Chest Physiotherapy
•Download as PPTX, PDF•
10 likes•7,190 views

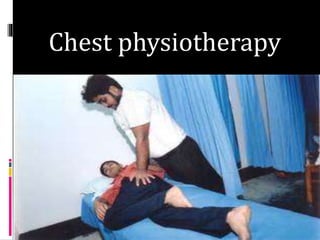
The document discusses chest physiotherapy techniques which are used to mobilize secretions in the lungs through external maneuvers like percussion, postural drainage, and vibration. It explains the indications for chest physiotherapy in patients with excessive secretions or ineffective cough from conditions like cystic fibrosis or pneumonia. The techniques involve positioning patients and using cupped hands to clap or vibrate the chest wall to loosen mucus so it can be coughed up.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Chest Physiotherapy
Similar to Chest Physiotherapy (20)
More from Prof.Dr.Shali.B.S.Mamata College of Nursing,Khammam,Telangana.
More from Prof.Dr.Shali.B.S.Mamata College of Nursing,Khammam,Telangana. (20)
Recently uploaded
Recently uploaded (20)
Chest Physiotherapy
- 3. DEFINITION Chest physiotherapy (CPT) is a technique used to mobilize or loose secretions in the lungs and respiratory tract. This is especially helpful for patients with large amount of secretions or ineffective cough.
- 4. Chest physiotherapy consists of external mechanical maneuvers, such as chest percussion, postural drainage, vibration, to augment mobilization and clearance of airway secretions, diaphragmatic breathing with pursed-lips, coughing and controlled coughing.
- 5. Physiology of Respiration INHALATION Inhalation is initiated by the diaphragm and supported by the external intercostal muscles. Normal resting respirations are 10 to 18 breaths per minute. Its time period is 2 seconds. Inhalation is primarily driven by the diaphragm and accessory muscles. When the diaphragm contracts, the ribcage expands and the contents of the abdomen are moved downward. This results in a larger thoracic volume, which in turn causes a decrease in intrathoracic pressure. As the pressure in the chest falls, air moves into the conducting zone. Here, the air is filtered, warmed, and humidified as it flows to the lungs
- 6. EXHALATION Exhalation is generally a passive process, however active or forced exhalation is achieved by the abdominal and the internal intercostal muscles. The lungs have a natural elasticity; as they recoil from the stretch of inhalation, air flows back out until the pressures in the chest and the atmosphere reach equilibrium. During forced exhalation, as when blowing out a candle, expiratory muscles including the abdominal muscles and internal intercostal muscles, generate abdominal and thoracic pressure, which forces air out of the lungs.
- 7. GAS EXCHANGE The major function of the respiratory system is gas exchange. Upon inhalation, gas exchange occurs at the alveoli, the tiny sacs which are the basic functional component of the lungs. The alveolar walls are extremely thin, and are permeable to gases. The alveoli are lined with pulmonary capillaries, the walls of which are also thin enough to permit gas exchange.
- 8. All gases diffuse from the alveolar air to the blood in the pulmonary capillaries, as carbon dioxide diffuses in the opposite direction, from capillary blood to alveolar air. Now, the pulmonary blood is oxygen-rich, and the lungs are holding carbon dioxide. Exhalation follows, thereby ridding the body of the carbon dioxide and completing the cycle of respiration. In an average resting adult, the lungs take up about 250ml of oxygen every minute while excreting about 200ml of carbon dioxide. During an average breath, an adult will exchange from 500 ml to 700 ml of air. This, average breath capacity is called tidal volume.
- 9. Indications of Chest Physiotherapy It is indicated for patients in whom cough is insufficient to clear thick, tenacious, or localized secretions. Examples include: Cystic fibrosis Bronchiectasis Atelectasis Lung abscess Neuromuscular diseases Pneumonias in dependent lung regions.
- 10. Contraindications of Chest Physiotherapy Increased ICP Unstable head or neck injury Active hemorrhage with hemodynamic instability or hemoptysis Recent spinal injury or injury Empyma Bronchoplueral fistula Rib fracture Fail chest Uncontrolled hypertension Anticoagulation Rib or vertebral fractures or osteoporosis.
- 11. ASSESSMENT FOR CHEST PHYSIOTHERAPY Nursing care and selection of CPT skills are based on specific assessment findings.
- 12. The following are the assessment criteria: Know the normal range of patient’s vital signs. Conditions requiring CPT, such atelectasis, and pneumonia, affects vital signs. Know the patient’s medications. particularly diuretics antihypertensive cause fluid and hemodynamic changes. These decrease patient’s tolerance to positional changes and postural drainage.
- 13. Know the patient’s medical history; certain conditions such as increased ICP, spinal cord injuries and abdominal aneurysm resection, contra indicate the positional change to postural drainage. Thoracic trauma and chest surgeries also contraindicate percussion and vibration.
- 14. Know the patient’s cognitive level of functioning. Participating in controlled cough techniques requires the patient to follow instructions. Beware of patient’s exercise tolerance. CPT maneuvers are fatiguing. Gradual increase in activity and through CPT, patient tolerance to the procedure improves.
- 15. Clinicalfindingsandinvestigations Detailed History Physical examination Inspection Palpation Percussion Auscultation Investigations X-ray Blood investigations-bleeding and clotting parameters
- 16. TECHNIQUESIN CHEST PHYSIOTHERAPY: A nurse or respiratory therapist may administer CPT, although the techniques can often be taught to family members of patients. The most common procedures used are postural drainage and chest percussion, in which the patient is rotated to facilitate drainage of secretions from a specific lobe or segment while being clapped with cupped hands to loosen and mobilize retained secretions that can then be expectorated or drained. The procedure is somewhat uncomfortable and tiring for the patient.
- 17. PERCUSSION Chest percussion involves striking the chest wall over the area being drained. Percussing lung areas involves the use of cupped palm to loosen pulmonary secretions so that hey can be expectorated with ease. Percussing with the hand held in a rigid dome-shaped position, the area over the lung lobes to be drained in struck in rhythmic pattern. Usually the patient will be positioned in supine or prone and should not experience any pain.
- 18. Cupping is never done on bare skin or performed over surgical incisions, below the ribs, or over the spine or breasts because of the danger tissue damage. Typically, each area is percussed for 30 to 6oseconds several times a day. If the patient has tenacious secretions, the area must be percussed for 3-5 minutes several times per day. Patients may learn how to percuss the anterior chest as well.
- 19. 2. Vibration In vibration, the nurse uses rhythmic contractions and relaxations is or her arm and shoulder muscles while holding thee patient flat on the patient’s chest as the patient exhales. The purpose is to help loosen respiratory secretions so that they can be expectorated with ease. Vibration (at a rate of 200 per minute) can be done for several times a day.
- 20. To avoid patient causing discomfort, vibration is never done over the patient’s breasts, spine, sternum, and rib cage. Vibration can also be taught to family members or accomplished with mechanical device.
- 23. PROCEDURE: Percussion & Vibration Instruct the patient use diaphragmatic breathing Position the patient in prescribed postural drainage positions. Spine should be straight to promote rib cage expansion Percuss or clap with cupped hands or chest wall for 5 minutes over each segment for 5 minutes for cystic fibrosis and 1-2 minutes for other conditions Avoid clapping over spine, liver, spleen, breast, scapula, clavicle or sternum Instruct the patient to inhale slowly and deeply. Vibrate the chest wall as the patient exhales slowly through the pursed lips.
- 24. Place one hand on top of the other affected over area or place one hand place one and on each side of the rib cage. Tense the muscles of the hands and hands while applying moderate pressure downward and vibrate arms and hands Relieve pressure on the thorax as the patient inhales. Encourage the patient cough, using abdominal muscles, after three or four vibrations.
- 25. Allow the patient rest several times Listen with stethoscope for changes in breath sounds Repeat the percussion and vibration cycle according to the patient’s tolerance and clinical response: usually 15-30 minutes.