2. Diabetes mellitus-
refers to a group of common metabolic
disorders that share the phenotype of
hyperglycemia
Diagnosed by symptoms of diabetes and a two
hour plasma glucose >11.1mmol/l
(200mg/dl)and a fasting glucose>7.0mmol/l
(126mg/dl)(WHO criteria)
7. NEUROPATHY
Different metabolic pathways activated by
excess glucose- reactive oxygen
species(ROS) ie, nitric oxide, hydrogen
peroxide, advanced glycosylation end
products such as HbA1c
ROS cause damage by causing nerve
ischemia affecting protein and cell lipids and
injuring nuclear material leading to increased
apoptosis
8. Advanced glycosylation end products, by
binding cellular receptors decrease the cells
ability to detoxify itself
Nerve myelinization can be affected, along
with injury to nerve ion channel which
decrease conduction velocity
Microvascular disease also damage nerves
9. When large sensory fibres are affected protective
sensation can be lost
Small fibres afferent neuropathy can lead to
increased pain generation
Motor neuropathy can cause claw toes –
ulcerations over bony prominences
When sympathetic nervous system is affected
,skin becomes dry and scaly-cracks in skin-
invasion by bacteria
10. VASCULOPATHY
Advanced glycosylation end products can
damage vascular endothelium leading to
microthrombosis and capillary obstruction,also
increase LDL which cause atherosclerosis
Vascular tone loss due to Reactive oxygen
species(ROS)
11. IMMUNOPATHY
Defects in leucocyte response to infection
ie,problems with chemotaxis, adherence,
impaired fibroblast proliferation,
phagocytosis,and intracellular killing
Impaired growth factor
80% increased risk of cellulitis
Four fold risk of osteomyelitis
Double risk of sepsis and death from infection
12. DELAYED BONE HEALING
Collagen synthesis is decreased
Biomechanical strength of fracture callus is
lower in diabetics
Decreased cellular proliferation at fracture site
and decreased mechanical stiffness
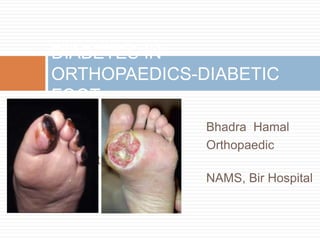
13. DIABETIC ULCER
PATHOPHYSIOLOGY
Sensory neuropathy- loss of sensation
Motor neuropathy- claw toes bony
prominences make skin vulnerable to
breakdown
Achillies contracture-(due to disorganisation
of tendon fibres and calcification within
tendon) increased forefoot pressure
forefoot ulceration
Peripheral arterial disease- ischemia
14. Wagner classification
Grade 0- skin at risk
Grade 1- superficial ulcer
Grade 2- exposed tendon and deep structures
Grade 3-deep ulcer with abscess or osteomyelitis
Grade 4-partial gangrene
Grade 5- more extensive gangrene
15.
16.
17. TREATMENT
NONOPERATIVE
TOTAL CONTACT CASTING (TCC) is the standard
of care because it reduces plantar loads better
than a well molded shoe cast
GOAL of total contact casting is the relief of
pressure by distributing stresses over a large
surface area
21. TREATMENT
Negative pressure wound treatment with vacuum
assisted closure
Hyperbaric oxygen treatment
overall healing rate 76% compared with 48% without
the use of it
Extracorporeal shockwave treatment
helpful for healing of chronic ulcer
Antibiotic treatment-if infected
deep culture obtained after debridement; superficial
swab often yield contaminants
22. TREATMENT
OPERATIVE
Indications for urgent surgical intervention
-necrotising infections
-gangrene
-deep abscess
-Incision and drainage with thorough
debridement
-Complete excision of infected bone
23. TREATMENT
Osteomyelitis of metatarsal head
-metatarsal head resection
If osteomyelitis involve more than metatarsal
head
-ray resection
Osteomyelitis of calcaneum secondary to ulcer
-partial calcanectomy
Achilles lenghtening
-to decrese plantar pressure
24. CHARCOT ARTHROPATHY
HISTORY
Prof Jean-Martin
Charcot
(1825-1893)
French Neurologist and
professor of anatomical
pathology
First described in
patient with Tabes
25. CHARCOT ARTHROPATHY
Diabetes – most common cause
Others - syphilis, syringomyelia, alcoholism,
stroke, congenital insensitivity to pain, spinal cord
or peripheral nerve injury, and spina bifida
Loss of autonomic control of the vasculature
High resting blood flow Osteopenia, combined
with somatosensory loss of pain and
proprioception multiple small mechanical
insults unrecognized by the patient which set the
stage for bony dissolution and loss of structural
integrity, followed by a collapse deformity
26.
27. Clinical Features
Foot swelling
Redness
Numbness
Pain – not a chief complaint (if present, less
than expected)
CRT – usually normal
Infected charcot’s joint – warm & red
28. Radiographs
Early neuropathic arthropathy – joint widening
and stress fractures
Progressive and late stages – further
destruction and multiple joint involvement are
seen.
Technetium bone scan is positive
29.
30. CLASSIFICATION-EICHENHOLTZ
“I CAN HOLDS”
Stage 0: No radiographic changes, marked warmth and swelling
after injury
Stage 1: Fragmentation. Erythema, warmth and swelling
of the extremity, with subluxation/dislocation of joints
and bony debris and fragmentation of subchondral
bone.
Stage 2: Coalescence. Decreased erythema, warmth and
swelling of the extremity, with absorption of fine debris,
new bone formation, and coalescence of larger
fragments.
Stage 3: Consolidation. Resolution of swelling; however,
residual deformity is present, with remodeling of bone
31. Anatomical classification-
BRODSKY
Type 1: Involvement of the
tarsometatarsal joints.
Type 2: Involvement of the Chopart
and subtalar joints.
Type 3A: involvement of the ankle
Type 3B: involvement of the calcaneus
Type 4 :involvement of multiple regions
Type 5: involvement of forefoot
32. TREATMENT
NONOPERATIVE
- Orthotics: custom-molded orthotics
that accommodate the deformity, resist
progression
-Total contact casting with protected
weight bearing
DRUGS
Bisphosphonate
-may reduce bone turnover in charcot
arthropathy and help with pain relief
Calcitonin
decrease bone turnover
33. OPERATIVE
-surgery required for approx
25% patients with charcots
arthropathy
GOAL
-Deformity correction and
stabilisation to create/maintain
a braceable, infection free foot
and ankle
34. TREATMENT
EXOSTECTOMY-remove bony prominences
causing ulceration. It should be done only if it
doesn’t lead to further instability
ARTHRODESIS-indicated for deformity
correction and for instability
AMPUTATION- last resort
35. REFERENCES
Campbell’s operative orthopaedics-12th edition
Apley’s System of Orthopaedics and Fractures- 9th
edition
Review of orthopaedics ,Miller-6th edition
Internet
Editor's Notes
type 1:This is the most common type and often leads to the rocker-bottom deformity and plantar ulcerations secondary to bony
prominences in this area. Type 2:The second most common affected area, type 2 involvement also can lead to a rocker-bottom deformity with plantar flexion of the talar head. Marked varus/valgus of the hindfoot also can develop.