A hernia happens when an organ or maybe fatty tissue squeezes through a weak
spot in a surrounding muscle or connective tissue called fascia.
Hernias were
once the leading cause of acute intestinal obstruction.
Public alertness of early
repair has markedly reduced the frequency of incarceration of intestine in these
musculofascial defects.
The common sites for these defects, in order of frequency,
are inguinal, umbilical, incisional and femoral. Techniques of repair continue to
evolve but tension-free, mesh repairs are the current standard.
You may have a hernia if you can feel a soft lump in your belly or groin or in a
scar where you had surgery in the past. The lump may go away when you press on
it or lie down. It may be painful, especially when you cough, bend over, or lift
something heavy.
Call Girls Hosur Just Call 9630942363 Top Class Call Girl Service Available
Hernia 2018
1. 2/28/2018
‘Hernia and its types’
‘University of Baghdad College of medicine’
SSC- HSF -module
Samer Adnan mohsin
2nd stage
B1
2. 1 ‘Hernia and its types’
‘Introduction’
What is a hernia?
A hernia happens when an organ or maybe fatty tissue squeezes through a weak
spot in a surrounding muscle or connective tissue called fascia.1
Hernias were
once the leading cause of acute intestinal obstruction.2
Public alertness of early
repair has markedly reduced the frequency of incarceration of intestine in these
musculofascial defects.3
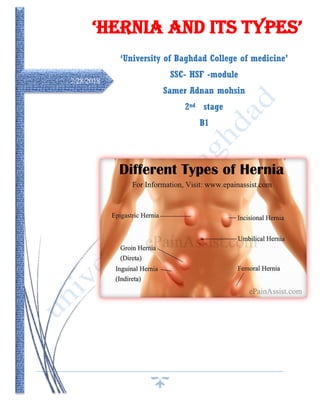
The common sites for these defects, in order of frequency,
are inguinal, umbilical, incisional and femoral. Techniques of repair continue to
evolve but tension-free, mesh repairs are the current standard.4
You may have a hernia if you can feel a soft lump in your belly or groin or in a
scar where you had surgery in the past. The lump may go away when you press on
it or lie down. It may be painful, especially when you cough, bend over, or lift
something heavy.5
What Causes Hernias?
Ultimately, all hernias are caused by a mixture of pressure and an opening or
weakness of muscle or fascia; the pressure squeezes an organ or tissue through the
opening or weak spot.6
Sometimes the muscle weakness is present at birth; more
often, it occurs later in life.
Anything that effects rise in pressure in the abdomen can cause a hernia,
including7
:-
Lifting heavy objects without stabilizing the abdominal muscles
Diarrhea or constipation
Persistent coughing or sneezing
In addition, obesity, poor nutrition, and smoking, can all weaken muscles and
make hernias more likely.8
Complications of abdominal wall hernias:
a. Incarceration
Incarceration means the limitation of a herniated structure in its protruded position.
Incarceration commonly occurs when the neck of the defect is small and rigid,
allowing entrance of the hernial sac and its contents but inhibits reduction.9
Once
incarceration has occurred, strangulation may quickly intervene leading to a
3. 2 ‘Hernia and its types’
surgical emergency.10
If bowel [usually small bowel] is contained in the hernia
then symptoms of obstruction will eventually occur. Incarceration in external
hernias is the number one cause of small bowel obstruction in patients who have
not undergone previous abdominal/pelvic surgery.11
Always look carefully for
incarcerated hernia in a patient with bowel obstruction when there has been no
prior abdominal surgery; this may require invagination of the scrotum into the
external ring or careful, deep palpation medial to the femoral vessels in obese
individuals.12
b. Strangulation
Once pressure at the neck of the hernial defects exceeds venous outflow pressure,
the hernia quickly becomes bloated with blood.13
The elevated pressure quickly
obstructs arterial flow leading to ischemia and subsequent edema and necrosis of
tissue.14
Approximately one quarter of strangulated hernias contain only omentum,
but the other 75% contain tissue which settlements bowel circulation. 15
Prolonged
strangulation of a hernia quickly raises mortality rates due to peritonitis and
sepsis.16
Frequency 17
Figure 1 epidemiology of hernia
Groin 75-85 %
-Indirect inguinal 60-65 %
-Direct inguinal 15 %
-Femoral 5 %
85%
10%
10%
5%
Sales
groin
incisional
ventral
others
4. 3 ‘Hernia and its types’
Incisional 10 %.
Ventral 10 %
- Epigastric
- Umbilical
Others 5 %
- Hiatal, Lumbar, spigelian, Sciatic
Types of hernias include: 18
1. Inguinal Hernia
2. Femoral Hernia
3. Umbilical Hernia
4. Incisional and parastomal Hernias
5. Epicastric Hernia
6. Hiatal Hernia
7. Spigelian Hernia
8. Obturator Hernia
9. Sciatic Hernia
10.Lumbar Hernia
1) Inguinal Hernia
An inguinal hernia is a condition in which intra-
abdominal fat or part of the small intestine, also
called the small bowel, bulges through a weak area
in the lower abdominal muscles.19
An inguinal
hernia occurs in the groin [the area between the
abdomen and thigh]. This type of hernia is called
inguinal because fat or part of the intestine slides
through a weak area at the inguinal ring, the
opening to the inguinal canal.20
An inguinal hernia appears as a bulge on one or
both sides of the groin. And can occur any time
from infancy to adulthood and is much more
common in males than females. It’s tend to become larger with time.21
There are two types of inguinal hernia have different causes:
Figure 2 position of inguinal hernia
5. 4 ‘Hernia and its types’
Indirect inguinal hernia: Indirect inguinal hernias are congenital hernias and
are much more common in males than females because of the way males develop
in the womb.22
In a male fetus, the spermatic cord and both testicles [starting from
an intra-abdominal location] normally descend through the inguinal canal into the
scrotum, the sac that holds the testicles. Sometimes the entrance of the inguinal
canal at the inguinal ring does not close as it should just after birth, leaving a
softness in the abdominal wall.23
Fat or part of the small intestine slides through
the weakness into the inguinal canal, causing a hernia. In females, an indirect
inguinal hernia is caused by the female organs or the small intestine sliding into the
groin through a weakness in the abdominal wall.24
Indirect hernias are the most
common type of inguinal hernia. Premature infants are especially at risk for
indirect inguinal hernias because there is less time for the inguinal canal to close.25
Direct inguinal hernia: Direct inguinal hernias are caused by connective
tissue degeneration of the abdominal muscles, which causes weakening of the
muscles during the adult years.26
Direct inguinal hernias occur only in males.27
The
hernia involves fat or the small intestine sliding through the weak muscles into the
groin. A direct hernia develops gradually because of continuous stress on the
muscles. One or more of the following factors can cause pressure on the abdominal
muscles and may worsen the hernia: 28
• Sudden twists, pulls, or muscle strains
• lifting heavy objects
• straining on the toilet
because of constipation
• Weight gain
• Chronic coughing
Indirect and direct
inguinal hernias usually
slide back and forth
spontaneously through the
inguinal canal and can
often be moved back into
the abdomen with gentle
massage.29
6. 5 ‘Hernia and its types’
2) Femoral Hernia
Femoral hernia is much like a direct inguinal hernia and is an unusual hernia in the
pediatric age group. A femoral hernia presents as a mass located lateral to and
below the pubic tubercle, inferior and posterior to the inguinal ligament and medial
to the femoral pulse.30
It occurs in about 0.5% of all groin hernias in children. The
diagnosis of a femoral hernia is challenging, and the correct preoperative diagnosis
is usually not made in many children. Most often, it is misdiagnosed, and only
during surgery for a suspected inguinal hernia is the specific diagnosis made.31
Note that a diagnosis of a missed femoral hernia or a direct inguinal hernia should
be considered if any child returns with an early recurrence of a groin bulge after an
adequate herniotomy, as recurrent indirect inguinal hernias are rare.32
Some
femoral hernias are reported to have occurred after an inguinal canal exploration or
even as a result of disruption of the femoral canal. Femoral hernias are high risk
for intestinal strangulation. The margins of a femoral hernia, inguinal, lacunar and
Cooper's ligament are rigid and unforgiving.33
In this case necrosis has developed at
the point of pressure at the hernia neck, after release of the hernia, intestinal
contents are already seen flowing into the distal bowel. A limited intestinal
resection was possible through the groin incision.34
The etiology of femoral
hernias remains indefinable. It is suggested that it may be due to either35
:
(1) A congenital narrow posterior inguinal wall attachment to Cooper’s ligament
with a resulting enlarged femoral ring (this is the anatomic aspect accepted by
many pediatric surgeons)
(2) An acquired genesis related to increased intra-abdominal pressure
The Incidence of Inguinal and Femoral
Hernias: 36
Direct Indirect Femoral
Men 40% 50% 10%
Female rare 70% 30%
Children rare All rare
Figure 3 position of femoral hernia
7. 6 ‘Hernia and its types’
Repair of inguinal and femoral hernias:
Elective repair of hernias has greatly reduced complications related to abdominal defects
(bowel obstruction, incarceration and strangulation). Almost all hernias should be
repaired.37
Discretion is used if the defect is small and the hernia easily reducible or the
patient is an appreciable risk for operative complication. Repairs of the inguinal hernias fall
into 4 groups: facial repairs (Bassini, Bassini with Tanner’s slide, McVay, Ferguson),
tension-free prosthetic repairs, laparoscopic (TAP) and percutaneous endoscopic external
ring repair (PEER).38
Fascial repairs carry a much higher risk of recurrence but have a decreased risk of infection.
Infection in the tension-free mesh techniques is rare in practice. Due the low recurrence
rates and low infection rates, this technique has taken favor by the majority of hernia
surgeons. Open tension-free method also allows for local anesthesia and patient is handled
as a day case.39
3) Umbilical Hernias
Umbilical hernias occurs when a small defect, caused by incomplete closure of the
umbilicus, allows intra-abdominal contents to protrude through the abdominal wall. The
defect may be insignificant during youth, only to weaken and stretch with age allowing for
the development of a hernia. 40
Incidence of Umbilical Hernias:
Umbilical hernias are congenital in origin and
often occur during infancy; spontaneous
closure by the age of 2 years is common.
In North America the incidence of umbilical
hernia in black infants is 8 times higher than
in white infants. Most umbilical hernias that
appear before the age of 6 months disappear
spontaneously by 1 year of age. Even large
hernias (5-6 cm in all dimensions) have been
known to disappear spontaneously by 5-6
years of age.41
4) Incisional and Parastomal Hernias
Figure 4 position of umbilical hernia
8. 7 ‘Hernia and its types’
Incisional and parastomal hernias are the protrusion of intra-abdominal contents through a
surgically formed defect. Incisional hernias are a huge problem, eventually developing in 5-
10% of patients where access to the abdomen was gained through a long midline incision.42
Often there is a readily identifiable contributing factor; in many instances, the wound
appears to heal only to become weaker over a period of months, with reduction of the
fascial layer and finally formation of a complete defect.
Initially, the defect may be oval shaped, in line with the
incision, but eventually will be circular; skin over the
peritoneum will become progressively more
attenuated.43
Fortunately, incisional hernias are usually diffuse bulges
that are unlikely to result in strangulation. Small defects
with rigid margins have the potential to cause
strangulation. Apart from the clear cosmetic scar,
incisional hernias cause pain, pulling, dragging and
heavy sensations often preventing return to work. For some people, with physically
demanding occupations, this can be permanent. 44
Repair of incisional hernias:
Many patients dislike the cosmetic effects of incisional hernias, and in combination with
pain insist on repair. 3 techniques are utilized to close an incisional hernia; primary facial
repair, tension-free repair by synthetic mesh prosthesis and autogenously repair by
vascularized innervated muscle flaps (usually used for large/recurrent defects). 45
a. Primary fascial repair
Due to extremely high reoccurrence rates, up to 50%, the primary fascial repair has been
uncontrolled and replaced by the tension-free repair. 46
b. Tension-free repair by synthetic mesh prosthesis
Reoccurrence rates with this technique are much more acceptable (2-10) %. A
polypropylene mesh (mono or double filament forms) or fluorinated polyester mesh (gel
impregnated with antibiotics) is sub-laid in the defect with generous overlap of the wound
margin and sutured into place. Risks of the tension-free repair of incisional hernias include
wound infection, infection of the mesh, seroma formation, wound sinuses, enterocutaneous
fistula formation, and recurrence. 47
5) Epicastric hernia
Figure 5 position of incisional hernia
9. 8 ‘Hernia and its types’
A hernia is a hole through a weakness in the abdominal wall. At the start of trouble you may
notice a lump or bulge appearing anywhere in the central, upper abdomen between the
breastbone and the tummy button. This area is known as the ‘epigastrium’, hence the term
‘Epigastric Hernia’. 48
The bulge consists most usually only of fatty tissue but when large
can contain gut. You may experience discomfort at first but it may become more painful
when lifting heavy objects or coughing. This hernia should not be confused with a large
bulge running from the breastbone to the navel which can sometimes occur as a result of
putting on weight and surgery is seldom
recommended.49
6) Hiatal hernia
Hiatal hernia is one of the different types of
hernia in which a part of your stomach impulses
upward across your diaphragm. There is a small
opening (hiatus) in your diaphragm through
which the food pipe that is the esophagus passes on its way to attach to the abdomen.50
This
hiatal hernia is the type of hernia that can be instigated when the abdomen pushes up
through this opening. Most of the time there is no problems caused because of small hiatal
hernia. One may know about it only when doctor gets to come across while diagnosing for
some other issue.51
A larger hiatal hernia can cause a bit of difficulty
as this hiatal hernia allows food and acid to back
up in your food pipe that will lead to heartburn.
Prevention and measures with proper medication
can relieve these problems, but a large hiatal
hernia can require operation.
Small hiatal hernia does not have any signs or
symptoms whereas larger hiatal hernia can cause
signs and symptoms which are as follows:52
Belching is a sign of hiatal hernia,
Feeling too full after regular meal,
Heartburn,
Difficulty in swallowing,
Figure 6 position of epicastric hernia
Figure 7 position of hiatal hernia
10. 9 ‘Hernia and its types’
Chest or stomach pain,
Vomiting blood or passing black stools indicating gastrointestinal bleeding is a major
symptom of hiatal hernia.
7) Spigelian hernia
Spigelian hernias occur when the abdominal contents protrude through a defect at the
semilunar line. The semilunar line is found on the lateral boarder of the rectus abdominals
muscle where it intersects the semicircular line of Douglas. 53
8) Obturator hernia
This rare hernia occurs mainly in elderly females. Abdominal contents protrude through a
weakened pelvic floor in the obturator canal. Patients will present with symptoms of
intermittent bowel obstruction and anteriomedial thigh paresthesias due to compression of
the obturator nerve coursing the superior aspect of the obturator canal. 54
9) Sciatic hernia
The greater sciatic foramen can also be the site of a relatively uncommon hernia. Diagnosis
can be difficult. Patients often present with pain on standing and diagnosis is often made
once bowel obstruction intervenes. Of note, a sciatic hernia rarely causes sciatic nerve pain.
55
10) Lumbar hernia
Lumbar hernias are fairly uncommon as associated to other ventral abdominal wall hernias,
accounting for less than 1.5% of all abdominal hernias. They are relatively rare. These occur
more commonly in males and are twice common on the left than the right side. 56
Patients
are usually between 50 to 70 years old. These hernias can occur anywhere within the lumbar
region but are more common through the superior lumbar triangle. This may be post-
surgical or following blunt injuries associated with intra-abdominal injuries. The
management of such patients constitutes a surgical challenge.57
Clinical diagnosis of this
entity is difficult due to non-specific symptoms. The diagnosis is particularly indescribable
in obese individuals or in post-surgical patients. Though rare defects, lumbar hernias are
prone to incarceration and strangulation.58
Factors contributing to abdominal wall hernias:
11. 10 ‘Hernia and its types’
Factors contributing the formation abdominal wall defects can be separated into congenital
and acquired defects.59
Congenital defects: account for the majority of hernias. A patent processus vaginalis
is the primary cause for the development of indirect inguinal hernias. Pelvic floor
deformities can contribute to the development of hernias. Rarely, collagen
deficiencies contribute to the development of direct hernias. 60
Acquired defects: are normally responsible for direct hernia formation. Wear-and-
tear; straining to urinate, coughing, and heavy lifting contribute to weakening of the
abdominal wall.61
Factors contributing to failure of healing of abdominal incisions:
A large number of factors have been identified as contributing to the development of
incisional hernias. Strategies and surgical techniques are recognized which will reduce
the frequency of, but will not erase this problem.62
1. Obesity, especially morbid obesity, other reasons for abdominal distention [massive
omentum-“beer belly”, ascites]
2. Chronic obstructive airway disease [cough, increase in abdominal pressures, hypoxia
and poor oxygen delivery to the healing wound.]
3. Type of incision, i.e. more frequent after vertical than transverse. Long incision has
greater risk than short.
Multiple incisions destroy nerve and vascular supply.
Radiation therapy to the area of the incision reduces blood supply.
4. Creation of a stoma [parastomal hernia formation]
5. Age > 70years
6. Exposure to certain drugs [steroids, antimetabolites,
Immune suppressants]
7. Chronic diseases [renal, liver and cardiac failure]
8. Severe malnutrition
9. Diabetes [insulin dependent]
Studies have also shown a decreased ratio of collagen I: III, due to increase collagen III,
increase the risk of incisional hernia formation and reoccurrence [especially post
inguinal hernia repairs].
Assessments – Hernias
12. 11 ‘Hernia and its types’
1) Functional Examination
Patients newly developing external hernias must be screened for collateral conditions
that would lead to rises in abdominal pressure. These would include respiratory disease
with cough and forced expiration, and obstruction to the intestine or to the bladder outlet.
Failure to identify these provoking issues may lead to early recurrence after repair. 63
2) Symptoms
Patients with a groin hernia commonly present with complaints of a bulge in the inguinal
region that may or may not be associated with minor or vague discomfort. Extreme pain
in relation to a groin hernia usually indicates incarceration and strangulation of the
hernia’s contents. Occasionally a patient may present with paresthesias, symptoms of
inguinal nerve compression or irritation. 64
3) Physical examination
Examination of the patient standing demonstrates loss of regularity between the inguinal
areas or a distinct bulge. Coughing or the Valsalva maneuver may accentuate the bulge.
Next the clinician places their hand on the abdominal wall and repeats the Valsalva
maneuver, noting any presence of hernia, then places his/her fingertip into the inguinal
canal repeating the Valsalva maneuver again. Movement in a medial direction suggests
an indirect inguinal hernia, whereas direct anterior motion deep to the finger in the
superficial ring suggests a direct inguinal hernia. Although distinguishing direct and
indirect inguinal hernias is not essential at examination, differentiation of a femoral
hernia is important.65
Femoral hernias stick out inferior to the inguinal ligament,
adjacent to the femoral vessels the patient should be examined in the supine position,
repeating the same techniques used in standing. If the groin mass is not significant, have
the patient stand or walk for a short period of time. The mass, if incarcerated, may be
reduced with mild pressure towards the inguinal ring in the Trendelenburg position.
Reduction of an incarcerated hernia should be abandoned if it does not return easily to
the abdomen. Hernias which become incarcerated will require surgical management;
attempting to reduce it with a combination of force, sedation and analgesia serves little
purpose. 66
4) Differential diagnosis of a groin mass
Simple hernias reduce when the patience is leaning. Incarcerated hernias are not mobile,
but rigid and bound to the hernial defect boarders. Listed below are some the more
common groin lesion misidentified as groin hernias. 67
Ilio inguinal adenitis, lymphoma and other neoplasms due not reduce on recumbence
and are mobile allowing for differentiation from the simple or incarcerated hernia.
13. 12 ‘Hernia and its types’
Varicoceles, epididymitis & testicular torsion are discrete conditions of the scrotum;
palpation of the mass reveals lack of continuity with superficial ring.
Careful palpation of a hydrocele, excess fluid accumulation in a persistent processeus
vaginalis, demonstrates a discrete neck that can be “pinched off” from the cord
above.
A psoas abscess results from the dissection of a retroperitoneal infection along the
psoas muscle to the groin. A mass may appear below the inguinal ligament that
mimics a femoral hernia. History should suggest the presence of an intra-abdominal
inflammatory process (e.g. pancreatitis). 68
5) Treatment.
Ideally, all hernias should be treated surgically. Because the risk of incarceration,
strangulation and obstruction are greater than the risk of elective operation.
The principles of repair 69
Preparation of hernial sac
Opening the sac (herniotomy)
Return of hernial contents into the peritoneal cavity
Excision or reduction (invagination) of the hernial sac.
Repair of the hernial defect
- Tissue approximation
-Prosthetic reinforcement
Open (Lichtenstein, Rives)
Laparoscopic
6) Prevention of Different Types of Hernia: 70
Prevention is better than treating the different types of hernia. You cannot help yourself
if the hernia has occurred due to weakness in muscle but you can make sure it never
occurs due to any other reason which you can have under your control. This can help you
stay away from a hernia or if a hernia has occurred it will help you to make that hernia
stay under control. Some of the prevention tips for different types of hernia include:
14. 13 ‘Hernia and its types’
Maintain healthy body weight by practicing exercises regularly is a good way to
prevent any type of hernia.
Giving up smoking can aid in preventing few different types of hernia
Trying to lift objects with the help of your knees and not back to prevent different
types of hernia.
Immediately seeking medical help when you are sick to avoid getting a long time
cough.
Avoid lifting weights that are too heavy for you to lift.
Straining to be avoided during bowel movements or urination is a great way to
prevent different types of hernias.
It is very important to treat any type of hernia as soon as you know about the problem.
Also try to minimize the effects of hernia by taking prevention measures.
Summary:
A hernia happens when an organ or maybe fatty tissue squeezes through a weak
spot in a surrounding muscle or connective tissue called fascia
You may have a hernia if you can feel a soft lump in your belly or groin or in a
scar where you had surgery in the past.
Anything that effects rise in pressure in the abdomen can cause a hernia, including
: Lifting heavy objects , Diarrhea or constipation,Persistent coughing or sneezing
15. 14 ‘Hernia and its types’
Ideally, all hernias should be treated. Because the risk of incarceration,
strangulation and obstruction.
There is different types of hernias according to their position in body: Inguinal
Hernia, Femoral, Umbilical, Incisional and parastomal, Epicastric , Hiatal ,
Spigelian , Obturator ,Sciatic ,Lumbar hernia.
Patients with a groin hernia commonly present with complaints of a bulge in the
inguinal region that may or may not be associated with minor or vague discomfort.
Factors contributing the formation abdominal wall defects can be separated into
congenital and acquired defects
Not any bulge refers to a hernia because it maybe tumor, lymphoma, psoas, etc.
Prevention is better than treating.
References:
1
Belloc H. On. Freeport, N.Y.: Books for Libraries Press; 1967.
2
BIRKETT J. Hernia. 1864.
3
Nyhus L, Condon R. Hernia. Philadelphia: J.B. Lippincott; 1995.
4
Jones D. Hernia surgery. Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins Health; 2013.
5
Belloc H. On. Freeport, N.Y.: Books for Libraries Press; 1967.
6
Coene E, Vinke H, Duijn H, Bron W. Hernia. [Amsterdam]: Stichting September; 2014.
7
Büchler M. Laparoscopic hernia repair: a new standard?. Basel [u.a.]: Karger; 1995.
8
Chevrel JP, Rath AM. Classifi cation of incisional hernias of the abdominal wall. Hernia. 2000
9
Iason AH (1941) Hernia. Blakiston, Philadelphia
10
Gans SL (1959) Sliding inguinal hernia in female infants. Arch Surg 79:109
16. 15 ‘Hernia and its types’
11
Scarpa A (1814) A treatise on hernia, transl Wishart JH.Longman, Hurst, Rees, et al., Edinburgh
12
Jamadar DA, Franz MG. Inguinal region hernias. Ultrasound Clin. 2007
13
Aasvang EK, Gmaehle E, Hansen JB, et al. Predictive risk factors for persistent postherniotomy pain.
Anesthesiology. 2010;
14
Koop CE (1957) Inguinal hernias in infants and children. Surg Clin North Am 1675–1682
15
Maingot R (1961) Operations for sliding herniae and for large incisional herniae. Br J Clin Pract 15:993–103
16
Moschowitz AV (1925) The rational treatment of sliding hernia. Ann Surg 81:330
17
Townsend CM, Beauchamp RD, Evers BM, Mattox KL. Sabiston textbook of surgery E-book. Elsevier Health
Sciences; 2016 Apr 22.chapter40.
18
Belloc H. On. Freeport, N.Y.: Books for Libraries Press; 1967.
19
Wantz G. Complications of Inguinal Hernial Repair. 2018.
20
Nyhus L, Condon R. Hernia. Philadelphia: J.B. Lippincott; 1995.
21
Jones D. Hernia surgery. Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins Health; 2013.
22
Hope W, Cobb W, Adrales G. Textbook of hernia.
23
Campanelli G. Inguinal hernia surgery.
24
Schumpelick V, Fitzgibbons R. Recurrent hernia. Heidelberg: Springer Medizin; 2007.
25
Wagner J. Hernias. New York: Nova Science; 2011.
26
Sutton A. Surgery sourcebook. Detroit, Mich.: Omnigraphics, Inc.; 2013.
27
Colombo D, Rossi G. Prostheses. New York: Nova Biomedical, Nova Science Publishers; 2012.
28
Jones K. Surgery sourcebook.
29
Schumpelick V, Fitzgibbons R. Recurrent hernia. Heidelberg: Springer Medizin; 2007.
30
PADMAKUMAR R. LAPAROSCOPIC HERNIA REPAIR. [S.l.]: JAYPEE BROTHERS MEDICAL P; 2017.
31
Albin D. The hernia solution. Mill City Press, Inc.; 2011.
32
Sriram B. SRB's clinical methods in surgery.
33
Rogers B, Randolph S, Mastroianni K. Occupational health nursing guidelines for primary clinical conditions.
Beverly Farms: OEM Press; 2003.
34
Pediatr Surg Int 2006; 22(12):1033
35
Given JP, Rubin SZ. Occurrence of contralateral inguinal hernia following unilateral repair in a pediatric hospital.
J Pediatr Surg. Oct 1989
36
Hope W, Cobb W, Adrales G. Textbook of hernia.
37
Othersen HB Jr. The pediatric inguinal hernia. Surg Clin North Am. Aug 1993;73(4):853-9.
38
Jones D. Hernia surgery. Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins Health; 2013.
39
AP Cooper. The Anatomy and Surgical Treatment of Inguinal and Congenital Hernia. London: Longman & Co.
40
Skinner MA, Grosfeld JL. Inguinal and umbilical hernia repair in infants and children. Surg Clin North Am. Jun
41
JA Ring. A case of internal inguinal hernia. Lond Med Reposit 1814;2:204.
42
Muysoms FE, et al. Classifi cation of primary and incisional abdominal wall hernias. Hernia. 2009
43
Chevrel JP, Rath AM. Classifi cation of incisional hernias of the abdominal wall. Hernia. 2000
44
Korenkov M, et al. Classifi cation and surgical treatment of incisional hernia. Results of an experts’ meeting.
Langenbecks Arch Surg. 2001
45
Collins R. Incisional and congenital diaphragmatic hernia (CDH).
46
Memon M. Hiatal Hernia Surgery.
47
DM Lloyd, KJ Karmand, MGA Norwood. An inguinal hernia of a third kind? Hernia 2009;13:77–79.
48
WN Warvi, TG Orr. Internal supravesical hernias. Surgery 1940;8:312–325.
49
Sutton A. Surgery sourcebook. Detroit, Mich.: Omnigraphics, Inc.; 2013.
50
Smith T. Coping successfully with your hiatus hernia.
51
Potterton D. Hiatus hernia. London: Foulsham; 1993.
52
Hiatal Hernia Causes, Picture, Symptoms, Tests, and Treatments [Internet]. [cited 22 February 2018]. Available
from: https://www.webmd.com/digestive-disorders/hiatal-hernia
53
Murkoff H, Eisenberg A, Hathaway S. What to expect the first year. New York: Workman Pub.; 2009.
54
Bodhe YG (1959) Condition of the testicle after division of the cord in treatment of hernia.
55
Y. Watanabe, M. Mike and N. Kano, “Inguinal Hernia Repair in Consideration of Mesh Material,” Geka, No. 11,
2007
56
Bailey H, Bulstrode CJ, Love RM. Bailey & Love's short practice of surgery. Crc Press; 2008.
17. 16 ‘Hernia and its types’
57
. Meinke AK. Totally extraperitoneal laparoendoscopic repair of lumbar hernia. Surgical Endoscopy and Other
Interventional Techniques. 2003 May 1;17(5):734-7.
58
Baker ME, Weinerth JL, Andriani RT, Cohan RH, Dunnick NR. Lumbar hernia: diagnosis by CT. American
Journal of Roentgenology. 1987 Mar 1;148(3):565-7.
59
Scarpa A (1814) A treatise on hernia, transl Wishart JH. Longman, Hurst, Rees, et al., Edinburgh
60
Banks WM (1887) Some statistics on operation for the radical cure of hernia. BMJ 1:1259
61
M. Mike and N. Kano, “Inguinofemoral Hernia Repair in the Original Papers—McVay Operation,” Shujyutu, 61,
No. 13, 2007
62
U. Dahlstrand . Sandblom and U. Gunnarsson, Hernia Repair. A, S. Wollert, P.Nordin, G
“Emergency Femoral Study Based on a National Register,” Annals of Surgery, 2009.
63
C. E. Tobin, J. A. Benjaminand J. C. Wells, “Continuity of the Fascia Lining the Abdomen, Pe Cord,” Surgery,
Gynecology & Obstetrics, Vol. 83, No. 5, lvis, and Spermatic 1946.
64
T. Sato, “Fundamental Plan ofthe Fascial Strata of the Body Wall,” Igakunoayumi, Vol. 114, No. 13, 1980
65
T. H. Quinn, “Anatomy of the Groin: A View from the Anatomistm,” In: L. M. Nyhus and R. E. Condon, Eds.,
Hernia, 5th Edition, Lippincott Williams &Wilkins, Philadelphia, 2002, pp. 55-70.
66
I. L. Lichtenstein, A. G. Shulman, P. K. Amid and M. M. Montllor, “The Tension-Free Herniopla can Journal of
Surgery, Vol. 157, No. 2, 1989,
67
G. Ruggi, “Metado Operativo Meovo per la Cure Radicale Dell’Ernia Crurale,” Bull Sci Med Bologna, Vol.
7,No.3, 1892,
68
7. Basu S. Author’s reply: A hernia in the inguinal region is not always an inguinal hernia. Hernia (2007) 11:449–
451. Hernia. 2007;12(2):221-221.
69
3. Hernia: Causes, Treatment, and Prevention - Health Line [Internet]. [cited 22 February 2018]. Available from:
https://www.healthline.com/health/hernia
70
re of In- E. Bassini, “New Operative Method for the Cure of inguinal Hernia,” Ciné-Med Inc., Woodbury, 2008.
Figures References :
Figure 1: Journal of Epidemiology and Community Health, 1978, 32, 59-67
Figure 2: https://myhealth.alberta.ca/Health/aftercareinformation/pages/conditions.aspx?hwid=te8190
Figure 3: http://medical-dictionary.thefreedictionary.com/_/viewer.aspx?path=MosbyMD&name=femoral-
hernia.jpg&url=http%3A%2F%2Fmedical-dictionary.thefreedictionary.com%2Ffemoral%2Bhernia
Figure 4: https://www.drugs.com/cg/umbilical-hernia-discharge-care.html
Figure 5 : https://www.drugs.com/cg/incisional-hernia.html
Figure 6: https://herniaonline.com/hernias/epigastric/
Figure 7: http://www.ketogenic-diet-menu.com/2016/11/gastric-hernia-symptoms.html