Rheumatoid Arthritis
•Download as PPTX, PDF•
420 likes•287,811 views

Student Seminar Presentation under supervision of orthopedic specialist. Reference as mentioned in the slides.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Rheumatoid Arthritis
Similar to Rheumatoid Arthritis (20)
More from yuyuricci
More from yuyuricci (20)
Recently uploaded
Recently uploaded (20)
Rheumatoid Arthritis
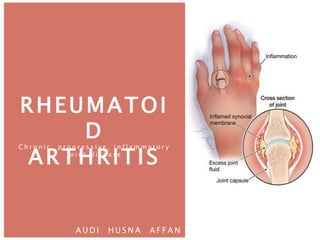
- 1. RHEUMATOI D ARTHRITIS A U D I H U S N A A F F A N C h r o n i c , p r o g r e s s i v e , i n f l a m m a t o r y j o i n t d i s e a s e
- 2. INTRODUCTION The most common cause of chronic inflammatory joint disease Most typical features: a. A symmetrical polyarthritis and tenosynovitis b. Morning stiffness c. Elevation of the erythrocyte sedimentation rate (ESR) d. Appearance of autoantibodies that target immunoglobins in the serum It is a systemic autoimmune disease and changes can be widespread in a number of tissues of the body RA tend to die younger than their peers as a result of the effects of chronic inflammation on a number of organ systems Chief among these is early ischemic heart disease secondary to the effects of inflammation on the cardiovascular system.
- 3. EPIDEMIOLOGY Affects 1 – 3% of the population world wide With a peak prevalence between the ages of 30 and 50 years Women are affected 3 or 4 times more commonly than men
- 4. CAUSES Important factors in the evolution of RA are: a. Genetic susceptibility b. An immunological reaction; possible involving a foreign antigen, preferentially focused on synovial tissue c. An inflammatory reaction in joints and tendon sheaths d. The appearance of rheumatoid factors in the blood and synovium e. Perpetuation of the inflammatory process f. Articular cartilage destruction
- 5. PATHOLOGY RA is a systemic disease but the most characteristic lesions are seen in the synovium or within rheumatoid nodules. The synovium is engorged with new blood vessels and packed full of inflammatory cells
- 6. PATHOLOGY Before RA becomes clinically apparent the immune pathology is already beginning. Raised ESR, C-reactive protein (CRP), and RF may be detectable years before the first diagnosis. STAGE 1 – pre-clinical
- 7. PATHOLOGY Early changes are: a. Vascular congestion with new blood vessel formation b. Proliferation of synoviocytes c. Infiltration of the sub synovial layers by polymorphs, lymphocytes and plasma cells. There is thickening of the capsular structures, villous formation of the synovium and a cell-rich effusion into the joints and tendon sheath. STAGE 2 – synovial
- 8. PATHOLOGY Persistent inflammation causes joint and tendon destruction. Articular cartilage is eroded. At the margins of the joint, bone is also eroded by granulation tissue invasion and osteoclastic resorption. Similar changes occur in tendon sheaths, causing tenosynovitis. Partial or complete rupture of tendons. Swelling of the joints, tendons and bursae. STAGE 3 - destruction
- 9. PATHOLOGY Combination of articular destruction, capsular stretching and tendon rupture leads to progressive instability and deformity of the joints. The inflammatory process usually continues but the mechanical and functional effects of joint and tendon disruption now become vital. STAGE 4 – deformity
- 10. CLINICAL FEATURES Early feature (synovitis) I. Most commonly affected MCPJ and PIPJ, wrist, tendon sheaths around the joints (wrist – feet – knee – shoulder) II. Bilateral symmetrical polysynovitis III. Pain, fusiform swelling, stiffness, loss of mobility IV. Constitutional symptom: a. LOA, LOW, malaise and low grade fever b. Tenosynovitis
- 12. CLINICAL FEATURES Late feature (DESTRUCTIVE) I. Spread to other joint – wrist, ankle, knee, shoulder (in order of frequency) II. Morning stiffness (more than 30 min) – improve with activity III. Activity of daily living will be affected – quality of life affected
- 14. CLINICAL FEATURES More later (DEFORMITY) I. Pain, deformity, instability, decreased ROM II. Joint deformity – movement restricted and painful Thumb – Z-deformity Fingers – Swan neck deformity/ Boutonniere’s deformities, ulnar deviation Wrist – radial and volar displacement Elbow – limited extension Shoulder - limited abduction Knees – swollen, flexion an vulgus Toes – clawed
- 18. DIAGNOSIS Mostly clinical: I. Bilateral, symmetrical polyarthritis II. Involving proximal joints of hand or feet III. Present for at least 6 weeks IV. Confirmed with subcutaneous nodules or periarticular erosions on x-ray
- 19. CLASSIFICATION E U L A R R H E U M ATO I D A R T H R I T I S C L A S S I F I C AT I O N C R I T E R I A
- 20. INVESTIGATION H E M ATO LO G I C A L 1. FBC- normocytic hypochromic anaemia (due to abnormal erythropoiesis from chronic inflammation), WBC 2. Inflammatory markers- ESR, CRP elevated (its use as indication of disease progression monitoring, treatment response) 3. Rheumatoid factor(RF)- anti-IgG auto Ab 80% will have it 4. Anti- cyclic citrullinated peptide(CCP) Ab
- 21. INVESTIGATION J O I N T A S P I R AT I O N
- 22. INVESTIGATION I M A G I N G For disease monitoring, treatment response. EARLY STAGE(SYNOVITIS) Soft tissue swelling, periarticular osteopenia LATER STAGE(DESTRUCTIVE) Juxta- erosions, narrowing of joint space ADVANCE STAGE(DEFORMITY) Articular destruction and joint deformity
- 23. INVESTIGATION I M A G I N G
- 24. MANAGEMENT There is no cure for rheumatoid arthritis Aim to delay the progression of the disease, alleviate symptoms, reduce functional limitation Supportive and palliative
- 25. MEDICATION 1. NSAIDs Ibuprofen, indomethacin, COX-2 inhibitors like celecoxib and valdecoxib (reduce inflammation and relieves pain) 2. Analgesics Morphine and acetaminophen (reduce pain) 3. Glucocorticoids or prednisolone Prescribed in a small dose to slow joint damage caused by inflammation
- 26. SURGERY Improve quality of life Synovectomy When one or two joints are affected more severely than others, this procedure is used to reduce the amount of inflammatory tissue by removing the diseased synovium or lining of the joint. It may result in less swelling and pain and the slowing or prevention of further joint damage Arthroscopic Surgery Thin tube with a light at the end inserted into the joint through a small incision. It is connected to a closed-circuit television and we can see the extent of the damage in the joint. Tissue samples taken, remove loose cartilage, repair tears, smooth a rough surface or remove diseased synovial tissue. It is most commonly performed on the knee and shoulder
- 27. MEDICATION 4. Disease Modifying Antirheumatic Drugs (DMARD) There are used with NSAIDs and/or prednisolone to slow joint destruction caused by RA over time. Examples are methotrexate, injectable gold, penicillamine, azathioprine, chloroquine, hydroxychloroquine, sulfasalazine and oral gold. 5. Biologic Response Modifiers These drugs directly modify the immune system by inhibiting proteins called cytokines, which contribute to inflammation. Examples of these are abatacept, etanercept, infliximab, adalimumab, and anakinra. 6. Protein – A Immunoadsorption Therapy This is not a drug, but a therapy that filters the blood to remove antibodies and immune complexes that promote inflammation
- 28. SURGERY Osteotomy Literally meaning, “to cut bone,” this procedure is used to increase stability by redistributing the weight on the joint. Osteotomy isn’t often used with RA because there are other options available besides cutting the bones. Joint Replacement Surgery or Arthroplasty This is the surgical reconstruction or replacement of a joint. Successfully used to help people who otherwise might be in a wheelchair, joint replacement surgery involves the removal of the joint, resurfacing and relining of the ends of bones and replacing the joint with a man-made component. This procedure is usually recommended for people over 50 or who have severe disease progression. Typically a new joint will last between 20 and 30 years Arthrodesis or fusion This procedure fuses two bones together. While it limits movement, it does decrease pain and increase stability of the joints in the ankles, wrists, fingers, toes and spine.
- 29. TREATMENT • Onset of disease o NSAIDs/analgesic o Exercise • Early ( 1st 6-12 month ) o NSAIDs, analgesic, low dose corticosteroid o Disease modifying drug o Physiotherapy o Splintage • Progressive erosive (1-5 years) o Disease modifying drug o Splintage o Surgical management ( synovectomy, arthroscopic surgery ), late ( 5-20 years) o Reconstructive surgery ( arthrodesis, osteotomy, arthroplasty)
- 30. COMPLICATION Fixed deformities Muscle weakness Infection Spinal cord compression Systemic vasculitis Amyloidosis- Renal failure