional class. Data from meta-analyses also suggest beneficial effects for hospitalization rates for heart failure and reduction in cardiovascular mortality rates. A prospective trial to investigate effects on morbidity and mortality is currently ongoing. This paper highlights current knowledge of the pathophysiology of iron deficiency in heart failure, its prevalence and clinical impact, and its possible treatment options. (J Am Coll Cardiol HF 2019;7:36–46) © 2019 by the American College of Cardiology Foundation. Iron is an essential element for all forms of human life, mostly for its ability to accept and to donate electrons, thereby switching between its ferrous (bivalent, Fe2þ ) and its ferric (trivalent, Fe3þ ) form (1). Iron deficiency (ID), on the other hand, affects up to one-third of the world’s population (2). Populations at high risk include infants, young children, adoles- cents, elderly persons, and women, the last particu- larly during menstrual periods and pregnancy. The past decades have seen tremendous research effort into ID in patients with chronic diseases with underly- ing inflammatory activation, and these efforts have finally yielded the understanding that patients with heart failure (HF), chronic kidney disease, cancer, and inflammatory bowel disease are likewise at increased risk of developing ID. Thus, it is now under- stood that childhood growth and blood loss as well as inflammatory activity, even when only just detectable as cytokine or C-reactive protein activation, are risk factors for ID. This review paper traces the history of ID and iron supplementation in HF and summarizes the available data from clinical trials in order to guide clinicians in their treatment decisions. HISTORY OF TREATING IRON DEFICIENCY IN HF Patients with HF are affected by severely reduced exercise capacity and quality of life. On the lookout for new ways of improving exercise capacity, re- searchers from Tel Aviv started in the late 1990s to ISSN 2213-1779/$36.00 https://doi.org/10.1016/j.jchf.2018.07.015 From the a Department of Cardiology and Pneumology, University of Göttingen Medical Center, Göttingen, Germany; b Department of Heart Diseases, Wroclaw Medical University, Centre for Heart Diseases, Military Hospital, Wroclaw, Poland; c Division of Cardiology and Metabolism-Heart Failure, Cachexia and Sarcopenia, Department of Cardiology, Campus Virchow-Klinikum, Charité-Universitätsmedizin Berlin, Berlin, Germany; and the d Berlin-Brandenburg Center for Regenerative Therapies, Charité- Universitätsmedizin Berlin, Berlin, Germany. Dr. von Haehling has consulted for Vifor Pharma, Roche, Bayer, Brahms; and has received speaker fees from Boehringer Ingelheim, Novartis, Chugai Pharma, and Amgen. Dr. Anker has consulted for Vifor Pharma, Boehringer Ingelheim, Bayer, Servier Pharmaceuticals, and Novartis; and has received grants through his institution from Vifor Pharma, IIT, and Abbott Vascular. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose. Manuscript received March 23, 2018; revised manuscript received June 29, 2018, accepted July 2, 2018. J A C C : H E A R T F A I L U R E V O L . 7 , N O . 1 , 2 0 1 9 ª 2 0 1 9 B Y T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N P U B L I S H E D B Y E L S E V I E R
- 2. treat anemic patients with HF with a combination of subcutaneous erythropoietin and intravenous (IV) iron sucrose (3). Mean hemoglobin concentration, left ventricular ejection fraction (LVEF), and New York Heart Association (NYHA) functional classes improved significantly over 6 months of treatment (3). These findings sparked an avalanche of research into treatment of anemia in HF, culminating in a program of large trials of the novel long-acting erythropoietin derivative darbepoetin-alfa (Online Refs. 1,2). The anemia treatment pathway was ulti- mately left only after a large trial of darbepoetin-alfa ended in disappointment. Indeed, the RED-HF (Reduction of Events by Darbepoetin Alfa in Heart Failure) study, a randomized, double-blind, placebo- controlled trial in 2,278 patients with systolic HF and mild to moderate anemia did not show any improvement in the primary endpoint of death from any cause or hospitalization for worsening HF; how- ever, there was an increased rate of thromboembolic events (13.5% vs. 10.0%, respectively; p ¼ 0.009) and an increased risk of ischemic stroke (4.5% vs. 2.8%, respectively; p ¼ 0.03) (4). In retrospect, it can be said that the early study design, consisting of a combina- tion therapy of erythropoietin and IV iron, hampered the discovery that ID treatment may be worthwhile even in the absence of anemia. Shortly before the results of RED-HF were pub- lished, a small open-label, nonrandomized, noncon- trolled study in 16 patients with hemoglobin of #12 g/dl and ferritin of #400 mg/l in NYHA functional class II (56%) or III (44%) using IV iron administration alone showed improvements in quality of life and physical well-being over 3 months of follow-up (5). At the end of the study, all patients were in NYHA functional class II, their hemoglobin had risen, and their quality-of-life score had improved. This point is interesting, because the trials of darbepoetin-alfa had all underutilized iron. Therefore, the confir- mation of these early results in a double-blind, randomized, placebo-controlled trial in 40 patients with symptomatic HF was important (6). Another small, randomized, observer-blinded study of IV iron sucrose also showed that improvements in exercise capacity measured by spiroergometry were possible (Online Ref. 3). DIAGNOSING IRON DEFICIENCY IN HF The dilemma of correctly diagnosing ID arises from the distinction between stored and circulating iron and from the difference between mobilizable and immobilizable iron. Because chronic HF, like chronic kidney disease, inflammatory bowel disease, or cancer, has been associated with increased systemic inflammation, the patient’s status plays an important role leading to functional ID. Hepcidin, a peptide encoded by the HAMP gene on chromosome 19 and secreted chiefly by hepatocytes, is the main regulator of iron uptake and release (1). Hepcidin controls the activity of ferroportin, a transmembrane iron exporter out of different cell types, that is, at the site of iron absorption (gut mucosa cells in the duo- denum), as well as at the site of iron storage (hepa- tocytes, macrophages). Once ferroportin is bound by hepcidin, it is destroyed in the lysosome, leading to reduced iron release (7). Because bacteria are largely dependent on the presence of iron for reproduction, the peptide that inhibits its uptake and its mobiliza- tion during periods of increased inflammatory activity was originally named liver-expressed anti- microbial protein (LEAP)-1. It was discovered in 2000 and later renamed hepatic bactericidal protein, or hepcidin. When research of ID started in cardiology, it was unclear how to correctly arrive at its diagnosis. Reli- able cutoff values were not available for HF but only for kidney disease or cancer. Early studies of ID in HF, therefore, used a ferritin concentration of #400 mg/l or <100 mg/l or a combination of ferritin concentra- tions ranging between 100 and 299 mg/l together with a transferrin saturation (TSAT) level of <20% as identifying criterion. After the latter cutoff values were validated in a double-blind trial, they were accepted and have been entered into the HF guide- lines of the European Society of Cardiology (ESC) (8). Consequently, current ESC HF guidelines give a Class Ic recommendation to screen all HF patients for the presence of ID by using serum ferritin and TSAT measurement (8). Because these values are signifi- cantly different from the cutoff values used in sub- jects without chronic inflammation (usually ferritin concentration of <20 mg/l), the point of alternative diagnostic cutoffs is worth stressing. Treatment should be considered regardless of the presence of anemia. Table 1 highlights the most important cutoff values for diagnosing ID across different clinical en- tities in internal medicine. PREVALENCE AND CLINICAL EFFECTS OF IRON DEFICIENCY IN HF ID is highly prevalent in patients with chronic and acute HF; however, studies have used different defi- nitions (13). A Canadian study in 12,065 patients with newly diagnosed HF found 21% of all anemic patients had absolute ID, as detected using discharge A B B R E V I A T I O N S A N D A C R O N Y M S HF = heart failure ID = iron deficiency LVEF = left ventricular ejection fraction J A C C : H E A R T F A I L U R E V O L . 7 , N O . 1 , 2 0 1 9 von Haehling et al. J A N U A R Y 2 0 1 9 : 3 6 – 4 6 Iron Deficiency in Heart Failure 37
- 3. international classification of disease codes, implying complete or nearly complete depletion of iron stores (Online Ref. 4). Nanas et al. (Online Ref. 5), on the other hand, showed that a diagnosis based on serum values of ferritin might be misleading. Those authors used bone marrow biopsies from 37 anemic patients with end-stage HF. They found that 27 patients (73%) presented with ID in the bone marrow, even though they had normal or nearly normal serum ferritin levels. Several studies have applied the defining criteria named above, that is, serum ferritin of <100 mg/l or serum ferritin ranging from 100 to 299 mg/l in combination with a TSAT value of <20%. Using data from 546 consecutive ambulatory patients TABLE 1 Relevant Cut-Offs for the Diagnosis of ID in Different Fields of Internal Medicine Clinical Trial Completed Completed Completed Completed Completed Completed Completed Study name (Ref. #) FERRIC-HF (Online Ref. 3) Toblli et al. (6) FAIR-HF (9) CONFIRM-HF (10) EFFECT-HF (11) IRON5 IRONOUT (12) ClinicalTrial.gov reference NCT00125996 NCT00520780 NCT01453608 NCT01394562 NCT02998697 NCT02188784 Diagnosis HFrEF HFrEF HFrEF HFrEF HFrEF HF HFrEF Number of patients 35 40 459 304 174 54 225 Randomization 2:1 (iron:placebo) 1:1 (iron:placebo) 2:1 (FCM:placebo) 1:1 (FCM:placebo) 1:1 (FCM:standard of care) 1:1 (iron:placebo) 1:1 (FCM:placebo) Blinding Double-blind Double-blind Double-blind Double-blind Open-label Double-blind Double-blind Symptoms NYHA functional class II–III NYHA functional class II–IV NYHA functional class II–III NYHA functional class II–III NYHA functional class II–III NYHA functional class II–III NYHA functional class II–IV LVEF #45% #35% #40% in NYHA functional class I, #45% in NYHA functional class III #45% #45% <50% #40 Definition of iron deficiency Serum ferritin <100 ng/ml, or serum ferritin 100–299 ng/ml with TSAT <20% TSAT <20%, ferritin <100 ng/ml Serum ferritin <100 ng/ml, or serum ferritin 100–299 ng/ml with TSAT <20% Serum ferritin <100 ng/ml, or serum ferritin 100–299 ng/ml with TSAT <20% Serum ferritin <100 ng/ml, or serum ferritin 100– 299 ng/ml with TSAT <20% Serum ferritin <100 ng/ml or 100– 300 ng/ml with TSAT <20% Serum ferritin <100 ng/ml, or serum ferritin 100–299 ng/ml with TSAT <20% Hemoglobin <12.5 g/dl anemic group, 12.5– 14.5 g/dl non anemic group <12.5 g/dl $9–#13.5 g/dl <15 g/dl #15 g/dl >8 and <13 g/dl for men and <12 g/dl for women $9.0–#13.5 g/dl Natriuretic peptides Not included NT-proBNP Not included BNP >100 pg/ml, NT-proBNP >400 pg/ml BNP >100 pg/ml, NT-proBNP >400 pg/ml NT-proBNP >4,000 pg/ml NT-proBNP Duration 16 weeks 25 weeks 24 weeks 52 weeks 24 weeks 90 days 16 week Dosage Iron sucrose 200 mg weekly until ferritin >500 ng/ml Iron sucrose 200 mg weekly for 5 weeks 200 mg ferric carboxymaltose 200 mg ferric carboxymaltose 500 mg ferric carboxymaltose 3 times Ferrous sulfate 200 mg 3 times daily for 90 days 150 mg oral iron polysaccharide iron complex (Feramax) twice daily Primary end point Change in absolute pVO2 (ml/min) from baseline to week 18 Change in the NT-proBNP level and inflammatory status by CRP Change in self- reported PGA score and NHYA class from baseline to week 24 Change in 6-min walk distance from baseline to week 24 Change in peak VO2 from baseline to week 24 Change in 6MWT from baseline to 90 days Change in peak VO2 from baseline to week 16 BNP ¼ B-type natriuretic peptide; FCM ¼ ferric carboxymaltose; Hb ¼ hemoglobin; HF ¼ heart failure; HFpEF ¼ heart failure with preserved ejection fraction; HFrEF ¼ heart failure with reduced ejection fraction; LVEF ¼ left ventricular ejection fraction; MR-proANP ¼ mid-reginal atrial natriuretic peptide prohormone; NT-proBNP ¼ N-terminal BNP prohormone; NYHA ¼ New York Heart Association; PGA ¼ patient global assessment; TSAT ¼ transferrin saturation. von Haehling et al. J A C C : H E A R T F A I L U R E V O L . 7 , N O . 1 , 2 0 1 9 Iron Deficiency in Heart Failure J A N U A R Y 2 0 1 9 : 3 6 – 4 6 38
- 4. with HF, Jankowska et al. (14) found ID was present in 37%. Another study, in outpatients in German office- based cardiology practices, using data from 1,198 pa- tients with HF, found a prevalence of ID reaching 42.5% (15). Acknowledged risk factors for the devel- opment of ID include female sex, a more advanced stage of HF, higher levels of N-terminal-proB-type natriuretic peptide (NT-proBNP), and higher serum levels of C-reactive protein (14). In addition, the presence of ID is an independent predictor of poor exercise capacity (15) and worse survival (14,16). IRON METABOLISM IN HUMANS Iron itself is potentially toxic, because intracellular reduction of molecular oxygen leads to the formation TABLE 1 Continued Clinical Trial Recruiting Recruiting Recruiting Recruiting Recruiting Recruiting Recruiting FAIR-HFpEF FAIR-HF 2 AFFIRM-AHF HEART-FID IRONMAN NCT03074591 NCT03036462 NCT02937454 NCT03037931 NCT01978028 NCT02642562 NCT03218384 HFpEF HFrEF AHF after restabilization HFrEF HFrEF HFrEF HFrEF 200 1,200 1,100 3,014 20 1,300 32 1:1 (FCM:placebo) 1:1 (FCM:placebo) 1:1 (FCM:placebo) 1:1 (FCM:placebo) 1:1 (FCM:placebo) 1:1 (iron:placebo) 1:1 (FCM:placebo) Double-blind Double-blind Double-blind Double-blind Double-blind Open label Double-blind NYHA functional class II-III NYHA functional class II-III NYHA functional class II-III NYHA functional class III-IV NYHA functional class II-III NYHA functional class II-IV NYHA functional class II-III $45% together with evidence of diastolic dysfunction #45% <50% #35% #40% <45% <40% or $40% with left atrial volume index >28 ml/m2 ) and/or left ventricular mass index >95 g/m2 (women) or >115 g/m2 (men) Serum ferritin <100 ng/ml, or serum ferritin 100–299 ng/ml with TSAT <20% Serum ferritin <100 ng/ml, or serum ferritin 100–299 ng/ml with TSAT <20% Serum ferritin <100 ng/ml, or serum ferritin 100–299 ng/ml with TSAT <20% Serum ferritin <100 ng/ml or 100–300 ng/ml with TSAT <20% Serum ferritin <100 ng/ml, or serum ferritin 100–299 ng/ml with TSAT <20% TSAT <20% and/or ferritin <100 mg/l Serum ferritin <100 ng/ml, or serum ferritin 100–299 ng/ml with TSAT <20% >9–#14 g/dl $9.5–#14 g/dl $8–#15 g/dl >9.0 and <13.5 g/dl (women) or <15.0 g/dl (men) 9.5-13.5 g/dl >9.0 and <13.5 g/dl (women) or <15.0 g/dl (men) <13 g/dl for men and <12 g/dl for women BNP >100 pg/ml, NT-proBNP >400 pg/ml, MR-proANP >125 pmol/l Not included Not included NT-proBNP >600 pg/ml or BNP >200 pg/ml for patients with normal sinus rhythm or NT-proBNP >1,000 pg/ml (or BNP >400 pg/ml) for patients with atrial fibrillation Not included NT-proBNP >250 ng/l in sinus rhythm or >1,000 ng/l in atrial fibrillation (or BNP of >75 pg/ml or 300 pg/ml, respectively Not included 52 weeks Event driven 52 weeks Event driven 12 weeks 120 weeks 4 weeks 500–2,000 mg ferric carboxymaltose according to Hb and weight value 500–2,000 mg ferric carboxymaltose according to Hb and weight value 500–1,500 mg ferric carboxymaltose according to Hb and weight value 500–2,000 mg ferric carboxymaltose according to Hb and weight value 500–2,000 mg ferric carboxymaltose according to Hb and weight value Iron (III) isomaltoside 1,000 750 mg ferric carboxymaltose Change in 6-min walk distance from baseline to week 24 Combined rate of recurrent hospitalizations for HF and of cardiovascular death from baseline to at least 12 months of follow-up HF hospitalizations and cardiovascular death up to 52 weeks after randomization Incidence of death and incidence of hospitalization for heart failure at least 12monthsoffollow-up and change in 6MWT distance after 6 months Evaluate the effect of ferric carboxymaltose on mitochondrial gene activation pattern after 12 weeks of treatment CV mortality or hospitalization for worsening heart failure Change in skeletal muscle mitochondrial oxidative capacity J A C C : H E A R T F A I L U R E V O L . 7 , N O . 1 , 2 0 1 9 von Haehling et al. J A N U A R Y 2 0 1 9 : 3 6 – 4 6 Iron Deficiency in Heart Failure 39
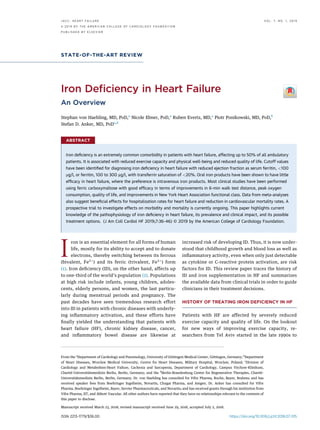
- 5. of reactive oxygen species. Therefore, intracellular and intravascular iron requires a “detoxifier,” intra- cellularly in the form of ferritin and intravascularly by binding to transferrin. Intravenously adminis- tered iron preparations likewise require such a “detoxifier” that usually has a composition similar to the “envelope” function of ferritin (Figure 1). Side effects of IV iron usually occur as a result of the “envelope” composition rather than as a result of the iron itself. Oral iron tablets are prone to cause gastrointes- tinal side effects, mostly as a result of direct iron effects on the gut wall. Indeed, most oral iron preparations contain ferrous iron (Fe2þ ) that is directly absorbed through divalent metal transporter (DMT)-1 into the gut mucosa cell. Nonheme (ferric) iron present in vegetables and fruits is less well absorbed and requires reduction by ferrireductase, an enzyme likewise present in the gut mucosa, before absorption. Ferrous iron (Fe2þ ), however, cannot bind to transferrin and ferritin, and therefore a reduction is necessary to enable such binding (Figure 2) (17). Inside the human body, iron not only plays a role in oxygen transport but also in skeletal muscle, the thyroid gland, the central nervous system, and in immune function. In a single person, the overall amount of iron is approximately 3 to 5 g, two-thirds of which resides inside hemoglobin (18). Stored iron bound to ferritin in several cell types has a much smaller part: 800 to 1,000 mg in men and 300 to 500 mg in women, thus explaining the higher prevalence of ID in female patients. With regard to function, the body always prioritizes the use of iron for metabolic purposes, with erythropoiesis having relative priority over other functions (19). Because no means of iron excretion exists, only the uptake in the duodenum and the upper jejunum is regulated (20). Normal food contains mostly nonheme (Fe3þ ) iron, approximately 5 to 6 mg per 1,000 kcal, a form that is less well absorbed than heme iron (Fe2þ ) found in meat (Online Ref. 6). Daily consumption is approximately 12 to 15 mg, but only 1 to 2 mg of this is ultimately absorbed. ESTIMATING THE IRON DEFICIT Conventionally, the iron deficit seen in patients with chronic disease had been estimated using Ganzoni’s formula published in 1970 (21). This equation assumes an ideal (target) hemoglobin value of 15.0 g/dl (body weight of >35 kg) or 13.0 g/dl (lower body weight). Because Ganzoni’s formula does not consider replenishment of iron stores, an extra depot dose of 500 mg is usually added, as follows: Iron deficit ðmgÞ ¼ ½body weight ðkgÞ Â ðtarget Hb À actual HbÞ Â 2:4 þ depot ironŠ The calculated result is 1,000 mg or higher in most cases. Therefore, modern IV iron products provide guidance for dosages listed in the drug information sheet. Ferric carboxymaltose, for example, is usually administered at a dose between 1,000 and 2,000 mg to replenish iron stores; however, dosages should not exceed 1,000 mg per week, which implies that a heavy patient needs to return for a second dose in the week after the first dose. ORAL IRON THERAPY Oral iron preparations usually contain Fe2þ (Online Ref. 7). Problems include the small amount of iron absorbed in the gut, a metallic taste, and the fact that up to 40% of patients experience side effects, most frequently gastrointestinal discomfort such as nausea, flatulence, abdominal pain, diarrhea, constipation, and black staining of the stool (Online Ref. 8). Oral iron preparations should be taken 30 to 60 mins before to meals because iron absorption is highest in the fasting state. The normal dosage is 100 to 200 mg per day. Success is usually assumed when an increase in reticulocytes or hemoglobin is observed after 1 or 3 weeks, respectively. Replenishing iron stores usually takes 2 to 6 months (Online Ref. 9). Two clinical studies evaluated the use of oral iron preparations in patients with HF. The first study, published in 2013, was named IRON 5-(Short Term Oral Iron Supplementation in Systolic Heart Failure Patients Suffering From Iron Deficiency Anemia) HF and enrolled patients with an LVEF of <40% in NYHA functional classes II to IV who had a hemo- globin concentration between 9 and 12 g/dl, a TSAT level of >20%, and a ferritin concentration of <500 mg/l. Patients were randomized to 1 of 3 groups: 1) an oral ferrous sulfate therapy, 200 mg 3 times daily, plus IV placebo; 2) an oral placebo plus IV iron sucrose, 200 mg weekly; or 3) an oral and IV placebo. Oral iron was administered over 8 weeks and IV iron over 5 weeks. The calculated sample size was 39 per group, making it the only clinical study in HF to compare IV and oral iron supplementation. All treat- ments were performed in a double-blinded fashion (Online Ref. 10). Unfortunately, the trial was termi- nated early after prolonged recruitment and funding problems, with only 23 patients in the database. von Haehling et al. J A C C : H E A R T F A I L U R E V O L . 7 , N O . 1 , 2 0 1 9 Iron Deficiency in Heart Failure J A N U A R Y 2 0 1 9 : 3 6 – 4 6 40
- 6. A significant increase in the patients’ peak oxygen consumption was noted in the IV iron group after 3 months but not in the other groups (22). The mean change in the patients’ TSAT level was 10 percentage points with IV iron and 5 and 2 percentage points with oral iron and placebo, respectively. Serum ferritin increased from 167 Æ 149 mg/l to 293 Æ 270 mg/l in the IV iron group and from 115 Æ 141 to 218 Æ 189 mg/l in the oral iron group, but only the latter change was statistically significant. These data, however, need to be interpreted with caution, as most of the nonsig- nificant results are probably explained by b-error. The second trial to use oral iron therapy in HF was the IRONOUT HF (Oral Iron Repletion Effects On Ox- ygen Uptake in Heart Failure) trial, a phase II double- blind, randomized, placebo-controlled trial of 225 patients with HF, an LVEF of <40%, and ID defined as ferritin concentration of 15 to 100 mg/l or ferritin 101 to 299 mg/l with TSAT of <20% (12). Patients received oral iron polysaccharide, 150 mg twice daily over 16 weeks. The primary endpoint of the trial, a change in peak oxygen uptake from baseline to 16 weeks, was not significantly different between the 2 groups at the end of follow-up (iron: þ23 ml/min vs. placebo: À2 ml/min; p ¼ 0.5). Likewise, no significant change was noted for the secondary endpoints, 6-min walk test and NT-proBNP levels. A mild increase in serum ferritin (þ11.3 mg/l; p ¼ 0.06) and TSAT (þ3.3%; p ¼ 0.003) was noted with oral iron therapy (12). The authors concluded that “these results do not support use of oral iron supplementation in patients with HF with reduced ejection fraction.” INTRAVENOUS IRON THERAPY Since the beginning of ID treatment in HF, oral iron preparations were not the most promising treatment approach due to pathophysiological considerations such as the established overactivity of inflammatory mediators in HF (23). Indeed, serum levels of tumor necrosis factor (TNF) and interleukin (IL)-6 are known to be elevated in patients with HF and are indepen- dent predictors of poor survival (Online Ref. 11). In addition, the gut wall itself has been shown to display increased thickness in cases of HF (Online Ref. 12). Therefore, early intervention trials were carried out with IV iron treatment using 1 of the several different formulations available on the market. Presently, the usual route of administration is the IV route, and treatment options are iron(III) gluconate, iron(III) hydroxide sucrose, iron(III) hydroxide polymaltose complex (ferric carboxymaltose), and ferumoxytol (Online Ref. 13). A combination of the products in 1 sitting is generally not recommended. The latest additions to the portfolio, that is, iron sucrose, ferric carboxymaltose, and ferumoxytol, permit the appli- cation of higher doses of iron in 1 sitting. Most studies in patients with HF and ID have used either iron su- crose (maximum dose in 1 sitting: 200 mg) or ferric carboxymaltose (1,000 mg). Iron dextran does not play a major role anymore in clinical routine (24). The early small studies of IV iron in HF are sum- marized in Table 2 and Figure 3. The first large-scale, double-blind, placebo-controlled multicenter trial of ferric carboxymaltose in patients with chronic HF was published in 2009 (Online Ref. 14). This study, the FAIR-HF (Ferinject Assessment in patients with IRon deficiency and chronic Heart Failure) trial recruited 459 patients in NYHA functional class II (LVEF #40%) or NYHA functional class III (LVEF #45%). With a hemoglobin concentration ranging between 9.5 and 13.5 g/dl, the recruitment of anemic patients was not a prerequisite. Patients had to have ID, defined as serum ferritin of <100 mg/l or ferritin ranging from 100 to 300 mg/l, with TSAT of <20%. Patients were randomly allocated in a 2:1 fashion to receive IV ferric carboxymaltose or placebo and entered the trial in the so-called correction phase, during which their calcu- lated iron deficit (Ganzoni’s formula) was replenished by weekly doses of 200 mg. A maintenance phase was added during which patients received 200 mg of ferric carboxymaltose per month. After 24 weeks of follow- up, 50% of patients in the ferric carboxymaltose group had improved according to the self-reported patient global assessment (PGA), the primary end point of the study, compared to 28% in the placebo group (odds ratio [OR] for being in a better rank: 2.51; FIGURE 1 Principal Structure of Ferritin and Intravenous Iron J A C C : H E A R T F A I L U R E V O L . 7 , N O . 1 , 2 0 1 9 von Haehling et al. J A N U A R Y 2 0 1 9 : 3 6 – 4 6 Iron Deficiency in Heart Failure 41
- 7. 95% confidence interval [CI]: 1.75 to 3.61; p < 0.001) (27). The PGA describes the patient’s overall well- being compared to the last assessment. Secondary endpoints included NYHA functional class, 6-min walk distance, and quality of life as assessed by the Kansas City Cardiomyopathy Questionnaire and showed, likewise, a statistically significant improve- ment. These effects were seen regardless of whether anemia was present at baseline. Publication of the FAIR-HF study results yielded the first recommen- dation to consider IV ferric carboxymaltose in the 2012 ESC HF guidelines (Online Ref. 15), which followed the 2011 update of the National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand guidelines for the management of HF (grade B recommendation) (Online Ref. 16). The second large-scale trial of ferric carbox- ymaltose in HF, the CONFIRM-HF (ferric Carbox- ymaltOse evaluatioN on perFormance in patients with IRon deficiency in coMbination with chronic Heart Failure) trial, showed results very similar to those of the FAIR-HF study. Likewise, CONFIRM-HF was a double-blind, multicenter, prospective, ran- domized controlled trial that enrolled ambulatory patients with symptomatic HF in NYHA functional class II or III with an LVEF of #45% and an elevated level of either NT-proBNP or B-type natriuretic pep- tide (BNP) (Online Ref. 17). Patients received between 500 and 2,000 mg of iron or placebo within the first 6 weeks in the study. Thereafter, patients received 500 mg of ferric carboxymaltose at each visit in weeks 12, 24, and 36 if ferritin and/or TSAT still indicated ID (Online Ref. 17). Randomization was performed in 1:1 fashion, and treatment duration was 52 weeks. The primary endpoint was the change in the 6-min walking distance from baseline to 24 weeks. Addi- tional assessments were done at 6, 36, and 52 weeks, also including secondary endpoints such as PGA score and safety. At 24 weeks, patients in the ferric car- boxymaltose group had a significantly greater FIGURE 2 Iron Uptake in the Duodenum and Release Iron uptake in the duodenum and iron release from cells of the reticuloendothelial system by ferroportin, whose expression is tightly regulated by the expression of the acute-phase reactant hepcidin. Adapted from von Haehling (17). TABLE 2 Published and Ongoing Clinical Trials in HF With Relevance for ID Treatment Illness TSAT, % Ferritin, mg/l No underlying illness <30 Chronic HF - <100 <20 100–299 Inflammatory bowel disease Without increased activity <20 <30 With increased activity <20 <100 Chronic kidney disease Treated with dialysis <25 <200 Without dialysis <25 <300 Cancer and chemotherapy-associated anemia Without inflammatory activity <20 <100 With inflammatory activity <20 $100 Adapted from von Haehling et al. (9). HF ¼ heart failure; ID ¼ iron deficiency; TSAT ¼ transferrin saturation. von Haehling et al. J A C C : H E A R T F A I L U R E V O L . 7 , N O . 1 , 2 0 1 9 Iron Deficiency in Heart Failure J A N U A R Y 2 0 1 9 : 3 6 – 4 6 42
- 8. improvement in their 6-min walk distances than pa- tients taking placebo (difference: 33 Æ 11 m; p ¼ 0.002), and this effect was maintained to week 52 (28). A more recent clinical study named EFFECT-HF (Effect of ferric carboxymaltose on exercise capacity in patients with chronic heart failure and iron defi- ciency) (29) showed that IV administration of ferric carboxymaltose can also improve patients’ peak ox- ygen consumption, as measured by spiroergometry (2). A total of 174 patients were randomized, unfor- tunately in a nonblinded fashion, to ferric carbox- ymaltose therapy or standard of care (i.e., no intervention) and were followed for 24 weeks. Most patients were in NYHA functional class II at baseline. Ferric carboxymaltose significantly increased serum ferritin and transferrin saturation. At 24 weeks, peak oxygen consumption had decreased in the control group (least square means: À1.19 Æ 0.389 ml/min/kg) but was maintained in the ferric carboxymaltose group (À0.16 Æ 0.387 ml/min/kg; p ¼ 0.02). This result was achieved by imputation of missing data by the last-observation-carried-forward approach. In a sensitivity analysis, in which missing data were not imputed, peak oxygen consumption at 24 weeks decreased by À0.63 Æ 0.375 ml/min/kg in the control group and by À0.16 Æ 0.373 ml/min/kg in the IV iron group; p ¼ 0.23. Two meta-analyses were published between 2016 and 2017 with regard to IV iron treatment in HF. Jan- kowska et al. (30) included 5 clinical studies yielding a total number of 851 patients, 509 of whom received iron sucrose or ferric carboxymaltose. IV iron therapy was found to reduce the risk of the combined endpoint of all-cause death or cardiovascular hospitalization (OR: 0.44; 95% CI: 0.30 to 0.64; p < 0.0001) and the combined endpoint of cardiovascular death or hospi- talization for worsening HF (OR: 0.39; 95% CI: 0.24 to 0.63; p ¼ 0.0001). With regard to overall well-being and quality of life, IV iron therapy resulted in a reduction in NYHA functional class (p ¼ 0.001), an increase in the 6-min walking test distance (þ31 m; 95% CI: 18 to 43; p < 0.0001), and an improvement in quality of life, using different assessment tools (all p # 0.01) (30). A second meta-analysis was published in 2017, using data from 4 randomized controlled trials including 839 patients, 504 of whom had received ferric carboxymaltose (31). Patients taking ferric carboxymaltose had lower rates of recurrent cardiovascular hospitalizations and cardiovascular mortality (OR: 0.59; 95% CI: 0.40 to 0.88; p ¼ 0.009). Treatment with ferric carboxymaltose also reduced recurrent HF hospitalizations and cardiovascular mortality (OR: 0.53; 95% CI: 0.33 to 0.86; p ¼ 0.011) and recurrent cardiovascular hospitalizations and FIGURE 3 Major Publications in the Field of Iron Deficiency and Anemia in Heart Failure J A C C : H E A R T F A I L U R E V O L . 7 , N O . 1 , 2 0 1 9 von Haehling et al. J A N U A R Y 2 0 1 9 : 3 6 – 4 6 Iron Deficiency in Heart Failure 43
- 9. all-cause mortality (OR: 0.60; 95% CI: 0.41 to 0.88; p ¼ 0.009) (31). These data suggest beneficial effects of IV iron treatment in HF and led to designing the prospective FAIR-HF 2 trial with a primary endpoint of the combined rate of recurrent hospitalizations for HF and of cardiovascular death. The trial is currently ongoing and aims to recruit 1,200 patients. TREATMENT OF IRON DEFICIENCY IN HF GUIDELINES Since 2012, the ESC guidelines have recommended that all patients with HF should undergo testing for ID by using serum assessment of ferritin and TSAT (Online Ref. 17). Anemia should be ruled out by using full blood count assessment, both are Class I, Level of Evidence: C recommendations. This point has not been changed in the 2016 version of the guidelines (8), in which the treatment recommendation had been updated after the publication of the CONFIRM- HF trial to Class IIa, Level of Evidence: A. The state- ment reads, “IV ferric carboxymaltose should be considered in symptomatic patients (serum ferritin <100 mg/l, or ferritin between 100 to 299 mg/l and TSAT <20%) in order to alleviate HF symptoms and improve exercise capacity and quality of life” (8). The Central Illustration shows the diagnostic algo- rithm for the treatment of iron deficiency in patients with HF as recommended by current ESC guidelines (32). The joint guidelines of the American Heart As- sociation and American College of Cardiology pub- lished in 2013 were less enthusiastic (33); however, the 2017 update now states that “in patients with NYHA functional class II and III HF and iron defi- ciency (ferritin <100 mg/l or 100 to 300 mg/l if TSAT is <20%), IV iron replacement might be reasonable to improve functional status and quality of life giving this recommendation a IIb level of evidence” (34). The European guidelines currently advocate only the use of ferric carboxymaltose, because large-scale tri- als have been undertaken, and the drug’s safety has been demonstrated in the HF population only with this drug. The U.S. guidelines do not mention a spe- cific type of iron but rather mention IV iron admin- istration. Previous smaller trials have also used other iron preparations, particularly iron sucrose, but large- scale trials that could have been considered by the guideline committees are still missing. Therefore, it remains unclear if these are able to achieve similar results. CONCLUSIONS AND OUTLOOK ID in HF with reduced ejection fraction has received increasing attention over the last 18 years. The prev- alence of ID reaches 50% among ambulatory patients with HF, and ID is an independent predictor of reduced exercise capacity, quality of life, and sur- vival. Risk factors include female sex, more advanced stage of HF, higher levels of NT-proBNP, and higher serum levels of C-reactive protein. Relevant cutoff values are ferritin of <100 mg/l or ferritin 100 to 300 mg/l when TSAT is <20%. It has been convincingly shown that IV iron application leads to improvements in quality of life, physical well-being, and exercise capacity. Most studies, particularly those of relevant size, have been conducted with ferric carboxymaltose and have good overall safety profiles. Data from 2 meta-analyses suggest beneficial effects in terms of reduced hospitalization rates for HF and cardiovas- cular mortality. A large-scale prospective morbidity and mortality trial is underway. The situation in HF with preserved ejection fraction (HFpEF) is less clear, and another prospective trial, the FAIR-HFpEF trial commenced recruitment late in November 2017. Likewise, uncertainty remains with regard to the CENTRAL ILLUSTRATION Diagnostic Algorithm for Treatment of Iron Deficiency in Patients With HF According to ESC Guidelines and Expert Consensus Recommendations * If significant anemia, initiate evaluation ** Re-evaluate iron status after 3-6 months Symptomatic HFrEF NYHA II-III yes no no yes yes Hemoglobin <15 g/dL* Ferritin <100 µµg/L or Ferritin 100-299 µµg/L with TSAT <20% Consider IV iron treatment** No IV iron treatment von Haehling, S. et al. J Am Coll Cardiol HF. 2019;7(1):36–46. Adapted with permission from Doehner et al. (32). *If anemia is significant, initiate an evaluation. **Re-evaluate iron status after 3 to 6 months (Online Ref. 18). HFrEF ¼ heart failure with reduced ejection fraction; IV ¼ intravenous; NYHA ¼ New York Heart Association. von Haehling et al. J A C C : H E A R T F A I L U R E V O L . 7 , N O . 1 , 2 0 1 9 Iron Deficiency in Heart Failure J A N U A R Y 2 0 1 9 : 3 6 – 4 6 44
- 10. ideal timepoint of IV application after cardiac decompensation. The AFFIRM-AHF (Study to Compare Ferric Carboxymaltose With Placebo in Pa- tients With Acute Heart Failure and Iron Deficiency) trial, a randomized, double-blind placebo-controlled trial comparing the effect of IV ferric carboxymaltose in patients with ID who are hospitalized for acute HF, is aimed at elucidating effects on hospitalization rates and mortality in this population. Table 2 highlights published and currently ongoing studies with rele- vance to ID in HF. For the time being, it appears sensible to test all symptomatic patients with HF with reduced ejection fraction for the presence of ID. A full blood count needs to be performed as well. When ID is diag- nosed, IV ferric carboxymaltose can be administered as a bolus injection or as an infusion over 15 mins. The label permits the use of ferric carboxymaltose up to a hemoglobin concentration of 15 g/dl. A single dosage cannot exceed 1,000 mg per week; dilutions can be made in 0.9% sodium chloride. A typical response is a sharp increase in the patient’s ferritin level following the infusion, which can easily exceed 500 mg/l and will decline only very slowly over several weeks to months. Reassessment of iron sta- tus is useful after approximately 3 to 6 months. However, whether this time frame is optimal has not been prospectively tested, and it remains unclear if 1,000 mg or higher doses are optimal for all patients. ADDRESS FOR CORRESPONDENCE: Prof. Stephan von Haehling, Department of Cardiology and Pneu- mology, University of Göttingen Medical School, Robert-Koch-Strasse 40, D-37075 Göttingen, Germany. E-mail: stephan.von.haehling@web.de. R E F E R E N C E S 1. Crielaard BJ, Lammers T, Rivella S. Targeting iron metabolism in drug discovery and delivery. Nat Rev Drug Discov 2017;16:400–23. 2. Stoltzfus RJ. Defining iron-deficiency anemia in public health terms: time for reflection. J Nutr 2001;131:565S–7S. 3. Silverberg DS, Wexler D, Blum M, et al. The use of subcutaneous erythropoietin and intravenous iron for the treatment of the anemia of severe, resistant congestive heart failure improves cardiac and renal function and functional cardiac class, and markedly reduces hospitalizations. J Am Coll Cardiol 2000;35:1737–44. 4. Swedberg K, Young JB, Anand IS, et al., for the RED-HF Committees; RED-HF Investigators. Treatment of anemia with darbepoetin alfa in systolic heart failure. N Engl J Med 2013;368: 1210–9. 5. Bolger AP, Bartlett FR, Penston HS, et al. Intravenous iron alone for the treatment of anemia in patients with chronic heart failure. J Am Coll Cardiol 2006;48:1225–7. 6. Toblli JE, Lombraña A, Duarte P, Di Gennaro F. Intravenous iron reduces NT-pro-brain natriuretic peptide in anemic patients with chronic heart failure and renal insufficiency. J Am Coll Cardiol 2007;50:1657–65. 7. Andrews NC. Closing the iron gate. N Engl J Med 2012;366:376–7. 8. Ponikowski P, Voors AA, Anker SD, et al., for the Authors/Task Force Members; Document Re- viewers. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail 2016;18:891–975. 9. von Haehling S, Ottenjann H, Anker SD. Iron deficiency: Recognition and treatment. Internist (Berl) 2017;58:627–38. 10. Silverberg DS, Wexler D, Sheps D, et al. The effect of correction of mild anemia in severe, resistant congestive heart failure using subcu- taneous erythropoietin and intravenous iron: a randomized controlled study. J Am Coll Cardiol 2001;37:1775–80. 11. Kalra PR, Bolger AP, Francis DP, et al. Effect of anemia on exercise tolerance in chronic heart failure in men. J Am Coll Cardiol 2003;91:888–91. 12. Lewis GD, Malhotra R, Hernandez AF, et al., for the NHLBI Heart Failure Clinical Research Network. effect of oral iron repletion on exercise capacity in patients with heart failure with reduced ejection fraction and iron deficiency: the IRONOUT HF randomized clinical trial. JAMA 2017;317: 1958–66. 13. Ebner N, von Haehling S. Iron deficiency in heart failure: a practical guide. Nutrients 2013;5: 3730–9. 14. Jankowska EA, Rozentryt P, Witkowska A, et al. Iron deficiency: an ominous sign in patients with systolic chronic heart failure. Eur Heart J 2010;31:1872–80. 15. von Haehling S, Gremmler U, Krumm M, et al. Prevalence and clinical impact of iron deficiency and anaemia among outpatients with chronic heart failure: The PrEP registry. Clin Res Cardiol 2017; 106:436–43. 16. Klip IT, Comin-Colet J, Voors AA, et al. Iron deficiency in chronic heart failure: an international pooled analysis. Am Heart J 2013;165:575–82. 17. von Haehling S, Jankowska EA, van Veldhuisen DJ, Ponikowski P, Anker SD. Iron deficiency and cardiovascular disease. Nat Rev Cardiol 2015;12:659–69. 18. Ganz T, Nemeth E. Iron imports. IV. Hepcidin and regulation of body iron metabolism. Am J Physiol Gastrointest Liver Physiol 2006;290:G199–203. 19. Andrews NC, Schmidt PJ. Iron homeostasis. Annu Rev Physiol 2007;69:69–85. 20. Jankowska EA, von Haehling S, Anker SD, Macdougall IC, Ponikowski PP. Iron deficiency and heart failure: diagnostic dilemmas and therapeutic perspectives. Eur Heart J 2013;34:816–26. 21. Ganzoni AM. Intravenous iron-dextran: thera- peutic and experimental possibilities. Schweiz Med Wochenschr 1970;100:301–3. 22. Beck-da-Silva L, Piardi D, Soder S, et al. IRON- HF study: a randomized trial to assess the effects of iron in heart failure patients with anemia. Int J Cardiol 2013;168:3439–42. 23. Anker SD, von Haehling S. Inflammatory me- diators in chronic heart failure: an overview. Heart 2004;90:464–70. 24. Danielson BG. Structure, chemistry, and pharmacokinetics of intravenous iron agents. J Am Soc Nephrol 2004;15 Suppl 2:S93–8. 25. Muckenthaler M, Richter A, Gunkel N, et al. Relationships and distinctions in iron-regulatory networks responding to interrelated signals. Blood 2003;101:3690–8. 26. Mancini DM, Katz SD, Lang CC, LaManca J, Hudaihed A, Androne AS. Effect of erythropoietin on exercise capacity in patients with moderate to severe chronic heart failure. Circulation 2003;107:294–9. 27. Anker SD, Comin Colet J, Filippatos G, et al., for the FAIR-HF Trial Investigators. Ferric carbox- ymaltose in patients with heart failure and iron deficiency. N Engl J Med 2009b;361:2436–48. 28. Ponikowski P, van Veldhuisen DJ, Comin- Colet J, et al., for the CONFIRM-HF Investigators. Beneficial effects of long-term intravenous iron therapy with ferric carboxymaltose in patients J A C C : H E A R T F A I L U R E V O L . 7 , N O . 1 , 2 0 1 9 von Haehling et al. J A N U A R Y 2 0 1 9 : 3 6 – 4 6 Iron Deficiency in Heart Failure 45
- 11. with symptomatic heart failure and iron deficiency. Eur Heart J 2015;36:657–68. 29. van Veldhuisen DJ, Ponikowski P, van der Meer P, et al., for EFFECT-HF Investigators. Effect of ferric carboxymaltose on exercise capacity in patients with chronic heart failure and iron defi- ciency. Circulation 2017;136:1374–83. 30. Jankowska EA, Tkaczyszyn M, Suchocki T, et al. Effects of intravenous iron therapy in iron- deficient patients with systolic heart failure: a meta-analysis of randomized controlled trials. Eur J Heart Fail 2016;18:786–95. 31. Anker SD, Kirwan BA, van Veldhuisen DJ, et al. Effects of ferric carboxymaltose on hospital- isations and mortality rates in iron-deficient heart failure patients: an individual patient data meta- analysis. Eur J Heart Fail 2018;20:125–33. 32. Doehner W, Blankenberg S, Erdmann E, et al. Iron deficiency in chronic heart failure: diagnostic algorithm and present-day therapeu- tic options. Dtsch Med Wochenschr 2017;142: 752–7. 33. Yancy CW, Jessup M, Bozkurt B, et al., for the American College of Cardiology Foundation/ American Heart Association Task Force on Practice Guidelines. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/ American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2013;62:e147–239. 34. Yancy CW, Jessup M, Bozkurt B, et al. 2017 ACC/AHA/HFSA Focused update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Fail- ure Society of America. J Am Coll Cardiol 2017;70: 776–803. KEY WORDS ferric carboxymaltose, heart failure, iron deficiency, treatment APPENDIX For supplemental references, please see the online version of this paper. von Haehling et al. J A C C : H E A R T F A I L U R E V O L . 7 , N O . 1 , 2 0 1 9 Iron Deficiency in Heart Failure J A N U A R Y 2 0 1 9 : 3 6 – 4 6 46