Corneal anatomy physiology and wound healing
•
8 j'aime•5,189 vues

Ophthalmology Yanoff Corneal Anatomy, Phisiology and Wound Healing - C. 4.1

Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
En vedette (20)
Similaire à Corneal anatomy physiology and wound healing
Similaire à Corneal anatomy physiology and wound healing (20)
Plus de Socrates Narvaez
Plus de Socrates Narvaez (20)
Dernier
Dernier (20)
Corneal anatomy physiology and wound healing
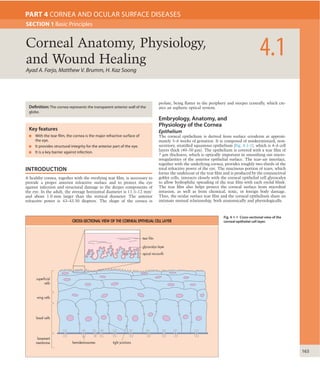
- 1. 163 INTRODUCTION A healthy cornea, together with the overlying tear film, is necessary to provide a proper anterior refractive surface and to protect the eye against infection and structural damage to the deeper components of the eye. In the adult, the average horizontal diameter is 11.5–12 mm1 and about 1.0 mm larger than the vertical diameter. The anterior refractive power is 43–43.50 diopters. The shape of the cornea is prolate, being flatter in the periphery and steeper centrally, which cre- ates an aspheric optical system. Embryology, Anatomy, and Physiology of the Cornea Epithelium The corneal epithelium is derived from surface ectoderm at approxi- mately 5–6 weeks of gestation. It is composed of nonkeratinized, non- secretory, stratified squamous epithelium (Fig. 4-1-1), which is 4–6 cell layers thick (40–50 μm). The epithelium is covered with a tear film of 7 μm thickness, which is optically important in smoothing out micro- irregularities of the anterior epithelial surface. The tear–air interface, together with the underlying cornea, provides roughly two-thirds of the total refractive power of the eye. The mucinous portion of tears, which forms the undercoat of the tear film and is produced by the conjunctival goblet cells, interacts closely with the corneal epithelial cell glycocalyx to allow hydrophilic spreading of the tear film with each eyelid blink. The tear film also helps protect the corneal surface from microbial invasion, as well as from chemical, toxic, or foreign body damage. Thus, the ocular surface tear film and the corneal epithelium share an intimate mutual relationship, both anatomically and physiologically. Ayad A. Farjo, Matthew V. Brumm, H. Kaz Soong 4.1Corneal Anatomy, Physiology, and Wound Healing SECTION 1 Basic Principles PART 4 CORNEA AND OCULAR SURFACE DISEASES Definition: The cornea represents the transparent anterior wall of the globe. Key features ■ With the tear film, the cornea is the major refractive surface of the eye. ■ It provides structural integrity for the anterior part of the eye. ■ It is a key barrier against infection. Fig. 4-1-1 Cross-sectional view of the corneal epithelial cell layer. superficial cells apical microvilli glycocalyx layer tear film wing cells basal cells basement membrane hemidesmosomes tight junctions CROSS-SECTIONAL VIEW OF THE CORNEAL EPITHELIAL CELL LAYER
- 2. 4 164 CORNEAANDOCULARSURFACEDISEASES the corneal thickness. The stroma differs from other collagenous struc- tures in its transparency and biomechanical properties. These func- tional properties result from the precise organization of stromal fibers and extracellular matrix.7–9 The fibers are aligned in a parallel fashion within each lamella, and arranged at angles relative to fibers in adjacent lamellae.10,11 This network reduces forward light scatter and contrib- utes to the mechanical strength of the cornea. The peripheral stroma is thicker than the central stroma and the collagen fibrils may change direction to run circumferentially as they approach the limbus.11,12 Bowman’s membrane is the acellular condensate of the most anterior portion of the stroma. The stromal collagen fibrils, which provide the major tensile strength to the cornea, are composed mostly of type I collagen, but require a heterodimeric complex with type V collagen to obtain their unique and narrow diameter.13–15 They are surrounded by specialized proteoglycans, consisting of keratan sulfate or chondroitin sulfate/ dermatan sulfate side chains, which help regulate hydration and struc- tural properties. Keratocytes are the major cell type of the stroma and are involved in maintaining the extracellular matrix environment.16 More keratocytes are situated in the anterior stroma than in the poste- rior stroma. Morphological differences between the anterior and poste- rior stromal keratocytes, such as fenestrations, have been identified.17 Corneal “crystallins,” representing 25–30% of soluble protein in kera- tocytes, appear to be responsible for reducing backscatter of light from the keratocytes and maintaining corneal transparency.18 Corneal shape and curvature are governed by the intrinsic biome- chanical structure and extrinsic environment (Fig. 4-1-3). Anterior corneal stromal rigidity in particular appears to be important in main- taining the corneal curvature.19 Organizational differences in the col- lagen bundles of the anterior stroma may contribute to a tighter cohesive strength in this area and may explain why the anterior curva- ture resists change to stromal hydration much more than the posterior stroma, which tends to more easily develop folds. Corneal nerves and sensation are derived from the nasociliary branch of the first (ophthal- mic) division of the trigeminal nerve. In the superficial cornea, the nerves enter the stroma radially in thick trunks forming plexiform arrangements, which eventually perforate Bowman’s membrane to provide a rich plexus beneath the basal epithelial layer.20 The fibers appear to directly communicate with keratocytes and epithelial cells21 and may play an important role in corneal homeostasis. Endothelium In early embryogenesis, the posterior cornea is lined with a neural crest-derived22 monolayer of orderly arranged cuboidal cells.23 By the 78 mm stage, the cells become flattened and tightly abut one another. At this stage, immediately anterior to the flattened layer is a discon- tinuous, homogeneous acellular layer, which in time becomes Descemet’s membrane.24 By the 120 mm and 165 mm stages of devel- opment, the endothelial monolayer is uniform in thickness, spans the entire posterior corneal surface, and fuses with the cells of the trabecu- lar meshwork.24 Similarly, Descemet’s membrane becomes continuous and uniform, fusing peripherally with the trabecular beams.24 The Fig. 4-1-2 Whorl-like deposition keratopathy in corneal epithelium seen in Fabry’s disease. Corneal epithelial cells undergo orderly involution, apoptosis, and desquamation. Complete turnover of corneal epithelial cells occurs in about 7–10 days,2 with the deeper cells eventually replacing the de- squamating superficial cells in an apically directed fashion. The most superficial cells of the corneal epithelium form an average of two to three layers of flat, polygonal cells. Extensive apical microvilli and microplicae characterize the cell membranes of the superficial cells, which in turn are covered by a fine, closely apposed, charged glycocal- yceal layer. The apical membrane projections increase the surface area of contact and adherence between the tear film’s mucinous undercoat and the cell membrane. Laterally, adjacent superficial cells are joined by barrier tight-junctional complexes, which restrict entry of tears into the intercellular spaces. Thus, a healthy epithelial surface repels dyes such as fluorescein and rose bengal. Beneath the superficial cell layer are the suprabasal or wing cells, so named for their cross-sectional alar shapes. This layer is about 2–3 cells deep and consists of cells that are less flat than the overlying superficial cells, but possess similar tight, lateral, intercellular junctions. Beneath the wing cells are the basal cells, which comprise the deepest cellular layer of the corneal epithelium. The basal cell layer is composed of a single-cell layer of columnar epithelium approximately 20 μm tall. Besides the stem cells and transient amplifying-cells, basal cells are the only corneal epithelial cells capable of mitosis.3,4 They are the source of both wing and superficial cells, and possess lateral intercellular junc- tions characterized by gap junctions and zonulae adherens. The basal cells are attached to the underlying basement membrane by an exten- sive basal hemidesmosomal system. This attachment is of pivotal importance in preventing the detachment of the multilayer epithelial sheet from the cornea. Abnormalities in this bonding system may result clinically in either recurrent corneal erosion syndromes or in persistent, nonhealing epithelial defects. The basement membrane is composed of an extracellular matrix material secreted by the basal cells. Following destruction of the base- ment membrane, about 6 weeks are required for it to reconstitute and heal. The epithelial bond to the underlying, newly laid basement mem- brane tends to be unstable and weak during this period. The epithelium also adheres relatively poorly to bare stroma or Bowman’s layer. Under ordinary conditions, type IV collagen and laminin are the major com- ponents of the basement membrane; however, fibronectin production increases to high levels during acute epithelial injury. The basement membrane, approximately 0.05 μm in thickness, adheres to the under- lying Bowman’s membrane through a poorly understood mechanism that involves the anchoring fibrils and plaques.5 Epithelial stem cells – undifferentiated pluripotent cells that serve as an important source of new corneal epithelium – have been localized to the limbal basal epithelium. As the cells migrate to the central cornea, they differentiate into transient amplifying cells (cells capable of multi- ple, but limited cellular division) and basal cells. The corneal epithelial cell layer mass appears to be the complex resultant of three phenomena. According to the ‘X, Y, Z hypothesis,” X is the proliferation of basal epithelial cells, Y is the centripetal mass movement of peripheral epithe- lial cells, and Z is the cell loss resulting from death and desquamation.6 These three phenomena probably are not totally independent of each other, but rather are controlled by a complex interactive feedback mecha- nism that maintains the status quo, vis-à-vis cell density, cell distribu- tion and polarity, and cell layer thickness. These cytodynamics are likely to be responsible for the striking verticillate (vortex or whorl-like) bio- chemical deposition patterns seen in Fabry’s disease (Fig. 4-1-2) and drug deposition keratopathies (e.g., from chloroquine and amiodarone). Langerhans cells, immunologically active dendritic macrophages derived from bone marrow and capable of antigen processing, are present in the peripheral corneal epithelium near the limbus. Under certain conditions (e.g. corneal graft rejection or injury), these cells are found among the central corneal epithelial cells. Human lymphocyte antigens are expressed by these corneal Langerhans cells. Langerhans cells have also been detected in the epithelial basal cell layer and in Bowman’s mem- brane in pathological inflammatory conditions such as Thygeson’s superficial punctate keratitis. After treatment with topical steroids, these cells are no longer detectable by laser confocal microscopy.7 Stroma In the seventh week of gestation, after the establishment of the primi- tive endothelium, a second wave of neural crest cells form the early corneal stroma. Akin to the dermis of the skin, the corneal stroma provides important structural integrity and comprises roughly 85% of
- 3. CornealAnatomy,Physiology,andWoundHealing 4.1 165 adhesion to Descemet’s membrane. Endothelial cells contain numer- ous mitochondria and a prominent Golgi apparatus, and continuously secrete Descemet’s membrane throughout life, beginning in utero at the 8-week stage. The anterior portion of Descemet’s membrane formed in utero has a distinctive banded appearance when viewed by electron microscopy, but Descemet’s membrane produced after birth is unbanded and has an amorphous ultrastructural texture. This mem- brane is approximately 3 μm thick at birth, but thickens to 10 μm with age. Endothelial cell density and topography also continue to change throughout life. From the second to eighth decades of life, the cell density declines from approximately 3000–4000 cells/mm2 to around 2600 cells/mm2 , and the percentage of hexagonal cells declines from about 75% to around 60%.28 The central endothelial cell density decreases at an average rate of 0.3% per year in normal corneas.29 As a result of endothelial activity, the stroma is maintained in a rela- tively deturgesced state (78% water content).30 One hypothesis is that this endothelial activity is mediated by a pump–leak process; net fluid egress from the corneal stroma follows movement down an osmotic gradient from a relatively hypo-osmotic stroma toward a relatively hypertonic aqueous humor. This passive bulk fluid movement requires no energy. The energy-requiring processes are the intracellular and membrane-bound ion transport systems, which generate the osmotic gradient. The two most important ion transport systems are the membrane-bound Na+ ,K+ -ATPase sites and the intracellular carbonic anhydrase pathway.31 Activity in both these pathways produces a net flux from stroma to aqueous humor. The barrier portion of the endothelium is unique, in that it is permeable to some degree, permit- ting the ion flux necessary to establish the osmotic gradient.24,26 Little, if any, in vivo mitotic potential exists within the endothelium. Although the exact minimum number of cells/mm2 required to main- tain corneal deturgescence is not known, corneas with cell counts below 500 cells/mm2 may be at risk for development of corneal edema. Endothelial cell morphology (size and shape) appears to also correlate with pump function. An increase in cell size (polymegathism) and an increase in variation of cell shape (pleomorphism) correlate to reduced ability of the endothelial cells to deturgesce the cornea.32,33 In vivo assessment of endothelial function relies on measurements of corneal thickness or on clinical morphological studies of the endothelial monolayer with specular microscopy. Measurement of the corneal thickness (pachymetry) indirectly reflects endothelial function. The average central corneal thickness is around 0.5 mm, which gradu- ally increases toward the periphery to around 0.7 mm. Normally, as a diurnal variation, corneas tend to be slightly thicker just after a person awakes in the morning. This increase in thickness is the consequence of diminished evaporation of water from underneath the closed eyelids, and the result of reduced nocturnal metabolic activity of the endothe- lium. Such overnight corneal swelling is more exaggerated in persons with unhealthy endothelium, causing blurred vision in the morning that gradually resolves later during the day. Endothelial Responses to Stress Mild endothelial stress may result in cell size and shape changes, while greater stress may result in cell loss as well as irreversible alterations in the endothelial cytoskeleton.34 Sources of stress may be metabolic (from hypoxia or hyperglycemia), toxic (from drugs or their preserva- tives), injury (from trauma or surgery), or alterations in pH or osmolar- ity. For example, contact lenses cause a hypoxic stress of varying degree to the endothelium.35 Over time, this may result in alteration of the morphology, microanatomy, and possibly the function of the endothe- lium.36,37 Hyperglycemia is another common metabolic stress that may produce changes in the endothelium. When compared with age- matched controls, the corneal endothelium in patients with type 1 and type 2 diabetes has a lower mean cell density and greater pleomorphism and polymegathism.38,39 Tissue manipulation, fluid flow in the anterior chamber, and intrac- ameral pharmacological agents introduced during anterior segment surgery may cause damage to the endothelium.40,41 Ophthalmic visco- elastic materials (composed of hydroxypropyl methylcellulose, chon- droitin sulfate, or sodium hyaluronate) provide significant protection against intraoperative trauma to the endothelium.42,43 Glaucoma has been associated with endothelial cell loss. Compared with age-matched controls, significantly lower endothelial cell counts were noted in patients with glaucoma and ocular hypertension in one study.44 Cell counts were inversely proportional to the mean intraocular fusion site, known as Schwalbe’s line, is a gonioscopic landmark that defines the end of Descemet’s membrane and the start of the trabecular meshwork. At birth, the endothelium is approximately 10 μm thick.25 The intact human endothelium is a monolayer, which appears as a honeycomb-like mosaic when viewed from the posterior side (Fig. 4-1- 4). The individual cells continue to flatten over time and stabilize at about 4 μm in thickness in adulthood (Fig. 4-1-5).26 The posterior sur- face of the endothelium is devoid of villi, except in certain pathological conditions, in which it may develop epithelioid characteristics. Adja- cent cells share extensive lateral interdigitations, and possess gap and tight junctions along their lateral borders. The lateral membranes con- tain a high density of Na+ ,K+ -ATPase pump sites.27 The basal surface of the endothelium contains numerous hemidesmosomes that promote Fig. 4-1-3 Major corneal loading forces in the steady state. (Illustration courtesy ofWilliam J. Dupps, MD, PhD.) MAJOR CORNEAL LOADING FORCES IN THE STEADY-STATE intraocular pressure swelling pressure epithelial barrier intralamellar cohesive forces lamellar tension endothelial pump endothelial barrier Fig. 4-1-4 Specular photomicrograph of normal endothelium. Note the dark, well-defined cell borders, the regular hexagonal array, and the uniform cell size. (Bar = 50 μm.). Fig. 4-1-5 Light micrograph of normal endothelium (×100). Note the single-cell endothelial layer with a Descemet’s membrane of uniform thickness (epithelial surface at top of figure). (Courtesy of Dr David Barsky.) endothelium Descement's membrane Bowman's membrane epithelium
- 4. 4 166 CORNEAANDOCULARSURFACEDISEASES and/or dystrophies), ocular surface inflammation or atopic disease, medicamentosa, dry eyes, neurotrophic and exposure keratopathies, conjunctival disease (e.g., pemphigoid, radiation keratoconjunctivitis, and Stevens–Johnson syndrome), extensive damage to the limbal stem cells, and eyelid abnormalities. The epithelial healing problems of postinfectious (metaherpetic) ulceration, seen after acute herpetic keratitis, are believed to be caused by damage to the basement membrane from antiviral drug toxicity or from overzealous iatrogenic scraping of the corneal surface using either mechanical or chemical means.49 In neurotrophic corneas it is possible that interruption of corneal innervation results in depletion of sub- stance P, a neurogenic chemical known to regulate corneal physiological functions. Diabetic corneas may manifest abnormally thickened and easily delaminated basement membranes (Fig. 4-1-7), perhaps akin to basement membrane abnormalities elsewhere, as in the renal glomer- uli.45 A combination of pharmacological interruption of corneal nerve function and damage to the epithelial cells and substrate may cause persistent epithelial defects associated with topical anesthetic abuse.50,51 Limbal stem cell deficiency is an increasingly recognized cause of nonhealing epithelial defects. Evidence also implicates matrix metalloprotease-9 (gelatinase B) as a factor that may impact epithelial healing and/or desquamation.52,53 Stromal Injury Similar to skin, stromal wound healing consists of repair, regeneration, and remodeling,13 involving a complex interplay of cytokines, growth factors, and chemokines.54 Importantly, stromal repair differs from dermatological healing in that it occurs avascularly and ideally main- tains corneal clarity. The reparative cascade begins with activation of stromal keratocytes (Fig. 4-1-8), which enlarge in size within the first 6 hours after injury and migrate into the injured area within 24 hours, becoming more fibroblast-like in appearance and behavior.55 Activation of the keratocytes may be triggered by epithelial factors.55 The repara- tive cascade that follows typically results in corneal opacity in the affected area. The keratocytes within the area of injury undergo apop- tosis, peaking 4 hours after the initial insult.56 Apoptosis appears to modulate the wound healing response by influencing the activation of adjacent keratocytes. Within 1–2 weeks, myofibroblasts with contractile properties enter the area under the epithelium and become involved in the remodeling of the stroma, with increased expression of matrix metalloproteas- es.13,57 These cells may be responsible for the “haze” seen after corneal injury or surgery. The remodeling process can sometimes continue over a prolonged period of several years, and may eventually restore corneal clarity in the affected area. Certain corneal surgeries, such as laser in situ keratomileusis, cause a progressive loss of keratocytes over time through an as yet unclear mechanism.58 pressure in the glaucoma and ocular hypertension groups. Mechanisms of cell loss may include direct damage from intraocular pressure, con- genital alterations of endothelium in glaucoma, and drug toxicity.45 CORNEAL WOUND HEALING Epithelial Injury Within minutes after a small corneal epithelial wound, cells at the edge of the abrasion begin to cover the defect as rapidly as possible by a combination of cell migration and cell spreading. A longer delay of up to 4–5 hours is seen in larger defects. This lag phase is necessary for the preparatory cellular changes of an anatomical, physiological, and biochemical nature to occur before rapid cell movement. Various cell membrane extensions, such as lamellipodia, filopodia, and ruffles, develop at the leading edge of the wound. Anchoring hemidesmosomes disappear from the basal cells. This early nonmitotic wound coverage phase is remarkable for its speed; the cells have been measured to migrate at a rate of 60–80 μm/h (Fig. 4-1-6).46 The migrating sheet of epithelial cells is attached most firmly to the underlying substrate at the leading margin. The relatively firmer adhesion at the leading mar- gin suggests that the epithelial sheet movement may have “front-wheel drive,” with the less well-anchored cells behind the leading margin being pulled forward, possibly by intracellular contractile mechanisms that involve actin.47 Fibronectin, a ubiquitous extracellular matrix pro- tein present in plasma and in fresh wounds, is thought to be one of the key elements in the mediation of cell-to-substrate adhesion and cell migration. Present on the extracellular side of adhesion plaques, it is thought to mediate the linkage between the vinculin–talin–integrin complex and the substrate during epithelial migration after a wound has occurred. Laminin, a less ubiquitous extracellular matrix protein, is thought to serve a similar function. At 24–30 hours after medium-sized epithelial injuries, mitosis or cell proliferation begins and restores the rarefied epithelial cell popula- tion. After large epithelial injuries, significant increases in cellular divi- sion occur as late as 96 hours.48 Only the basal cells, transient amplifying cells, and the limbal stem cells partake in this reconstitutive mitosis.3,4 In laboratory and clinical trials, agents known to influence epithelial migration, mitosis, apoptosis, adhesion, and differentiation have been studied as possible therapeutic agents to enhance corneal epithelial healing, including growth factors, fibronectin, and retinoids. Primarily mitogenic agents and growth factors also stimulate produc- tion of extracellular matrix components to enhance cell-to-substrate adhesion. Various pathological conditions may delay or prevent the normal corneal epithelial healing process. These include the following: damage to the cellular substrate (caused by herpetic or other infectious disease, diabetes mellitus, chemical burns, or basement membrane injuries Fig. 4-1-6 Light micrograph that shows the leading edge of migrating rat corneal epithelium as it tapers to a layer of one-cell thickness. As the epithelial defect is rapidly covered by migrating cells, it is initially coated with a thin, rarefied cell population prior to onset of mitotic activity (hematoxylin & eosin). Fig. 4-1-7 Recurrent erosion in a diabetic cornea. Note the abnormally thick basement membrane (asterisk) and the intralamellar split within (arrow) (hematoxylin & eosin). *
- 5. CornealAnatomy,Physiology,andWoundHealing 4.1 167 enlargement of the surrounding cells and their centripetal migration into the injured region. Clinically, by slit-lamp biomicroscopy, these endothelial lesions disappear 1–3 days after injury. With more severe trauma, the underlying Descemet’s membrane may even be torn or ruptured, as in forceps delivery injuries and in corneal hydrops in kera- toconus. When injured, Descemet’s membrane curls in toward the stroma and surrounding endothelial cells slide in to cover the defect and produce new Descemet’s membrane. Although normal endotheli- um does not appear to replicate in vivo, recent evidence suggests that endothelial cells retain a degree of latent proliferative potential even into adulthood.59 KEY REFERENCES Bonanno JA. Molecular mechanisms underlying the corneal endothelial pump. Exp Eye Res 2012;95:2–7. Fini ME, Stramer BM. How the cornea heals: cornea-specific repair mechanisms affecting surgical outcomes. Cornea 2005;24:S2–SS11. Kawamoto K, Chikama T, Takahashi N, et al. In vivo observation of Langerhans cells by laser confocal microscopy in Thygeson’s superficical punctate keratitis. Mol Vis 2009;15:1456–62. Maurice DM. The structure and transparency of the corneal stroma. J Physiol 1957;136:263–86. Netto MV, Mohan RR, Ambrosio R Jr, et al. Wound healing in the cornea: a review of refractive surgery complications and new prospects for therapy. Cornea 2005;24:509–22. Oliveira-Soto L, Efron N. Morphology of corneal nerves using confocal microscopy. Cornea 2001;20:374–84. Pflugfelder SC, Farley W, Luo L, et al. Matrix metalloproteinase-9 knockout confers resistance to corneal epithelial barrier disruption in experimental dry eye. Am J Pathol 2005;166:61–71. Qazi Y, Wong, G, Monson B, et al. Corneal transparency: genesis, maintenance and dysfuction. Brain Res Bull 2010;81:198–210. Rao SK, Ranjan Sen P, Fogla R, et al. Corneal endothelial cell density and morphology in normal Indian eyes. Cornea 2000;19:820–3. Soong HK. Vinculin in focal cell-to-substrate attachments of spreading corneal epithelial cells. Arch Ophthalmol 1987;105:1129–32. Stiemke MM, Edelhauser HF, Geroski DH. The developing corneal endothelium: correlation of morphology, hydration and Na/K ATPase pump site density. Curr Eye Res 1991;10:145–56. Thoft RA, Friend J. The X, Y, Z hypothesis of corneal epithelial maintenance. Invest Ophthalmol Vis Sci 1983;24:1442–3. Van den Bruel A, Gailly J, Devriese S, et al. The protective effect of ophthalmic viscoelastic devices on endothelial cell loss during cataract surgery: a meta-analysis using mixed treatment com- parisons. Br J Ophthalmol 2011;95:5–10. Yee RW, Matsuda M, Schultz RO, et al. Changes in the normal corneal endothelial cellular pattern as a function of age. Curr Eye Res 1985;4:671–7. Endothelial Injury Nonperforating puncture injuries of the anterior cornea that do not directly involve the endothelium (e.g., those that occur when the cor- nea is struck by small, high-velocity particles) may cause concentric lesions of the endothelium arising from rapid focal distortion of the cell layer. Buckling of the endothelial layer can also result from excessive corneal bending in large-incision surgeries and/or from lens fragments striking the endothelium during cataract surgery, and may occasionally produce snail-track lesions, clinically seen as serpentine, grayish lines on the endothelium. The damaged cells are rapidly replaced by Fig. 4-1-8 Transmission electron micrograph of the corneal stroma. Activated keratocytes with dilated endoplasmic reticulum (inset: black arrow) and prominent nucleoli (white arrow) 1 week after keratoplasty. Bowman’s layer is at the upper border of the micrograph. A normal keratocyte (asterisk), noticeably smaller than the activated cells, is visible above the scale bar. (Bar = 5.0 μm.) (Reproduced with permission from Ohno K, Mitooka K, Nelson LR, et al. Keratocyte activation and apoptosis in transplanted human corneas in a xenograft model. Invest OphthalmolVis Sci 2002;43:1025–31.) Access the complete reference list online at
- 6. CornealAnatomy,Physiology,andWoundHealing 4.1 167.e1 REFERENCES 1. Rufer F, Schroder A, Erb C. White-to-white corneal diameter: normal values in healthy humans obtained with the Orbscan II topography system. Cornea 2005;24:259–61. 2. Hanna C, Bicknell DS, O’Brien JE. Cell turnover in the adult human eye. Arch Ophthalmol 1961;65:695–8. 3. Beebe DC, Masters BR. Cell lineage and the differentiation of corneal epithelial cells. Invest Ophthalmol Vis Sci 1996;37:1815–25. 4. Wiley L, SunderRaj N, Sun TT, et al. Regional heterogeneity in human corneal and limbal epithelia: an immunohistochemical evaluation. Invest Ophthalmol Vis Sci 1991;32:594–602. 5. Ehlers N, Heegaard S, Hjortdal J, et al. Morphological evaluation of normal human corneal epithelium. Acta Ophthalmol 2010;88:858–61. 6. Thoft RA, Friend J. The X, Y, Z hypothesis of corneal epithelial maintenance. Invest Ophthalmol Vis Sci 1983;24:1442–3. 7. Kawamoto K, Chikama T, Takahashi N, et al. In vivo observation of Langerhans cells by laser confocal microscopy in Thygeson’s superficical punctate keratitis. Mol Vis 2009;15:1456–62. 8. Qazi Y, Wong, G, Monson B, et al. Corneal transparency: genesis, maintenance and dysfuction. Brain Res Bull 2010;81:198–210. 9. Boote C, Dennis S, Newton RH, et al. Collagen fibrils appear more closely packed in the prepupillary cornea: optical and biomechanical implications. Invest Ophthalmol Vis Sci 2003;44:2941–8. 10. Maurice DM. The structure and transparency of the corneal stroma. J Physiol 1957;136: 263–86. 11. Meek KM, Boote C. The organization of collagen in the corneal stroma. Exp Eye Res 2004;78:503–12. 12. Kamma-Lorger CS, Boote C, Hayes S, et al. Collagen and mature elastic fibre organization as a function of depth in the human cornea and limbus. J Struct Biol 2010;169:424–30. 13. Fini ME, Stramer BM. How the cornea heals: cornea-specific repair mechanisms affecting surgical outcomes. Cornea 2005;24:S2–S11. 14. Sun M, Chen S, Adams SM, et al. Collagen V is a dominant regulator of collagen fibrillogenesis: dysfunctional regulation of structure and function in a corneal-stroma- specific Cola5a1-null mouse model. J Cell Sci 2011;124:4096–105. 15. Birk DE. Type V collagen: heterotypic type I/V collagen interactions in the regulation of fibril assembly. Micron 2001;32:223–37. 16. Hassell JR, Birk DE. The molecular basis of corneal transparency. Exp Eye Res 2010;91:326–35. 17. Ojeda JL, Ventosa JA, Piedra S. The three-dimensional microanatomy of the rabbit and human cornea. A chemical and mechanical microdissection – SEM approach. J Anat 2001;199:567–76. 18. Ren S, Liu T, Jia C, et al. Physiological expression of lens α-, β-, and γ-crystallins in murine and human corneas. Mol Vis 2010;16:2745–52. 19. Muller LJ, Pels E, Vrensen GFJM. The specific architecture of the anterior stroma accounts for maintenance of corneal curvature. Br J Ophthalmol 2001;85:437–43. 20. Oliveira-Soto L, Efron N. Morphology of corneal nerves using confocal microscopy. Cornea 2001;20:374–84. 21. Muller LJ, Pels L, Vrensen GF. Ultrastructural organization of human corneal nerves. Invest Ophthalmol Vis Sci 1996;37:476–88. 22. Beebe DC, Coats JM. The lens organizes the anterior segment: specification of neural crest cell differentiation in the avian eye. Dev Biol 2000;220:424–31. 23. Sevel D, Isaacs R. A reevaluation of corneal development. Trans Am Ophthalmol Soc 1988;136:178–207. 24. Watsky MA, McDermott ML, Edelhauser HF. In vitro corneal endothelial permeability in rabbit and human: the effects of age, cataract surgery and diabetes. Exp Eye Res 1989;49:751–67. 25. Nuijts RMMA. Ocular toxicity of intraoperatively used drugs and solutions. New Amsterdam: Kugler Publications; 1995. 26. Joyce NC. Proliferative capacity of corneal endothelial cells. Exp Eye Res 2012;95:16–23. 27. Stiemke MM, Edelhauser HF, Geroski DH. The developing corneal endothelium: correlation of morphology, hydration and Na/K ATPase pump site density. Curr Eye Res 1991;10:145–56. 28. Yee RW, Matsuda M, Schultz RO, et al. Changes in the normal corneal endothelial cellular pattern as a function of age. Curr Eye Res 1985;4:671–7. 29. Rao SK, Ranjan Sen P, Fogla R, et al. Corneal endothelial cell density and morphology in normal Indian eyes. Cornea 2000;19:820–3. 30. Bonanno JA. Molecular mechanisms underlying the corneal endothelial pump. Exp Eye Res 2012;95:2–7. 31. Riley M. Transport of ions and metabolites across the corneal endothelium. In: McDevitt D, editor. Cell biology of the eye. New York: Academic Press; 1982. p. 53–95. 32. Polse KA, Brand RJ, Cohen SR, et al. Hypoxic effects on corneal morphology and function. Invest Ophthalmol Vis Sci 1990;31:1542–54. 33. Odenthal MT, Gan IM, Oosting J, et al. Long-term changes in corneal endothelial morphology after discontinuation of low gas-permeable contact lens wear. Cornea 2005;24:32–8. 34. Kim EK, Geroski DH, Holly GP, et al. Corneal endothelial cytoskeletal changes in F-actin with aging, diabetes, and after cytochalasin exposure. Am J Ophthalmol 1992;114:329–35. 35. Patel SV, McLaren JW, Hodge DO, et al. Confocal microscopy in vivo corneas of long-term contact lens wearers. Invest Ophthalmol Vis Sci 2002;43:995–1003. 36. Polse KA, Brand RJ, Cohen SR, et al. Hypoxic effects on corneal morphology and function. Invest Ophthalmol Vis Sci 1990;31:1542–54. 37. Bonanno JA. Effects of contact lens-induced hypoxia on the physiology of the corneal endothelium. Optom Vis Sci 2001;78:783–90. 38. Roszkowska AM, Tringali CG, Colosi P, et al. Corneal endothelium evaluation in type I and type II diabetes mellitus. Ophthalmologica 1999;213:258–61. 39. Sudhir RR, Raman R, Sharma T. Changes in the corneal endothelial cell density and morphology in patients with type 2 diabetes mellitus: a population-based study. Cornea 2012;31:1119–22. 40. Hyndiuk RA, Schultz RO. Overview of the corneal toxicity of surgical solutions and drugs: and clinical concepts in corneal edema. Lens Eye Toxic Res 1992;9:331–50. 41. Joussen AM, Barth U, Cubuk H, et al. Effect of irrigating solution and irrigation temperature on the cornea and pupil during phacoemulsification. J Cataract Refract Surg 2000;26:392–7. 42. Van den Bruel A, Gailly J, Devriese S, et al. The protective effect of ophthalmic viscoelastic devices on endothelial cell loss during cataract surgery: a meta-analysis using mixed treatment comparisons. Br J Ophthalmol 2011;95:5–10. 43. Holzer MP, Tetz MR, Auffarth GU, et al. Effect of Healon5 and 4 other viscoelastic substances on intraocular pressure and endothelium after cataract surgery. J Cataract Refract Surg 2001;27:213–18. 44. Gagnon MM, Boisjoly HM, Brunette I, et al. Corneal endothelial cell density in glaucoma. Cornea 1997;16:314–18. 45. Taylor HR, Kimsey RA. Corneal epithelial basement membrane changes in diabetics. Invest Ophthalmol Vis Sci 1981;20:548–53. 46. Matsuda M, Ubels JL, Edelhauser HF. A larger corneal epithelial wound closes at a faster rate. Invest Ophthalmol Vis Sci 1985;26:897–900. 47. Soong HK. Vinculin in focal cell-to-substrate attachments of spreading corneal epithelial cells. Arch Ophthalmol 1987;105:1129–32. 48. Arey LB, Cavode WM. The method of repair in epithelial wounds of the cornea. Anat Rec 1943;86:75–82. 49. Kaufman HE. Epithelial erosion syndrome: Metaherpetic keratitis. Am J Ophthalmol 1964;57:983–7. 50. Yagci A, Bozkurt B, Egrilmez S, et al. Topical anesthetic abuse keratopathy: a commonly overlooked health care problem. Cornea 2011;30:571–5. 51. Dass B, Soong HK, Lee B. Effects of proparacaine on actin cytoskeleton of corneal epithelium. J Ocul Pharmacol 1988;4:187–94. 52. Sivak JM, West-Mays JA, Yee A, et al. Transcription factors Pax6 and AP-2alpha interact to coordinate corneal epithelial repair by controlling expression of matrix metalloproteinase gelatinase B. Mol Cell Biol 2004;24:245–57. 53. Pflugfelder SC, Farley W, Luo L, et al. Matrix metalloproteinase-9 knockout confers resistance to corneal epithelial barrier disruption in experimental dry eye. Am J Pathol 2005;166:61–71. 54. Netto MV, Mohan RR, Ambrosio R Jr, et al. Wound healing in the cornea: a review of refractive surgery complications and new prospects for therapy. Cornea 2005;24:509–22. 55. Stramer BM, Zieske JD, Jung JC, et al. Molecular mechanisms controlling the fibrotic repair phenotype in cornea: implications for surgical outcomes. Invest Ophthalmol Vis Sci 2003;44:4237–46. 56. Wilson SE, He YG, Weng J, et al. Epithelial injury induces keratocyte apoptosis: hypothesized role for the interleukin-1 system in the modulation of corneal tissue organization and wound healing. Exp Eye Res 1996;62:325–7. 57. Mohan RR, Hutcheon AE, Choi R, et al. Apoptosis, necrosis, proliferation, and myofibroblast generation in the stroma following LASIK and PRK. Exp Eye Res 2003;76:71–87. 58. Erie JC, McLaren JW, Hodge DO, et al. Long-term corneal keratoctye deficits after photorefractive keratectomy and laser in situ keratomileusis. Trans Am Ophthalmol Soc 2005;103:56–66; discussion 67–8. 59. Konomi K, Zhu C, Harris D, et al. Comparison of the proliferative capacity of human corneal endothelial cells from the central and peripheral areas. Invest Ophthalmol Vis Sci 2005;46:4086–91.