Total hip replacement
•Télécharger en tant que PPSX, PDF•
230 j'aime•111,125 vues


Recommandé
Contenu connexe
Tendances
Tendances (20)
Similaire à Total hip replacement
Similaire à Total hip replacement (20)
Plus de BP KOIRALA INSTITUTE OF HELATH SCIENCS,, NEPAL
Plus de BP KOIRALA INSTITUTE OF HELATH SCIENCS,, NEPAL (20)
Dernier
Dernier (20)
Total hip replacement
- 2. Objectives Introduction History Principles and considerations Indications Contraindication Implants (its part and type) Techniques
- 3. Conti……. Nursing management Health education Exercise guide for hip replacement Complication Alternative management Prognosis
- 4. Introduction Hip replacement is also known for “Arthroplasty”. Arthroplasty is a reconstructive surgery to restore the joint motion and function and to relieve pain. It generally involves the replacement of bony joint structure by a prosthesis. It is the most common orthopaedic surgery. Hip replacement surgery can be performed:- Total replacement :- It consist of replacing both the acetabulum and the femoral head. Half (hemi) replacement :- It consist of replacing of only femoral head in general.
- 5. History Charnely (1979) revolutionized the management of the arthritic hip with the development of low-friction arthroplasty. His three major contribution to the evolution of hip replacement were:- 1. The concept of low-friction torque arthroplasty. 2. The use of acryclic cement to fix the components. 3. The introduction of high-density polyethylene as a bearing materials.
- 6. Principle & Considerations The prosthetic implant must be durable. They must permit extraordinary low-friction movement at the articulation. They must be firmly fixed to the skeleton. They must be inert and not provoke any unwanted reaction in the tissue. The prostheses are of various designs and may be fixed to the remaining bone by cement, press fit, or bone ingrowth. Selection of the prosthesis and fixation technique depends on patient’s bone structure, joint stability, and other individual characteristics, including age, weight, and activity level. Arthroplasty is an exacting and meticulous procedure. To reduce the risk of an infected prosthesis, special precautions are carried out in OT room to reduce particulate matter and bacterial count of the air.
- 7. Indications For patients with unremitting pain and irreversibly damaged joints:- Severe osteoarthritis Rheumatoid arthritis Selected fracture (femoral neck fracture). Failure of previous reconstructive surgery ( osteotomy, cup arthroplasty, femoral neck fracture complication – non union, avascular necrosis) Congenital hip diseases. Pathologic fractures from metastatic cancer. Joint instability.
- 8. Contraindication When the infection is recent or remote. When the person is under 60years of age, especially when alternative surgery is available. When pain is not severe. When manual labovers are gainfully employed.
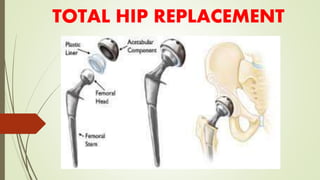
- 9. Implants The prosthetic implant used in hip replacement consist of different part. i. The acetabular cup ii. The femoral component iii. The articular interface Options exist for different patients and indications. Correct selection of the prosthesis is important.
- 10. Conti……. Type of fixation a. Cemented fixation :- cement stem use acrylic bone cement to form a mantle between the stem and the bone. b. Uncemented fixation :- uncemented stem use friction, shape and surface coating to stimulate bone to remodel and bond to the implant.
- 11. Types of implants 1. Ceramic 2. Metal-on-metal 3. Cemented, cementless or hybrid fixation of prosthesis.
- 12. Techniques There are several incisions, defined by their relation to the gluteus medius. The approaches are :- 1. Posterior (Moore) :- The posterior (Moore or Southern) approach accesses the joint and capsule through the back, taking piriformis muscle and the short external rotators off the femur. 2. Lateral (Hardinge or Liverpool) :- The lateral approach is also commonly used for hip replacement. The approach requires elevation of the hip abductors (gluteus medius andgluteus minimus) to access the joint. 3. Antero-lateral (Watson-Jones) :- The anterolateral approach develops the interval between the tensor fasciae latae and the gluteus medius. 4. Anterior (Smith-Petersen):- The anterior approach uses an interval between the sartorius muscle and tensor fascia latae.
- 13. Conti….. 5. Greater trochanter osteotomy. 6. Minimally invasive approach. There is no compelling evidence in the literature for any particular approach, but consensus of professional opinion favours either modified anterolateral (Watson-Jones) or posterior approach.
- 15. Pre-operative management Infections (bladder, dental, skin) are ruled out. Potential foci of infection for seeding prosthesis infection. Pre-operative teaching is provided. a) Post operative regimen (eg:- extended exercise program) that will be carried out after surgery is explained; atrophied muscles must be re- educated and strengthened. b) Isometric exercises of quadriceps and gluteal muscles are taught. c) Bed-to-wheel chair transfer with out going beyond the hip flexion limits (usually 60-90º) is taught. d) Non-weight and partial weight bearing ambulation with ambulatory aid (walker, crutches) is taught to facilitate post-operative ambulation. e) Abduction splint, knee immobilizer, or continuous passive motion is demonstrated if equipment will be used post-operatively.
- 16. Conti……… Anti-embolism stockings are applied to minimize development of thrombophlebitis. Skin preparation includes antimicrobial solution to reduce the skin microorganisms, a potential sources of infection. Antibiotics are administered, as prescribed, to ensure therapeutic blood level during and immediately after surgery. Cardiovascular, respiratory, renal and hepatic function are assessed and measures are taken to maximize general health conditions. Review discharge and rehabilitation options post-surgery.
- 17. Post-operative management 1.Use of appropriate position To prevent dislocation of prosthesis and facilitate healing. Numerous modifications are required in positioning the patient post-operatively. After Hip Arthroplasty a) Patient is usually positioned supine in bed. b) The affected extremity is held in slight abduction by either abduction splint or pillow or Buck’s extension traction to prevent dislocation of the prosthesis. c) Avoid acute flexion of the hip. Nurse alert:- The patient must not adduct or flex the operated hip – may lead to subluxation or dislocation of hip.
- 18. Conti…. Signs of hip dislocation Shortened extremity Increasing discomfort Inability to move
- 19. Conti……… d) Two nurse turn patient on un-operated side while supported operated hip securely in an abducted position; the entire length of leg is supported by pillows. Use of pillows to keep the leg abducted; place pillow at back for comfort. Use of overhead trapeze to assist with position change. d) The bed is not usually elevated more than 45-60º; placing the patient in an upright sitting position, put a strain on the hip joint and may cause dislocation. e) A fracture bed pan is used. Instruct patient to flex the un-operated hip and knee & pull up on the trapeze to lift buttocks onto pan. Instruct patient not to bear down on operated hip in flexion when getting off the pan.
- 20. Conti……. 2. Deterring complications Provide aggressive care and continuous assessment. Prevent thromboembolism by continuous use of elastic hose and SCD while patient is in bed. Discontinue SCD when patient is ambulatory. 3. Promoting early ambulation i. Within 1 day after surgery, short period of standing may be ordered. Monitor orthostatic hypotension. Weight bearing may be limited with ingrowth prosthesis to prevent disruption of bone growth. ii. Transfer to the chair or ambulation with aids, such as walkers, are encouraged as tolerated and based on patient’s condition and type of surgery.
- 21. Health Education 1. Encourage patient to continue to wear elastic stockings after discharge until full activities are resumed. 2. Ensure that patient avoid excessive hip adduction, flexion and rotation for 6 weeks after hip arthroplasty. Avoid sitting low chair or toilet seat to avoid flexing hip > 90º. Keep knees apart :- do not cross leg. Limit sitting to 30 minutes at a time – to minimize hip flexion and the risk of prosthetic dislocation and to prevent hip stiffness & flexion contractures. Avoid internal rotation of the hip. Follow weight-bearing restrictions from surgeon.
- 22. Conti……….. 3. Encourage quadriceps setting and range of motion exercise as directed. Have a daily program of stretching, exercise and rest throughout life time. Do not participate in any activity placing undue or sudden stress on joint.(jogging, jumping, lifting, excessive bending) Use a cane when taking fairly long steps. 4. Suggest self-help and energy-saving devices. 5. Advise patient to sleep with 2 pillows between the legs to prevent turning over in sleep.
- 23. Conti……. 6. Tell patient to lie prone when able twice daily for 30 minutes to promote full extension of hip. 7. Monitor for late complications:- deep infection, increased pain or decreased function, implant wear, dislocation, Avascular necrosis. 8. Teach patient use of supportive equipment (crutches, canes) as prescribed. 9. Avoid MRI studies because of implanted metal components. 10. Advice patient that metal components in hip may set off metal detectors (airports, some buildings). They should carry a medical identification card.
- 24. Exercise guide for hip replacement Regular exercises to restore your normal hip motion and strength and a gradual return to everyday activities are important for your full recovery. Orthopaedic surgeon and physical therapist may recommend an exercise for 20 to 30 minutes, 2 or 3 times a day during your early recovery. They may suggest some of the following exercises:- 1. Ankle Pumps Slowly push your foot up and down. Do this exercise several times as often as every 5 or 10 minutes. This exercise can begin immediately after surgery and continue until you are fully recovered.
- 25. Conti……. 2. Ankle rotation Move your ankle inward toward your other foot and then outward away from your other foot. Repeat 5 times in each direction, 3 or 4 times a day. 3. Bed-Supported Knee Bends Slide your heel toward your buttocks, bending your knee and keeping your heel on the bed. Do not let your knee roll inward. Repeat 10 times, 3 or 4 times a day
- 26. Conti……. 4. Buttock Contractions Tighten buttock muscles and hold to a count of 5. Repeat 10 times 3 or 4 times a day 5. Abduction Exercise Slide your leg out to the side as far as you can and then back. Repeat 10 times 3 or 4 times a day 6. Quadriceps Set Tighten your thigh muscle. Try to straighten your knee. Hold for 5 to 10 seconds. Repeat this exercise 10 times during a 10-minute period. Continue until your thigh feels fatigued.
- 27. Conti….. 7. Straight Leg Raises Tighten your thigh muscle with your knee fully straightened on the bed. As your thigh muscle tightens, lift your leg several inches off the bed. Hold for 5 to 10 seconds. Slowly lower. Repeat until your thigh feels fatigued 8. Standing Knee Raises Lift your operated leg toward your chest. Do not lift your knee higher than your waist. Hold for 2 or 3 counts and put your leg down. Repeat 10 times 3 or 4 times a day
- 28. Conti…… 9. Standing Hip Abduction Be sure your hip, knee and foot are pointing straight forward. Keep your body straight. With your knee straight, lift your leg out to the side. Slowly lower your leg so your foot is back on the floor. Repeat 10 times 3 or 4 times a day 10. Standing Hip Extensions Lift your operated leg backward slowly. Try to keep your back straight. Hold for 2 or 3 counts. Return your foot to the floor. Repeat 10 times 3 or 4 times a day
- 29. Conti……. 11. Walking and Early Activity. 12. Walking with Walker, Full Weight-bearing. 13. Walking with Cane or Crutch. 14. Stair Climbing and Descending.
- 30. Complications Vein thrombosis Pulmonary embolism Dislocation Osteolytis Metal sensitivity Metal toxicity Nerve palsy Chronic pain Leg length inequality Death
- 31. Alternative management 1. Conservative management The first line approach as an alternative to hip replacement is conservative management which involves a multimodal approach of medication, activity modification and physical therapy. Conservative management can prevent or delay the need for hip replacement. 2. Hemiarthroplasty Hemiarthroplasty is a surgical procedure which replaces one half of the joint with an artificial surface and leaves the other part in its natural (pre- operative) state. This class of procedure is most commonly performed on the hip after a subcapital (just below the head) fracture of the neck of the femur (a hip fracture).
- 32. Conti…… The procedure is performed by removing the head of the femur and replacing it with a metal or composite prosthesis. 3. Hip resurfacing Hip resurfacing is an alternative to hip replacement surgery. It has been used in Europe for over 17 years and become a common procedure. The minimally invasive hip resurfacing procedure is a further refinement to hip resurfacing. 4. Viscosupplementation Current alternatives also include viscosupplementation, or the injection of artificial lubricants into the joint.[29] Use of these medications in the hip is off label.
- 33. Prognosis Hip replacement surgery results are often excellent. Most or all of your pain and stiffness should go away. Some people may have problems with infection, loosening, or even dislocation of the new hip joint. Over time the artificial hip joint will loosen. This can happen after as long as 15 - 20 years. You may need a second replacement. Younger, more active people may wear out parts of their new hip. It may need to be replaced before the artificial hip loosens.
- 34. References 1. Louis Solomon, David Warwick, Selvadural Nayagam, “Apley’s system of orthopaedics and fractures”, 9th edition, pg no:- 534-43. 2. Wiesel Dilahay Connel, “Essentials of orthopaedic surgery”,1st edition, pg no:-237-50. 3. Samuel L Turek, “Orthopaedic – principles & their applications”, 4th edition, volume-2, pg no:- 1198-1204. 4. William and Wilkins, “Lippincott Manual of nursing practices”, 9th edition, pg no:-1116-1119. 5. Brunner & Suddarth’s, “Textbook of Medical-Surgical Nursing”, 12th edition, volume-2, pg no :-2036-2044.
- 35. Thank You PREPARED BY:- Sunita –Rai, Bsc. Nursing 2nd year