
Recommandé
Contenu connexe
Tendances
Tendances (20)
Similaire à 2. Sinuses Pathology 21-22 (1).pdf
Similaire à 2. Sinuses Pathology 21-22 (1).pdf (20)
Dernier
Dernier (20)
2. Sinuses Pathology 21-22 (1).pdf
- 1. ParanasalSinuses Pathology. Lecture 2 Dr. Moiseeva Aleksandra Anatol’evna 1
- 2. Paranasal sinuses pathology • Sinusitis - Acute sinusitis - Chronic sinusitis - Chronic sinusitis with polyps
- 3. Thesinusesare: • Cavities, or air- fi lled pockets, near the nasal passages • Lined with mucous membrane continuous with that of nasal cavity • All communicate with nasal fossa through their various ostia • 3
- 4. Thesinusesare: • Cavities, or air- fi lled pockets, near the nasal passages • Lined with mucous membrane continuous with that of nasal cavity • All communicate with nasal fossa through their various ostia • 4 How many types of PNS can you name?
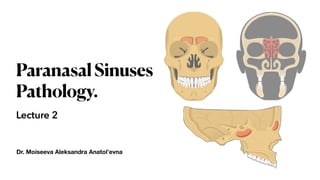
- 5. Typesofsinuses: • Ethmoid sinus. This sinus is located inside the face, around the area of the bridge of the nose. • Maxillary sinus. This sinus is located inside the face, around the area of the cheeks. • Frontal sinus. This sinus is located inside the face, in the area of the forehead. • Sphenoid sinus. This sinus is located deep in the face, behind the nose. 5
- 6. Typesofsinuses: • Ethmoid sinus. This sinus is located inside the face, around the area of the bridge of the nose. • Maxillary sinus. This sinus is located inside the face, around the area of the cheeks. • Frontal sinus. This sinus is located inside the face, in the area of the forehead. • Sphenoid sinus. This sinus is located deep in the face, behind the nose. 6 Which sinuses are present at birth?
- 7. Typesofsinuses: • Ethmoid sinus. This sinus is located inside the face, around the area of the bridge of the nose. It is present at birth, and continues to grow. • Maxillary sinus. This sinus is located inside the face, around the area of the cheeks. It is also present at birth, and continues to grow. • Frontal sinus. This sinus is located inside the face, in the area of the forehead. It does not develop until around 7 years of age. • Sphenoid sinus. This sinus is located deep in the face, behind the nose. It does not typically develop until adolescence. 7
- 8. Accordingtothe damagedsinus patientswillcomplain onpaininspeci f icarea: • Ethmoid sinus. This sinus is located inside the face, around the area of the bridge of the nose. It is present at birth, and continues to grow. • Maxillary sinus. This sinus is located inside the face, around the area of the cheeks. It is also present at birth, and continues to grow. • Frontal sinus. This sinus is located inside the face, in the area of the forehead. It does not develop until around 7 years of age. • Sphenoid sinus. This sinus is located deep in the face, behind the nose. It does not typically develop until adolescence. 8
- 9. Thesinusesare: • Cavities, or air- fi lled pockets, near the nasal passages • Lined with mucous membrane continuous with that of nasal cavity • All communicate with nasal fossa through their various ostia • The sinuses are divided for Clinical Purposes into two groups: - Anterior - Posterior • The line of attachment of middle turbinate to lateral wall of nose marks division between the two. 9
- 10. Groupsofsinuses 10 The Posterior Group draining at several locations above the middle turbinate is made up of: - Posterior Ethmoidal Cells - Sphenoidal Sinuses The Anterior Group draining below the middle turbinate or near the infundibulum and consists of: - Frontal - Maxillary - Anterior and Middle Group of Ethmoidal cells
- 11. Wheredothedischargego • All the PNS are draining into nasal cavity by speci fi c nasal meatus (passage) • Anterior group of sinuses -> middle meatus • Posterior group of sinuses -> superior meatus • The nasolacrimal duct is draining to the inferior meatus
- 13. Functionsofthesinuses • Give resonance to voice • Sound protection from transmission of one’s own speech to the ears • May have a role in air-conditioning of the inspired air • May reduce skull weight • Provide protection to orbits • An hitherto unexplained function of the PNS may be the supply of the fresh, uncontaminated mucus to the middle meatus. 13
- 14. Nasolacrimal duct – acts to drain tears from the eye. It opens into the inferior meatus. 14 Inadditiontotheparanasalsinuses, otherstructuresopeninto thenasalcavity:
- 15. Auditory (Eustachian) tube – opens into the nasopharynx at the level of the inferior meatus. It allows the middle ear to equalise with the atmospheric air pressure.
- 16. Paranasal sinuses pathology • Sinusitis - Acute sinusitis - Chronic sinusitis - Chronic sinusitis with polyps
- 17. Whatissinusitis? Sinusitis is an in fl ammation of the mucosa of one or several paranasal sinuses. The in fl ammation may be • suppurative or non-suppurative; • acute or chronic; • with or without polyps. 17
- 18. 1) Acute – duration of symptoms lasts up to 12 weeks, including 4-12 weeks of subacute 2) Recurrent acute – 2-4 acute cases of sinusitis per year 3) Chronic – symptoms lasts over 12 weeks 1. Monosinusitis – one sinus is damaged: Maxillary sinusitis, frontitis, ethmoiditis, sphenoiditis 2. Polysinusitis (more than 1 sinus are damaged), Hemisinusitis (sinuses of one side are damaged), Pansinusitis (all sinuses are damaged) Duration Localisation 18 Classi f ication
- 19. Local predisposing factors • Upper respiratory tract infection (acute infective rhinitis, tonsillitis or adenoiditis) • Pre-existing rhinitis (allergic, vasomotor, rhinitis medicamentosa, etc) • Nasal polyps • Nasal foreign body • Nasal anatomical variations (septal deviation, abnormal uncinate process, middle turbinate or ethmoid bulla) which narrow the infundibulum and predispose to its occlusion when there is intercurrent disease • Nasal tumour • Dental extraction or infection (diseases of the upper premolars and molars) • Fractures involving the sinuses 19
- 20. • Debilitation • Immunocompromise patients • Mucociliary disorders (e.g. Kartagener’s syndrome, cystic fi brosis) • Atmospheric irritants(dust, fumes, tobacco smoking) 20 General predisposing factors
- 21. – is de fi ned as the sudden onset of two or more symptoms, one of which is nasal congestion/di ffi culty in nasal breathing or discharge from the nose (out, into the nasopharynx) ± pain / pressure in the face, ± decrease or loss of smell. Symptoms persist for <12 weeks. The latest series of guidelines on rhinosinusitis from an international cohort of experts 21 Acutesinusitis
- 22. Pathology The majority of cases follow a viral upper respiratory tract infection which involves all of the respiratory epithelium including the paranasal sinuses. Such infections cause hyperaemia and oedema of the mucosa, which blocks the ostia. There will be cellular in fi ltration and an increase in mucus production. The infection will also paralyse the cilia, leading to stasis of secretions predisposing to secondary bacterial infection. The usual causative organisms are Streptococcus pneumoniae, Haemophilus in fl uenzae (pneumococcal and haemophilus infections accounting for 70% of cases in adults), Streptococcus pyogenes, Moraxella catarrhalis, and Staphylococcus aureus. Klebsiella pneumoniae, Escherichia coli and Streptococcus faecalis may spread from a dental source. Acute fungal infections (for example mucormycosis and aspergillosis) are rare, but may develop in immunocompromised or elderly diabetic patients. 22
- 24. - pain over the infected sinus - nasal congestion - fullness in the face - malaise and possibly a pyrexia The symptoms usually occur several days after developing an upper respiratory tract infection. Speci fi c features may indicate the sinus that is infected. Complaints 24
- 25. Maxillary sinus – pain developing in the cheek or upper teeth Frontal sinusitis – pain in the forehead and tenderness below the eyebrows Ethmoid sinusitis – pain between the eyes accompanied by frontal headache Sphenoid sinus – pain anywhere across the vault or retro- orbital pain Speci f icfeatures 25
- 26. Diagnostic • red oedematous nasal mucosa and turbinates • pus in the middle meatus 26 • X-ray of paranasal sinuses is needed only if there is a clinic of complications, it is better to make CT • Also could be needed in di ffi cult cases for a di ff erential diagnosis • In some cases – bacteriological examination of the discharge (puncture and selection of antibioticterial treatment) Anterior rhinoscopy: Any other diagnostic needed?
- 27. Diagnosis: Example of diagnosis • Ill for 11 days, beginning with light nasal discharge • Now there’s a temperature up to 37oC • By anterior rhinoscopy – hyperaemia of nasal mucosa, white discharge in the left part of the nose coming throw the middle nasal passage • Pain in the left cheek 27
- 28. Diagnosis: Acuteleft-sidedmaxillarysinusitis Example of diagnosis • Ill for 11 days, beginning with light nasal discharge • Now there’s a temperature up to 37oC • By anterior rhinoscopy – hyperaemia of nasal mucosa, white discharge in the left part of the nose coming throw the middle nasal passage • Pain in the left cheek 28
- 29. Treatment ofacutesinusitis • Only catarrhal changes – treating as acute rhinitis • 29
- 30. Treatment ofacutesinusitis • Only catarrhal changes – treating as acute rhinitis • Acute bacterial sinusitis: - antibacterial treatment - washing the nasal cavity according to Proetz - topical decongestants – up to 3-5 days - topical corticosteroids (see Lecture 1) + mucolytics (see Lecture 1) - puncture of maxillary sinus – better to be done after CT for out fl ow of pus 30
- 31. Antibacterialtreatmentofacutesinusitis Major bacterial pathogens Drugs of the 1 step Drugs of the 2 step Drugs of the 3 step Duration of therapy S. Pneumoniae H. In fl uenzae b-hem streptococci (not A) M. Catarrhalis Doc. of GM (mild and uncomplicated forms): Amoxicillin per os 0,5 3 times a day or 1,0 2 times a day ENT (moderate and complicated forms): Amoxicillin/Сlavulanate per os 0,625 3 times a day or 1,0 2 times a day Ce fi xim per os 0,4 ones a day Cefditoren per os 0,2 twice a day Josamicin per os 1,0 twice a day Clarithromycin per os 0,5 twice a day Levo fl oxacin per os 0,75 once a day Moxi fl oxacin per os 0,4 once a day 5-7 days 31
- 32. WashingthenasalcavityaccordingtoProetz 32 The washing of the sinuses is popularly called the «cuckoo». This term was chosen for a reason, since during the procedure the patient is asked to repeat “cuckoo-cuckoo” all the time to provide protection of respiratory tract from the ingress of liquid, since during the pronunciation of these sounds a soft palate rises and thereby closes the nasopharynx, the epiglottis also blocks the entrance to the larynx.
- 33. WashingthenasalcavityaccordingtoProetz • The patient is o ff ered to lie on his back (sitting position is acceptable). He/she needs to breathe smoothly and calmly. • The next step is the anemization of the mucosa (using vasoconstrictive drops) • The doctor heats the solution, with the help of which the Proetz method will be carried out (saline solutions, NaCl 0,9% or solutions with antibiotics or corticosteroids) 33
- 34. WashingthenasalcavityaccordingtoProetz • The otolaryngologist pours the prepared solution into one nostril, and using a special vacuum apparatus sucks it from the other half of the nose. • Under the in fl uence of vacuum, negative pressure is created, which helps to clear the sinuses from pathological contents. • «Cuckoo» sound during such washing can be carried out up to 5 times in 10 minutes. 34
- 35. Maxillarysinuspuncture(Antralwashout) • The maxillary sinus is irrigated with 0,9% NaCl solution by a cannula introduced through the inferior meatus. • The solution circulates inside the sinus cavity and comes out together with accumulated discharge through the natural ostium in the middle meatus. • Before procedure – anemisation with decongestant; anaesthesia (lidokain) 35
- 36. • Is a chronic in fl ammation of the mucous membrane which has resulted in irreversible and usually degenerative changes. • Symptoms persist for >12 weeks. - odontogenic – treating by dentist - associated with systemic diseases - associated with tumor process - chronic atelectasis of the maxillary sinus Speci fi c forms: 36 Chronicsinusitis
- 37. Signs • persistent nasal discharge • di ffi culty in nasal breathing • headache or pain in the projection of the sinuses • postnasal syndrome (a feeling of constant fl ow of viscous secretions along the back wall of the nasopharynx) •Examination, palpation and percussion, anterior rhinoscopy •Assessment of clinical manifestations, anamnesis and complaints •CT of paranasal sinuses – not at exacerbation! •Results of laboratory studies 37 Diagnostic
- 38. Treatment • Antibacterial treatment • Intranasal corticosteroids during ~ 3 months • Irrigation therapy (according to Proetz) • Mucolytics • Surgical treatment: puncture and revision of paranasal sinuses Endoscopic view of the removal of the left posterior maxillary bone and polypoid tissue with through-cut forceps. 38
- 39. Antibacterial treatment of exacerbation of chronic sinusitis Major bacterial pathogens Drugs of the 1step Drugs of the 2 step Drugs of the 3 step Duration of therapy Polyetiologic: S. Pnemoniae H. In fl uenzae Staphylococcus aureus, Enterobacteria etd, + Anaerobes Amoxicillin/ Сlavulanate per os 0,625 3 times a day or 1,0 twice a day Ce fi ximum per os 0,4 ones a day Levo fl oxacin per os 0,75 once a day Moxi fl oxacin per os 0,4 once a day 10-14 days 39
- 40. Patients usually present with: • nasal obstruction • persistent nasal discharge (rhinorrhea) • sinus infection • loss of the sense of smell (anosmia) of prolonged duration Polyp formation in the nasal cavity is due to chronic allergic rhinitis, chronic sinusitis, and, less commonly, underlying disease such as cystic fi brosis. Often combined with bronchial asthma. 40 Chronicsinusitiswithpolyps
- 41. 41
- 42. Tactics • The presence of obstruction – polypectomy • The presence of changes in the mucous membrane and deformation of the intranasal structures – conservative therapy and surgical treatment of anatomical anomalies • The presence of anatomical changes and diagnosed bronchial asthma – combined treatment of an ENT specialist and an allergist 42
- 43. 43