IVMS Endocrine Part III-PATHOPHYSIOLOGY OF DIABETES MELLITUS
•
37 j'aime•7,662 vues

ENDOCRINE SYSTEM Part III-PATHOPHYSIOLOGY OF DIABETES MELLITUS

Recommandé
Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
En vedette (20)
Similaire à IVMS Endocrine Part III-PATHOPHYSIOLOGY OF DIABETES MELLITUS
Similaire à IVMS Endocrine Part III-PATHOPHYSIOLOGY OF DIABETES MELLITUS (20)
Plus de Imhotep Virtual Medical School
Plus de Imhotep Virtual Medical School (20)
Dernier
Dernier (20)
IVMS Endocrine Part III-PATHOPHYSIOLOGY OF DIABETES MELLITUS
- 1. ENDOCRINE SYSTEM Part III PATHOPHYSIOLOGY OF DIABETES MELLITUS Prepared and presented by: Marc Imhotep Cray, M.D. IVMS Endocrine Secretion and Action Part I Part II WebPath Pathology: Endocrine Pathology 70 Images Recommended Reading: Management of Diabetes Formative Assessment Practice question set #1 Clinical: E-Medicine Article Diabetes Mellitus, Type 2 – A Review 1
- 2. Pathophysiology of Diabetes Mellitus 2
- 4. Endocrine Pathology (Next 7 Slides) Islets of Langerhans Source: http://library.med.utah.edu/WebPath/ENDOHTML/ENDOIDX.html#6 1. Islets of Langerhans Islet of Langerhans, normal, microscopic 2. Islet of Langerhans, immunoperoxidase staining with antibody to insulin (on right) and glucagon (on left), microscopic 3. Islet of Langerhans, insulitis in type I diabetes mellitus, microscopic 4. Islet of Langerhans, amyloid deposition in type II diabetes mellitus, microscopic 5. Islet of Langerhans, islet cell adenoma, low power microscopic 6. Islet of Langerhans, islet cell adenoma, medium power microscopic 7. Islet of Langerhans, islet cell adenoma with immunoperoxidase staining with antibody to insulin, (insulinoma), microscopic 4
- 5. Islet of Langerhans, normal, microscopic Here is a normal pancreatic islet of Langerhans surrounded by normal exocrine pancreatic acinar tissue. The islets contain alpha cells secreting glucagon, beta cells secreting insulin, and delta cells secreting somatostatin. 5
- 6. Islet of Langerhans, immunoperoxidase staining with antibody to insulin (on right) and glucagon (on left), microscopic Immunoperoxidase staining can help identify the nature of the cells present in the islets of Langerhans. On the right, antibody to insulin has been employed to identify the beta cells. On the left, antibody to glucagon identifies the alpha cells. 6
- 7. Islet of Langerhans, insulitis in type I diabetes mellitus, microscopic This is an insulitis of an islet of Langerhans in a patient who will eventually develop type I diabetes mellitus. The presence of the lymphocytic infiltrates in this edematous islet suggests an autoimmune mechanism for this process. The destruction of the islets leads to an absolute lack of insulin that 7
- 8. Islet of Langerhans, amyloid deposition in type II diabetes mellitus, microscopic This islet of Langerhans demonstrates pink hyalinization (with deposition of amyloid) in many of the islet cells. This change is common in the islets of patients with type II diabetes mellitus. 8
- 9. Islet of Langerhans, islet cell adenoma, low power microscopic An islet cell adenoma is seen here, separated from the pancreas by a thin collagenous capsule. A few normal islets are seen in the pancreas at the right for comparison. 9
- 10. Islet of Langerhans, islet cell adenoma, medium power microscopic The islet cell adenoma at the left contrasts with the normal pancreas with islets at the right. Some of these adenomas function. Those that produce insulin may lead to hypoglycemia. Those that produce gastrin may lead to multiple gastric and duodenal ulcerations (Zollinger-Ellison syndrome). 10
- 11. Islet of Langerhans, islet cell adenoma with immunoperoxidase staining with antibody to insulin, (insulinoma), microscopic This is an immunohistochemical stain for insulin in the islet cell adenoma. Thus, it is an insulinoma. 11
- 12. Properties of IDDM* and NIDDM** Characteristic IDDM NIDDM Genetic locus Chromosome 6 unknown Usually < 40 years of Typical age of onset > 40 years of age age Plasma insulin Low to absent Normal to high Plasma glucagon High, suppressible High, resistant Acute complication Ketoacidosis Hyperosmolar coma Responsive to Insulin therapy Responsive resistant Response to Unresponsive Responsive sulfonylurea drugs * Insulin-dependent diabetes mellitus **Non-insulin dependent diabetes mellitus 12
- 13. Alpha cell stimulation "Inputs to alpha cells and effects of glucagon, including negative feedback, which increases plasma glucose levels" Robert H. Parsons, Ph.D., Rensselaer Polytechnic Institute 13
- 14. Beta cell stimulation "Inputs to beta cells and effects of insulin, including negative feedback on glucose and amino-acids levels. " Robert H. Parsons, Ph.D., Rensselaer Polytechnic Institute 14
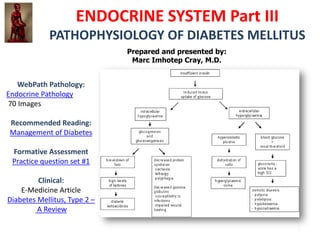
- 15. "Effects of Insulin deficiency" Robert H. Parsons, Ph.D., Rensselaer Polytechnic Institute 15
- 16. Diabetes Insipidis vs Diabetes Mellitus • Diabetes Insipidis – Due to disease of and/or damage to hypothalamus – Causes Antidiuretic Hormone (ADH) insufficiency • Water re-absorption in kidney is impaired • can lose up to 25 liters water/day • Diabetes Mellitus – Due to insufficient production of, or insensitivity to insulin eMedicine Articles – Diabetes Mellitus, Type 1 – Diabetes Mellitus, Type 2 – Diabetic Ketoacidosis 16
- 17. Ketogenesis Ketogenesis is the process by which ketone bodies are produced as a result of fatty acid breakdown. • ketone bodies are created at moderate levels in everyone's bodies, such as during sleep and other times when no carbohydrates are available. However, when ketogenesis is happening at higher than normal levels, the body is said to be in a state of ketosis. It is unknown whether ketosis has negative long-term effects or not. • Ketoacidosis occurs in IDDM, not NIDDM 17
- 18. Ketogenesis (See notes, next slide for RXN explanation) • Both acetoacetate and beta- hydroxybutyrate are acidic, and, if levels of these ketone bodies are too high, the pH of the blood drops, resulting in ketoacidosis. This is very rare, and, in general, happens only in untreated Type I diabetes (see diabetic ketoacidosis) and in alcoholics after binge drinking and subsequent starvation (see alcoholic ketoacidosis). 18
- 19. Ketogenesis The acetyl-CoA produced by mitochondrial beta-oxidation of fatty acids enters the Kreb's cycle to produce energy, but that is not the only fate of acetyl-CoA. In liver mitochondria, some acetyl-CoA is converted to acetoacetate, beta-hydroxybutyrate, and acetone, collectively called ketone bodies. Ketone bodies are transported to other tissues such as brain, muscle or heart where they are converted back to acetyl-CoA to serve as an energy source. The brain normally uses only glucose for energy, but during starvation ketone bodies can become the main energy source for the brain. In the metabolic condition called ketosis, ketone bodies are produced faster than they are consumed by tissues and the smell of acetone can be detected on a person's breath. The smell of acetone is one indication that a person may have diabetes. The consumption of high- fat/low carbohydrate diets has been used as a weight loss program by many, intentionally inducing ketosis to consume fat stores, but these ketogenic diets can cause unwanted side effects related to increased urea production resulting from protein intake and risk of heart disease from increased cholesterol and fat intake. 19
- 20. Pancreas: Endocrine Function • Endocrine functions – Produces hormones (insulin and glucagon) that are released into bloodstream – Islets of Langerhans = hormone-secreting cells • Beta () cells secrete insulin • Alpha () cells secrete glucagon 20
- 21. Absorptive State • Ingested nutrients – move from GI tract to bloodstream – some provide energy for body needs – some is stored • Glucose = major energy source • Principle hormone = Insulin – promotes glucose (nutrient) uptake and storage (as glycogen) 21
- 22. Post-Absorptive State • Mechanisms initiated to maintain blood glucose levels even without recent intake of food – Glycogenolysis – Gluconeogenesis – Glucose sparing (fat utilization) • Main energy source = fats • Main hormone = glucagon – promotes conversion of glycogen to glucose 22
- 23. Insulin • Produced & secreted as prohormone – 84 a.a. long – Beta chain-- connecting peptide-- alpha chain • After secretion prohormone cleaved to yield active hormone – Connecting peptide cut out – Active hormone formed by the two remaining chains (alpha and beta), held together by two -s-s- (disulfide) bonds 23
- 24. Insulin Actions • Lowers blood glucose levels – Moves glucose from bloodstream into cells • liver and brain = only cells capable of glucose uptake independent of insulin – Promotes muscle and liver conversion of glucose to glycogen • Lowers blood levels of free f.a. and a.a. – Promotes incorporation of free fatty acids into triglycerides – Promotes incorporation of amino acids into protein 24
- 25. Glucagon • Produced by cells of Islets of Langerhans • Single-chain polypeptide, 29 a.a. long A microscopic image stained for glucagon • Glucagon Action – Raises blood glucose levels – Promotes gluconeogenesis, glycogenolysis and triglyceride utilization, protein catabolism Rotating stereogram animation of glucagon. (1.70 MB, animated GIF format). 25
- 26. Diabetes Mellitus • Impaired carbohydrate (glucose) metabolism • Type I versus Type II – Type I (IDDM) • ‘juvenile onset’ • IDDM = Insulin-dependent diabetes mellitus – Type II (NIDDM) • ‘mature onset’ • NIDDM = Non insulin-dependent diabetes mellitus 26
- 27. Type I Diabetes Mellitus • Insulin-dependent diabetes Mellitus (IDDM) – Therapy requires administration of insulin • Less common form • Due to insulin insufficiency – Pancreas secretes little, if any, insulin – Pancreas secretes higher than normal levels of glucagon 27
- 28. Possible causes of diabetes 28
- 29. Insulin Influence on Glucagon Secretion • Insulin needed for alpha cells to sense blood glucose levels properly • When insulin levels are low, alpha cells cannot properly detect glucose in blood, respond as if glucose levels are low, even though glucose levels are very high in diabetic patient • Can cause over-secretion of glucagon 29
- 30. Type I DM (continued) • Some genetic predisposition – One twin afflicted; 50% predictive of disease in second twin • Environmental factors as important as genetic factors – viral infections may play a role • Most recent studies implicate autoimmune disease as underlying cause – Body’s white blood cells attack and destroy pancreas beta cells 30
- 31. Type II Diabetes Mellitus • Non insulin-dependent diabetes mellitus (NIDDM) • Most common form of DM(90%) • Pancreas secretes insulin – Insulin levels normal or high • Due to insulin insensitivity/insulin resistance – Altered receptor structure – Altered cellular responses after hormone activation 31
- 32. Type II DM (continued) • Disease mainly seen in overweight adults – Highly correlated to obesity – High fat diet may play role in insulin resistance • Often accompanied by beta cell defect in ability to secrete insulin in response to rise in plasma glucose • High genetic predisposition – Twin studies; one affected, 100% predictive of development in other twin 32
- 33. Type II DM Therapy • Therapy does not require insulin administration • Weight loss - eliminate obesity • Exercise – endurance exercise often increases insulin responsiveness • Dietary modification – low-fat diet to reduce insulin resistance • Sulfonylurea drugs can be administered to stimulate increased beta cell insulin production 33
- 34. Insulin and Glucagon Insulin Association of the British Pharmaceutical Industry • Insulin and glucagon have opposite effects on liver and other tissues for controlling blood-glucose levels 34
- 35. Blood Glucose and the Brain • Brain cannot synthesize, store, or concentrate glucose • Brain does not require insulin to take up glucose from bloodstream • Amount of glucose taken up in brain is directly proportional to amount of glucose in bloodstream 35
- 36. Primary Symptoms of Diabetes Mellitus • Glucosuria • Polyuria • Polydipsia • Polyphagia 36
- 37. Glucosuria • Glucosuria = glucose in the urine – glucose filtered blood in kidney – normally, all that is filtered in kidney is reabsorbed • high glucose levels in DM patients exceed kidneys capacity for reabsorption, so some glucose is lost in urine 37
- 38. Polyuria • Polyuria = production of large amounts of urine • Kidney is unable to reabsorb all the glucose, so some is lost in urine – large amounts of water eliminated (urine formed) as glucose is removed from blood 38
- 39. Polydipsia • Polydipsia = increased intake of liquids • Large amount of water lost in urine causes profound thirst – DM patient ingests large amounts of water to quench thirst 39
- 40. Polyphagia • Polyphagia = excessive food intake • Body’s inability to utilize glucose results in inadequate nutrient/energy for body tissues • Increased ingestion of foods to compensate, not accompanied by weigh gain 40
- 41. Weight Loss • Although food intake is increased, it is not accompanied by weight gain – body is unable to use carbohydrates ingested • Body breaks down fats and proteins to use as fuel/nutrient supplies – fatty acids and amino acids used in Kreb’s cycle to generate energy – glycerol and some amino acids can be converted to glucose 41
- 42. Ketosis • Ketones = fatty acid metabolites – made principally in liver, from acetyl CoA – acetone, acetoacetate, b-hydroxybutyrate – brain and other tissues can metabolize them via Kreb’s cycle as energy source • Ketones accumulate in blood, build up faster than they’re used or eliminated • Ketones volatile, in liquid phase, rapidly move to gaseous phase – give diabetic’s breath a fruity odor 42
- 43. Ketosis (continued) • Ketones increase hydrogen-ion concentration in blood; cause acidosis = ketosis, ketoacidosis • Ketoacidosis occurs in IDDM, not NIDDM • Can result in diabetic coma and death 43
- 44. Diabetic Coma • Results from untreated/ out-of-control diabetes • Blood glucose and ketone levels very high • Fruity breath • Symptoms: difficulty breathing, nausea, vomitting, flushing of skin, dehydration, electrolyte imbalance • Treatment: – insulin administration to reduce blood glucose – fluid and electrolyte administration 44
- 45. High blood Glucose in Diabetes • The high blood glucose in diabetes produces glucose in the urine and frequent urination through effects on the kidneys 45
- 46. Lack of insulin or insulin resistance • The lack of insulin or insulin resistance acts on many organs to produce a variety of effects. 46
- 47. Complications of DM 47
- 48. Complications of DM • Cardiovascular – atherosclerosis &/or damage to small vessels • heart attack • stroke • poor perfusion of extremities; poor wound healing – gangrene causes need for limb amputations • Renal complications – renal damage leads to kidney failure 48
- 49. Complications (continued) • Nervous system complications – nerve damage • peripheral neuropathy; loss of sensation in extremeties • evident in genitals; impotence in men, loss of sensation in women • Vision complications – damage to retina as small vessels rupture – produces blindness 49
- 50. Complications (continued) • Many, if not all, complications related to high blood glucose levels – accumulation of high concentrations of glucose metabolites (sorbitol) in cells associated with cell damage • May be related to high glucagon levels and altered metabolic activity • Diabetics die most often from complications, rather than from diabetes itself (i.e. insulin shock or diabetic coma) 50
- 51. Insulin Shock • Caused by too much insulin for the amount of glucose present in bloodstream – administer too much – body’s demand for glucose not matched to insulin levels – body’s dietary intake not matched to insulin levels • Symptoms: confusion, personality changes, profuse sweating, unconciousness • Treatment: raise blood glucose levels 51
- 52. REMEMBER Glycosylated Hemoglobin • Formed by addition of glucose to nml Hgb molecules • Formed in larger amounts in diabetics under poor glycemic control because they have high levels of glucose in bloodstream • Molecule is very stable so once formed does not readily break down (RBC lifespan is 120 days) – This makes it a good indicator of long term glycemic control – Measuring normal blood glucose is a better indicator of immediate glucose control 52
- 53. Animations and Tutorials • Glucose Homeostasis Gerard Scholte & Ineke Marree • Glucose Metabolism for the Endocrine System Wisconsin Online • Insulin Association of the British Pharmaceutical Industry 53
- 54. Q&A • Q#: I : The features characteristic of non-insulin dependent diabetes mellitus include which of the following? • A. Age of onset is below forty years • B. Insulin level is often decreased • C. Responds to an oral hypoglycernic agent (sulfonylurea) • D. Genetic locus is present in chromosome 6 • E. Prone to develop diabetes ketoacidosis 54
- 55. Q&A • Q#: 2 : Diabetes mellitus is divided into three categories based on etiology. Which disease occurs most commonly in those individuals who are less than 40 years of age and what is the cause? • A. Gestational diabetes and high serum insulin • B. Insulin-dependent and high blood glucose • C. Gestational diabetes and low serum insulin • D. Non-insulin dependent and low blood glucose 55
- 56. Q&A • Q#: 3 : The main cause of acidosis in the untreated diabetic patient is • A. Elevated blood levels of ketone bodies • B. Consumption of a high protein diet • C. Excess production of bicarbonate • D. Elevated levels of insulin are present • E. Decreased blood levels of ketone bodies 56
- 57. Q&A • Q#: 4 : In which of the following childhood diseases does ketone bodies reach dangerous levels in untreated cases? • A. Diabetes mellitus • B. OTCD • C. Phenylketonuria • D. Von Gierke's disease • E. Medium chain acyl-CoA dehydrogenase deficiency 57
- 58. Q&A • Q#: 5 : For which of the following diseases would you perform the urine test, Glucose? • A. Cushing syndrome • B. 11 -hydroxylase deficiency • C. Diabetes mellitus • D. Pheochromocytorna • E. Diabetes insipidus 58
- 59. Q&A • Q#: 6 : Which of the following statements about the epidemiology of diabetes is true? • A. Women are at higher risk of developing insulin dependent diabetes mellitus than men • B. Almost half of all diabetics develop nephropathy during the course of their illness • C. Of diabetics in the U.S., approximately 75% have insulin dependent diabetes mellitus • D. The majority of people with non-insulin dependent diabetes mellitus are obese • E. Blacks have a higher incidence rate of insulin dependent diabetes mellitus than whites 59
- 60. Q&A • Q#: 7 : In individuals with untreated diabetes mellitus, there is a shift in fuel usage from • A. Fats to carbohydrates • B. Fats to ketone bodies • C. No change occurs • D. Ketone bodies to carbohydrates • E. Carbohydrates to fats 60
- 61. Q&A • Q#: 8 : Elevated levels of hemoglobin A1c in the blood could be an indication of • A. Gout • B. Sickle cell anemia • C. Thalassemia • D. Hypertension • E. Diabetes mellitus 61
- 62. Q&A • Q#: 9 : Which one of the following is a characteristic of Type II diabetes mellitus? • A. Rare occurrence • B. Increased insulin resistance caused by decrease in the number of cell receptor sites • C. Strong association with HLA-DR3 and HLA-DR4 • D. Usual occurrence in underweight or normal adults • E. Peak onset at age 11 to 13 62
- 63. End of Session Services provided by Imhotep Virtual Medical School Individualized Webcam facilitated USMLE Step 1 Tutorials with Dr. Cray Starting at $50.00/hr., depending on pre-assessment. 1 BMS Unit is 4 hr. General Principles and some Organ System require multiple units to complete in preparation for the USMLE Step 1 A HIGH YIELD FOCUS in Biochemistry / Cell Biology, Microbiology / Immunology, the 4 P’s-Physiology, Pathophys., Path and Pharm and Intro to Clinical Medicine Webcam Facilitated USMLE Step 2 Clinical Knowledge and Clinical Skills didactic tutorials starting at $75.00 per hour /1 Unit is 4 hours, individualized one-on-one and group sessions, Including Introduction to Clinical Medicine and all Internal Medicine sub-specialities at the clerkship level. For questions or more information. drcray@imhotepvirtualmedsch.com ALL e-books and learning tools provided 63