Malignant melanoma
•Download as PPTX, PDF•
21 likes•6,854 views

Please find the power point (ppt.) on everything that you need to know about Malignant melanoma in very simple language by Sunil kumar Daha from very reliable references. Especially focused on surgical interventions. Thank you

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Malignant melanoma
Similar to Malignant melanoma (20)
More from sunil kumar daha
More from sunil kumar daha (20)
Recently uploaded
Recently uploaded (20)
Malignant melanoma
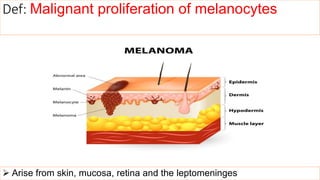
- 1. Arise from skin, mucosa, retina and the leptomeninges Def: Malignant proliferation of melanocytes
- 2. Epidemiology App. 5% of skin malignancy ( 75 per cent of skin malignancy related deaths), MM accounts for 3% of all malignancy worldwide, Most common cancer in young adults (20–39 years), 5% of all patients with MM will develop a second primary melanoma, 7% MMs present as occult metastases from an unknown primary Increasing incidence over the years and equal in both sexes
- 3. Risk factors: Hx of exposure to sunlight: Intense intermittent exposure Significant adult exposure ( associated with sunburn below 10) Geographical location (Australia and New Zealand) Skin Factors: Xeroderma pigmentosum (RR= 1000) Past medical or family history of MM with dysplastic naevi Previous melanoma (RR= 84) Multiple benign or atypical naevi Dysplastic naevi (10% lifetime risk) Red hair (RR= 3) Tendency to freckle Immunosuppression Giant congenital pigmented naevus Albinism Genetic predisposition (CDKN2A gene)
- 4. Pathophysiology UV exposure is the major causal factor for developing MM Cumulative exposure favours the development of lentigo maligna melanoma (LMM), Whereas ‘flash fry’ exposure, typical of rapidly acquired holiday tans – favours the other morphological variants
- 5. Diagnosis History • Change in size, shape and color • Redness • Itchy • Tender • Bleeding • Crusting • Ulceration Examination: • ABCDEs criteria • Glasgow 7 point Criteria
- 6. ABCDEs Criteria A- Asymmetry B- Border irregularity/bleeding C- Color Variation D- Diameter (>6mm) E- Elevation
- 7. Glasgow 7 point Criteria • Major Features: 1. Change in size 2. Irregular shape 3. Irregular color • Minor features: 1. Inflammation 2. Oozing 3. Change in sensation
- 8. Microscopic finding: Nevus • nevus cells are arranged in nests. • nuclei of nevus cells are uniform and rounded in contour and contain inconspicuous nucleoli. • the cells contain melanin pigment. • little or no mitotic activity.
- 9. Microscopy: Melanoma • melanoma cells are pleomorphic and have hyperchromatic nuclei with prominent nucleoli. • melanin pigment is present as fine granules. • frequent mitosis.
- 10. 4 common variants of MM 1. Superficial spreading melanoma 2. Nodular melanoma 3. Lentigo maligna melanoma 4. Acral lentiginous melanoma
- 11. 1. Superficial spreading melanoma • Most common type (70%) • Most likely to arise in a pre-existing naevus, after several years of slow change • Followed by rapid growth in the preceding months before presentation • Typically it is a darker pigmented area in a junctional naevus • Nodularity within superficial spreading melanoma heralds the onset of the vertical growth phase
- 13. 2. Nodular melanoma • Accounts 15% of all MMs • male > female, arise typically de novo in skin • More aggressive • Shorter clinical onset • Presenting in middle age and usually on the trunk, head or neck • Appear as blue/black papules, 1–2 cm in diameter • They lack the horizontal growth phase, tend to be sharply demarcated
- 15. 3. Lentigo maligna melanoma • Previously k/a Hutchison’s melanotic freckle • Slow growing, varigated brown macule (a lentigo), on face, neck or hands of the elderly • Positively correlated with prolonged, intense sun exposure • Women > men (5-10%) • In situ melanoma in this variant is called lentigo maligna • Less metastatic potential than other variants as they take longer to enter a vertical growth phase
- 17. 4. Acral lentiginous melanoma • Affects the soles of feet and palms of hands • Rare in white-skinned individuals • More common in the Afro-Caribbean, Hispanic and Asian populations (35–60%) • Usually presents as a flat, irregular macule in later life • Twenty-five per cent are amelanotic may mimic a fungal infection or pyogenic granuloma • MM under the finger nail is usually SSM rather than ALM
- 18. • For finger or toe nail lesions, vital to biopsy the nail matrix rather than just the pigment on the nail plate • Feature of subungual melanoma- Hutchinson’s sign positive (nail fold pigmentation which then widens progressively to produce a triangular pigmented macule with associated nail dystrophy) • The differential diagnosis is ‘benign racial melanonychia’, which produces a linear dark streak under a nail in a dark-skinned individual
- 19. Fig: Acral lentiginous melanoma on the sole of the footFig: Subungual melanoma – superficial spreading melanoma. Fig: Benign racial melanonychia
- 20. Miscellaneous Types • Amelanotic melanoma (often arising in the GI tract and presenting with obstruction, intussusception or as a metastasis from an unknown primary) • Desmoplastic – mostly found on the head and neck region, has a propensity for perineural infiltration and often recurs locally if not widely excised. May be amelanotic clinically
- 21. Investigations • Guidelines for staging are controversial • Offering sentinel node biopsy to patients with clinical stage II disease is prudent • Investigations for stage III disease should be directed to individual clinical presentation
- 23. Management • focuses on: Prolonging survival Eliminating the cancer Shrinking or stopping the growth of known metastases Controlling symptomatic or risky sites of disease Providing comfort “Depending upon where and how big the metastases are, treatment may involve drug treatments, surgery, and/or radiation therapy”
- 24. For Primary: Surgery is the main treatment 1. Handley’s wide local excision (WLE): wide excision with clearance of margin as well as depth. 2. If primary area is wide, then amputation with one joint above is done. 3. In fingers and toes, disarticulation is required.
- 25. Regional lymph nodes For biopsy positive nodal disease : block dissection of the regional lymph nodes to remove all the lymph nodes in that regional basin
- 26. Drug treatments 3 main categories : 1. Immunotherapy – Drugs that stimulate or unleash your immune system to attack and kill the cancer cells 2. Targeted therapy – Drugs that inhibit specific enzymes or molecules important to the cancer cells 3. Chemotherapy – Drugs that stop or slow the growth of cancer cells by interfering with their ability to divide or reproduce themselves
- 27. Immunotherapy • (nivolumab [Opdivo], pembrolizumab [Keytruda], ipilimumab [Yervoy]), which have largely replaced high-dose interleukin-2 (IL-2). These have important benefits for some patients, although each can cause significant side effects. • Anti-PD-1 checkpoint inhibitors — The anti-PD-1 checkpoint inhibitors (nivolumab, pembrolizumab) unleash the body’s immune system so that it can be able reject the melanoma. Nivolumab is given once every two weeks, while pembrolizumab is given once every three weeks.
- 28. Targeted therapy • Three drugs, vemurafenib (Zelboraf), dabrafenib (Taflinar), and trametinib (Mekinist) block this protein or the pathway it stimulates and cause tumors with this specific mutation in BRAF to shrink. • Generally, dabrafenib is given in combination with trametinib, as the two agents together have been shown to be more effective and no more toxic than single- agent dabrafenib or vemurafenib.
- 29. Chemotherapy • dacarbazine or temozolomide to stop or slow the growth of cancer cells by interfering with the ability of cancer cells to divide or reproduce. • S/E on highly growing cells. Chemotherapy is less effective than immunotherapy or targeted therapy, and it generally is not used as the initial treatment for patients with advanced disease.
- 30. Prognosis Very aggressive tumor The higher the mitotic index, the poorer the prognosis of the primary tumor. Once regional nodes are involved clinically, 70–85% of patients will have occult distant metastases. Ageing, Females and Extremities melanoma better prognosis
- 31. References • Bailey and Love’s Short Practice of Surgery; 26th Edition • SRB’s manual of surgery; 5th edition • Robbin’s Basis of pathology; 9th edition
- 32. Summary • Definition • Epidemiology • Risk factors • Diagnosis • Types of melanoma • Investigations • Management • Prognosis The end
Editor's Notes
- Melanocytes: The melanin pigment producing cells of skin, located in stratum Basale Melanoma leads to pigmentation of the skin - Melanoma is the sixth most common cancer in the United States, and the number of melanoma cases diagnosed annually is increasing faster than for any other cancer.
- Cutaneous melanoma is caused largely by exposure to ultraviolet radiation Its rise in incidence reflects social behaviour and increased recreational activity in the sun among white-skinned races not suited to sun exposure
- - Only 10–20 per cent of MM form in pre existing naevi, with the remainder arising de novo in previously normally pigmented skin The most likely naevi to form MM are the junctional and compound types
- flash-fry verb fry (food) briefly and at a very high temperature.
- Tingling/itching/serosanguinous discharge (usually late signs) Blood supply: melanomas >1 mm thick have blood supply, ‘Doppler positive’, pigmented lesions should be excised Serosanguineous means containing or relating to both blood and the liquid part of blood (serum). It usually refers to fluids collected from or leaving the body. For example, fluid exiting a wound that is serosanguineous is yellowish with small amounts of blood.
- Melanocytic NEVus: brown uniformly pigmented small (usually <6 mm) well-defined, rounded borders
- Malignant change occurs in the melanocytes in the basal epidermis In situ, atypical melanocytes are limited to the dermoepidermal junction, show no evidence of dermal involvement During the horizontal growth phase, cells spread along the dermo-epidermal junction, Although they may breach the dermis, Migration is predominantly radial During the vertical growth phase, the dermis may be invaded The greater the depth of invasion, the greater is the metastatic potential of the tumour.
- Hutchinson’s sign. This is nail fold pigmentation which then widens progressively to produce a triangular pigmented macule with associated nail dystrophy. variegated ˈvɛːrɪɡeɪtɪd,ˈvɛːrɪə-/ adjective exhibiting different colours, especially as irregular patches or streaks. In situ melanoma is the very earliest stage of melanoma. There are cancer cells in the top layer of skin (the epidermis) but they are all contained in the area in which they started to develop. So they have not started to spread or grow into deeper layers of the skin.
- Hutchinson’s sign. This is nail fold pigmentation which then widens progressively to produce a triangular pigmented macule with associated nail dystrophy.
- 1. a melanoma beginning in the skin at the border of or beneath the nail, usually of acral lentiginous type (q.v.). The definition information forsubungual melanoma is provided by Stedman's.
- The sentinel lymph node is the hypothetical first lymph node or group of nodes draining a cancer. In case of established cancerous dissemination it is postulated that the sentinel lymph node/s is/are the target organs primarily reached by metastasizing cancer cells from the tumor. - After melanoma is diagnosed, the next step is to determine the cancer's stage, which is based upon the thickness of the tumor, the extent of its spread, and its aggressiveness. Staging is important to determine the most appropriate treatment. Melanoma generally starts as a single tumor or lesion. Cancer cells can then spread to nearby lymph nodes and/or distant sites throughout the body. Once melanoma spreads to distant locations, it is called advanced or metastatic.
- Evidence says that more than 2 cm clearance will not show any additional advantage in treating primary tumour. Primary closure or SSG or local fl aps are used to cover the defect. - Procedure can be done under regional or local anaesthesia. 4. Melanoma in anal canal may require abdominoperineal resection. 5. Enucleation in case of melanoma in eye. 6. Melanoma in pregnancy is treated with termination of pregnancy and specifi c therapy for melanoma. Pregnancy should be postponed for 2 years.
- Surgery — Surgery may be recommended if melanoma has spread to one or a very limited number of sites. Surgery may prolong survival or relieve symptoms caused by the melanoma. However, surgery is rarely curative because metastatic melanoma usually spreads to many different places throughout the body. Surgery can also help to relieve pain caused by a metastatic tumor, such as in the lung or brain.
- Advances in the use of immunotherapy and targeted therapy improve survival for most patients and now are the preferred approaches for patients with metastatic melanoma. Although chemotherapy was widely used in the past, it now has a limited role for patients whose disease can no longer be controlled with either immunotherapy or targeted therapy. Both are continued unless there is evidence of disease progression or severe side effects. Nivolumab may be given in combination with ipilimumab. Treatment with nivolumab, pembrolizumab, or the combination of nivolumab plus ipilimumab may decrease the extent of your melanoma and help you live longer. Both nivolumab and pembrolizumab can cause the body to develop an immune reaction against its own tissues. This can result in a wide range of side effects that occasionally (<5 percent of all treated patients) can be severe or life-threatening. The most important of these side effects include lung inflammation (causing difficulty breathing), rash or inflammation of the skin, hepatitis, inflammation of the kidneys causing decreased kidney function, colitis (causing diarrhea or bleeding), and inflammation of endocrine organs (pituitary, thyroid, or adrenal, leading to diminished hormone production). If one takes one of these drugs, it is important to tell your doctor about any side effects they experience, even mild ones. This will help to avoid more serious complications. Ipilimumab — Ipilimumab is a drug that stimulates the body’s immune system to react against the melanoma. Ipilimumab is given once every three weeks for a total of four doses. Although treatment with ipilimumab may decrease the extent of your melanoma and help you live longer, it is less effective than nivolumab or pembrolizumab, and is used primarily in combination with nivolumab. Ipilimumab can also cause the body to develop an immune reaction against its own tissues. Principal immune-related toxicities from ipilimumab include colitis, rash, hepatitis, and inflammation of the endocrine organs, each occurring in 5 to 30 percent of patients. These ipilimumab-related side effects tend to be both more frequent and more severe than those seen with the anti-PD-1 pathway checkpoint inhibitors. Interleukin-2 (IL-2) — IL-2 is a form of immunotherapy that was found to help some people with metastatic melanoma when given in high doses. In some people treated with high-dose IL-2, the disease disappeared completely or stopped growing for a prolonged period. Treatment usually required being in the hospital. IL-2 has largely been replaced by checkpoint inhibitors, which are safer and more effective. These drugs thus prolong the time until there is disease growth and extend overall survival in patients with BRAF-mutant melanoma. However, tumors eventually start to grow again despite continuation of treatment with this targeted therapy. The most significant side effects with vemurafenib are development of other kinds of skin cancers (non-melanoma), which can be managed with routine skin cancer care and do not require interruption of treatment; skin photosensitivity; joint pain; and fatigue. The most significant side effects for dabrafenib and trametinib combination are fevers, rash, fatigue, and liver test abnormalities.
- - About one-half of metastatic melanomas contain a specific mutation in one gene (BRAF) that causes the cell to make a particular protein that drives the growth of cancer cells. The melanoma actually becomes addicted to the actions of this protein (oncogene addiction).