Call Girls Jaipur Just Call 9521753030 Top Class Call Girl Service Available
Cardiomyopathy - lecture.ppt
1. Chala.F, MD, consultant internist and cardiologist
Assistant professor
AAU, CHS, SoM, cardiology unit
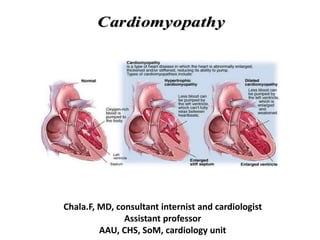
Cardiomyopathy
Cardiomyopathy
2. Definition of cardiomyopathy
• Cardiomyopathies:
Are group of diseases that primarily affect the heart muscle
and are not the result of congenital, acquired valvular,
hypertensive, coronary arterial, or pericardial abnormalities
2
3. Classification of Cardiomyopathies
• Two fundamental forms:
primary type: predominantly involving the myocardium
and/or of unknown cause
secondary type: myocardial disease of known cause or
associated with a systemic disease such as amyloidosis or
chronic alcohol use.
3
Etiology and classification
5. • In many cases it is not possible to arrive at a specific etiologic
diagnosis, and thus it is often more desirable to classify the
cardiomyopathies into one of three morphologic types:
o Dilated,
o Restrictive, and
o Hypertrophic
On the basis of differences in their pathophysiology and
clinical presentation
5
Etiology and classification
6. • Dilated CMP:
Left and/or right ventricular enlargement,
impaired systolic function,
• Restrictive CMP:
Endomyocardial fibrosis/scarring or myocardial infiltration resulting in
restriction to left and/or right ventricular filling
• Hypertrophic CMP:
Disproportionate left ventricular hypertrophy, typically involving septum
more than free wall, with or without an intraventricular systolic pressure
gradient; usually of a nondilated left ventricular cavity
Clinical Classification of Cardiomyopathies
6
8. Dilated Cardiomyopathy
• Most common
• LV and/or RV systolic pump function
is impaired, leading to progressive
cardiac dilatation
Symptoms of heart failure
typically appear only after
remodeling has been ongoing for
some time (months/yrs)
• may occur at any age, but most
commonly becomes apparent
clinically in the 3rd or 4th decades
8
10. • Familial/ Genetic
– 30% of ‘idiopathic’
– Inheritance patterns
• Autosommal dominant /recessive , x-linked, mitochondrial
– Associated phenotypes:
• Skeletal muscle abnormality, neurologic, auditory
– Mechanism:
• Abnormalities in:
– Energy production
– Contractile force generation
• Specific genes coding for:
– Myosin, actin, dystophin…
Dilated Cardiomyopathy
11. Reversible forms of DCM may be found with:
• Alcohol abuse,
• Pregnancy,
• Thyroid disease,
• Cocaine use, and
• Chronic uncontrolled tachycardia
11
Dilated Cardiomyopathy
13. Clinical Features
• Symptoms HF usually develop gradually
• vague chest pain may be present, typical angina pectoris is
unusual and suggests the presence of IHD
• Syncope due to arrhythmias and systemic embolism may occur
• Physical Examination:
Variable degrees of cardiac enlargement
In patients with advanced disease, the pulse pressure is
narrow and the jugular venous pressure is elevated
Third and fourth heart sounds are common, and mitral or
tricuspid regurgitation may occur
13
14. Laboratory Examinations
• CXR:
enlargement of the cardiac silhouette or generalized cardiomegaly
pulmonary vascular redistribution and interstitial or, alveolar edema
• ECG:
sinus tachycardia or atrial fibrillation, low voltage, diffuse nonspecific ST-T-
wave abnormalities, and sometimes intraventricular and/or AV conduction
defects
• Circulating levels of BNP are usually elevated
• Echocardiography, Cardiac MRI, CT
show LV dilatation, with normal, minimally thickened, or thinned walls, and
systolic dysfunction
14
16. Prognosis and treatment
• Patients of African ancestry are more likely to suffer rapidly
progressive HF and death than Caucasians
– Death is due to either progressive HF or ventricular tachy- or
bradyarrhythmia
• Standard therapy of HF
• Cardiac resynchronization therapy and insertion of an
implantable cardioverter defibrillator (ICD)…if indicated
16
17. Alcoholic Cardiomyopathy
• Individuals who consume large quantities (>90 g/d) of alcohol over
many years
• The risk of developing cardiomyopathy is partially determined
genetically
A polymorphism of the gene encoding the alcohol metabolizing enzyme,
alcohol dehydrogenase (ALDH2*2), as well as angiotensin-converting
enzyme (ACE) gene increase the risk
• Patients with advanced alcoholic cardiomyopathy and severe HF
have a poor prognosis
• Management consists of abstention, which may halt the progression
or even reverse the course of this disease 17
18. • Holiday Heart syndrome:
Typically appears after a drinking binge
May be found in individuals without overt HF and consists of
recurrent supraventricular or ventricular tachyarrhythmias
Atrial fibrillation is seen most frequently, followed by atrial
flutter and frequent PVCs
18
Alcoholic Cardiomyopathy
19. Peripartum Cardiomyopathy
• Occurs during the last trimester of pregnancy till 6th month post
partum
• cause is unknown
– incriminated factors : inflammatory myocarditis, immune activation, and
gestational hypertension
• Typically occurs in :
Multiparous,
Twin pregnancy
African ancestry
Age >30 years
malnutrition
Use of tocolytics , preeclampsia or toxemia of pregnancy
• The mortality rate of this disorder is around 10% 19
20. • The prognosis is related to whether the heart size returns to
normal after the first episode of HF
– If it does, subsequent pregnancies may be tolerated
– if the heart remains enlarged, and/or the LV ejection fraction
(EF) remains depressed after 6 months,
prognosis is poor, and further pregnancies frequently
produce additional myocardial damage
• Patients who recover from peripartum cardiomyopathy should be
encouraged to avoid further pregnancies, particularly if LV
dysfunction persists
20
Peripartum Cardiomyopathy
21. Anthracycline CMP
• anthracycline derivatives (EX- doxorubicin)… usual culprits
• Systolic dysfunction and ventricular arrhythmias occur in a dose-
dependent manner (doses >550 mg/m2 )
appears to be related to damage to the inner mitochondrial
membrane and interference with the synthesis of ATP
• Occurrence depends on the presence or absence of several risk
factors, which include cardiac irradiation, underlying heart
disease, hypertension, and concurrent treatment with
cyclophosphamide
21
22. Prognosis depends on Etiology
1230 pts. referred for unexplained CM. Felker GM. NEJM 2000;342:1077
23. Hypertrophic Cardiomyopathy
• Characterized by LV hypertrophy, typically of a non-dilated chamber,
without obvious cause, such as hypertension or aortic stenosis
• Two features of HCM:
asymmetric LV hypertrophy, often with preferential hypertrophy
of the interventricular septum; and
a dynamic LV outflow tract pressure gradient, related to
narrowing of the subaortic area
• diastolic dysfunction results in elevated LVEDP
23
24. • Incidence : 1:500 adult population
• Etiology:
– About half of pts have a positive
family history
– Familial in ~ 55% of cases with
autosomal dominant transmission
– Mutations in one of 4 genes
encoding proteins of cardiac
sarcomere account for majority of
familial cases (60-70% )
– Most common mutations occur in
beta myosin heavy chain
Hypertrophic Cardiomyopathy
25. • Patterns of hypertrophy:
– Diffuse hypertrophy of the ventricular septum and
anterolateral free wall (70% to 75%)
– Basal septal hypertrophy (10% to 15%)
– Concentric hypertrophy (5%)
– Apical hypertrophy (<5%)
– Hypertrophy of the lateral wall (1% to 2%).
25
Hypertrophic Cardiomyopathy
28. Clinical Features
• Phenotypic expression usually occurs in childhood or early
adolescence
Most are asymptomatic or mildly symptomatic
Symptoms include chest pain, SOB, palpitations, and Syncope
• most common complaint is dyspnea
Unfortunately, the first clinical manifestation may be SCD
• More young people die of SCD
• 5-10% will progress to develop systolic HF ( burned out)
• Mortality is 1-2% /year and attributed to SCD, HF and stroke
28
29. Physical Examination
• double or triple apical precordial impulse and a fourth
heart sound
• a systolic murmur, which is typically harsh, diamond-
shaped, and usually begins well after the first heart
sound
• The murmur is best heard at the lower left sternal
border as well as at the apex
29
30. • HCM is characterized by wide array of hemodynamic abnormalities
– Dynamic LV outflow tract obstruction
• Outflow tract gradient (>30 mm Hg), considered severe if >50 mm Hg
(occurs in 25-30% of cases leading to name hypertrophic obstructive
cardiomyopathy)
• Obstruction appears to result from narrowing of the LV outflow tract by
systolic anterior movement (SAM) of the mitral valve against the
hypertrophied septum
– Diastolic dysfunction
• Impaired diastolic filling, filling pressure
– Myocardial ischemia
– Mitral regurgitation
30
Hemodynamic abnormalities
31. Laboratory Evaluation
31
ECG
• Abnormal - >90% of pts & >75% of asymptomatic relatives
– Increased voltages consistent with LV hypertrophy
– ST-T changes - marked T wave inversion in the lateral precordial leads
– Left atrial enlargement
– Deep and narrow Q waves
– Diminished R waves in the lateral precordial leads.
• Normal ECG - 5% of pts
– Less severe phenotype and favorable course
– Not predictive of future sudden death
• Increased voltages
– Weakly correlated with the magnitude of LV hypertrophy
– Do not distinguish the obstructive and nonobstructive forms
32. • Echocardiogram:
septum 1.3 times the thickness of the posterior LV free wall
SAM of the mitral valve + MR is found in pts with pressure
gradients
33. CMRI
• More accurate than echo
• Can detect 6% more hypertrophy
• Accurate measurement of thickness
• Should be done in
Poor echo window
Discrepancy between Clinical findings / ECG / Echo
34. Wall Thickness and Sudden Death
in HCM
Spirito P. N Engl J Med. 2000;342:1778-
1785.
0
2
4
6
8
10
12
14
16
18
20
< 15 16-19 20-24 25-29 > 30
Maximum Left-Ventricular-Wall Thickness (mm)
Incidence
of
Sudden
Death
(per
1,000
person/yr)
0
2.6
7.4
11.0
18.2
35. BURNT OUT HCM
• Occurs : 3 % of pts with HCM
• Systolic dysfunction with EF <50%
• Wall thinning and cavity dilation
• Diffuse transmural scarring
• Associated with AF
• Progression to refractory heart failure or sudden death is
frequent (10%/year)
• Most reliable risk marker - a family history of the end stage
36. Natural History of HCM
• Heart Failure
– Only 10-15% progress to
NYHA III-IV
– Only 3% will become truly
end-stage with systolic
dysfunction
• Endocarditis
– 4-5% of HCM patients
– Usually mitral valve
affected
• Atrial Fibrillation
– Prevalent in up to 30% of
older patients
– Dependent on atrial kick – CO
decreases by 40% if AF
present
• Autonomic Dysfunction
– 25% of HCM patients
– Associated with poor
prognosis
37. Athlete's Heart Vs Hypertrophic Cardiomyopathy
HCM
• Can be asymmetric
• Wall thickness: > 15 mm
• LA: > 40 mm
• LVEDD : < 45 mm
• Diastolic function: always
abnormal
Athletic heart
• Concentric & regresses
• < 15 mm
• < 40 mm
• > 45 mm
• Normal
38. Treatment
• Competitive sports and very strenuous activities should be avoided
• Dehydration should be avoided, and diuretics used with caution
• B-Adrenergic blockers and Verapamil :
• ameliorate angina pectoris and syncope in 30-50% of patients
• may limit the increase in the gradient that occurs during exercise
• Amiodarone:
• reduces the frequency of supraventricular as well as of life-threatening
ventricular arrhythmias
• reduces the risk of SCD
38
39. • Screening all first-degree relatives is recommended
– Echocardiography
• Children & participating in competitive athletics Every
12 to 18 months
• Adults no competitive athletics - every 5 years
39
Treatment
40. • Surgical myotomy/myectomy
abolishes intraventricular
obstruction and provides lasting
symptomatic improvement in
about three-quarters of severely
symptomatic patients
unresponsive to medical
management
• alcohol septal ablation
40
Treatment
42. • Least Common
• Fibrotic or infiltrated
myocardium
• Non-dilated ventricles
with dilated atria
• The hallmark is abnormal diastolic function
The ventricular walls are excessively rigid and impede ventricular
filling
Normal systolic function except In late stages.
Restrictive Cardiomyopathy
43. • In many of these conditions, particularly those with substantial
concomitant endocardial involvement, partial obliteration of
the ventricular cavity by fibrous tissue and thrombus
contributes to the abnormally increased resistance to ventricular
filling
Thromboembolic complications are frequent in such patients
43
Restrictive Cardiomyopathy
44. Clinical Features
• Hallmarks of Disease
Symptoms and signs of heart failure with predominant right-sided findings.
Normal left and right ventricular size and systolic function with dilated atria.
Diastolic ventricular functional abnormalities suggestive of reduced ventricular
compliance ( stiffness)
• Exercise intolerance and dyspnea are usually prominent
– As inability of the ventricles to fill limits cardiac output and raises filling
pressures
• JVP is elevated and does not fall normally with inspiration (Kussmaul's sign)
44
48. Ventricular arrhythmias
– SCD in young
ECG shows QRS prolongation in right precordial
leads
CMRI typically show RV dilatation, RV
aneurysm, and fatty replacement
48
Arrhythmogenic Right Ventricular
Cardiomyopathy/Dysplasia
49. Tako-Tsubo Cardiomyopathy
• Also known as apical ballooning syndrome
• characterized by the abrupt onset of severe chest discomfort
preceded by a very stressful emotional or physical event
• most common in women >50 years and is accompanied by ST-
segment elevations and/or deep T-wave inversions in the
precordial leads
– No obstruction in the epicardial coronary arteries is noted on angiography
– There is severe akinesia of the distal portion of the left ventricle with
reduction of the EF
• Troponins are usually mildly elevated
49
50. • Cardiac imaging typically shows "ballooning" of the left ventriclar
apex in end-systole
– these changes, are reversible within 3–7 days and do not cause long-term
cardiac dysfunction or disability
• Mechanism responsible is not clear
– likely an adrenergic surge that includes circulating catecholamines, acting
on the epicardial coronary vessels and/or coronary microcirculation is in
involved.
• Rx: BB?
50
Tako-Tsubo Cardiomyopathy
51. Summary
• Cardiomyopathies are diseases of the heart
muscle and are classified based on their
structural and functional phenotype
• Disorders are frequently genetic
• Accurate differentiation is needed in order to
guide treatment and management