CRIANÇA, INFANTIL, JUVENIL: DESENVOLVIMENTO SEXUAL PRECOCE E CRESCIMENTO LINEAR INICIAL EXAGERADO
•Télécharger en tant que DOCX, PDF•
0 j'aime•517 vues

A solução mais adequada é uma avaliação profissional minuciosa e não necessariamente a espera de um possível pulso ou estirão longitudinal, que poderá ou não ocorrer e se ocorrer será provavelmente de poucos centímetros na estatura ou altura, afinal não podemos, grosso modo, afirmar se tal possível estirão será de 2 cm ou 10 cm, etc., que muito provavelmente em uma criança com tais características merece uma avaliação e um tratamento provável com inibidores da aromatase e GH.

Recommandé
Recommandé
Contenu connexe
Plus de Van Der Häägen Brazil
Plus de Van Der Häägen Brazil (20)
Dernier
Dernier (7)
CRIANÇA, INFANTIL, JUVENIL: DESENVOLVIMENTO SEXUAL PRECOCE E CRESCIMENTO LINEAR INICIAL EXAGERADO
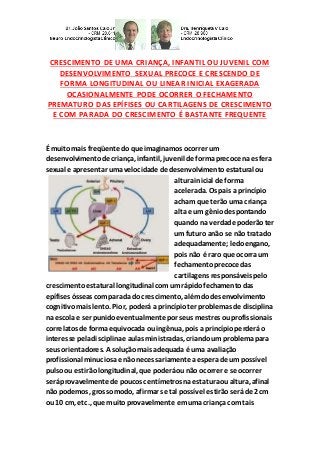
- 1. CRESCIMENTO DE UMA CRIANÇA, INFANTIL OU JUVENIL COM DESENVOLVIMENTO SEXUAL PRECOCE E CRESCENDO DE FORMA LONGITUDINAL OU LINEAR INICIAL EXAGERADA OCASIONALMENTE PODE OCORRER O FECHAMENTO PREMATURO DAS EPÍFISES OU CARTILAGENS DE CRESCIMENTO E COM PARADA DO CRESCIMENTO É BASTANTE FREQUENTE É muito mais freqüente doque imaginamos ocorrer um desenvolvimentode criança, infantil, juvenil de formaprecoce na esfera sexual e apresentar umavelocidade de desenvolvimentoestatural ou alturainicial de forma acelerada. Os pais a princípio acham que terãouma criança alta e um gêniodespontando quando na verdade poderãoter um futuro anão se não tratado adequadamente;ledoengano, pois não é raro que ocorraum fechamentoprecoce das cartilagens responsáveispelo crescimentoestatural longitudinal comum rápidofechamentodas epífises ósseas comparada do crescimento, alémdodesenvolvimento cognitivomais lento. Pior, poderá a princípioter problemas de disciplina na escolae ser punidoeventualmente por seus mestres ouprofissionais correlatos de formaequivocada ou ingênua, pois a princípioperderáo interesse peladisciplinae aulas ministradas, criandoum problemapara seus orientadores. A soluçãomais adequada é uma avaliação profissional minuciosae não necessariamente aesperade um possível pulsoou estirãolongitudinal, que poderáounão ocorrer e se ocorrer seráprovavelmente de poucos centímetros naestaturaoualtura, afinal não podemos, grossomodo, afirmar se tal possível estirãoseráde 2 cm ou 10 cm, etc., que muitoprovavelmente emuma criança com tais
- 2. características merece umaavaliação e um tratamentoprovável com inibidores daaromatase e GH-hormôniode crescimento, que propiciará o mais cedopossível umcrescimentocompensatórioapartir do iníciodo tratamentose ocorreremdeficiências hormonais. Por exemplo:o crescimentode ummenino com DGH, o qual demonstrouum crescimentoprogressivoinsuficiente até os seis (6) anos de idade cronológica, quando for tratadocom GH-hormôniode crescimento ocorreráum aumento da estaturaou alturalongitudinal, incluindoum desenvolvimentoorgânicoe cognitivoadequadoa um crescimento compensatório, emboradevaficar claro, que tratamentonão recuperao tempoperdido, pois como se enfatizaemdiversas pesquisas na literaturacientífica, acompensaçãoa partir do já estabelecidosó ocorrerámediante um tratamentoespecíficocorretivoexecutadopor médicoendocrinologista, neuroendocrinologistaoude outra área com conhecimentos adequados. CONCLUSÃO:Quandoos pais, mestres, pediatras, ououtromédico avaliaremum quadro semelhante aodescrito, é de bom sensoque pense na possibilidade de não ser culpada criança, infantil, ou juvenil. Nosso organismoé uma maravilhada natureza, entretanto, estásujeitoa pequenas alterações orgânicas noinícioque se tornarão estigmatizantes e desastrosas nasequênciadaqualidade de vida de humanos se não foremtomadas atitudes preventivas muitoclaras e precoces. CHILD, INFANT AND JUVENILE WITH SEXUAL EARLY DEVELOPMENT AND INITIAL GROWTH PITCH EXAGGERATED. GROWTH OF A CHILD, INFANT AND JUVENILE WITH EARLY SEXUAL DEVELOPMENT AND INITIAL GROWING ALONG OR LINEAR EXAGGERATED OCCASIONALLY LOCK PREMATURE EPIPHYSEAL CARTILAGE OR STOP WITH GROWTH AND GROWTH IS QUITE FREQUENTLY:PHYSIOLOGY-ENDOCRINOLOGY-NEUROENDOCRINOLOGY- GENETICS-ENDOCRINE-PEDIATRICS (SUBDIVISIONOF ENDOCRINOLOGY): DR. JOÃO SANTOS CAIO JR. ET DRA. HENRIQUETA VERLANGIERI CAIO.
- 3. It is much more common than a development of child, infantile and juvenile early sexual development andheight development or initial height inan expeditedmanner imaginedoccur. Parents at first think he will have a highchild and an emerging genius when infact may have a future dwarf if not properly treated;certain mistake, it is not unusual that an early closing of the cartilages is responsible for longitudinal height growthwitha rapid closure of epiphysis withbone growth arrest, inadditionto slower cognitive development occurs. Worse, youmay at first have discipline problems inschool andeventually be punishedby their masters or relatedprofessionals misguidedor naive way, because at first you will lose interestinthe discipline andtaught classes, creating a problemfor their supervisors. The best solutionis athorough professional evaluation, not necessarily waiting for a possible wrist or longitudinal growthspurt, whichmay or may not occur and if it occurs will probably be a fewcentimeters inheight, after all we cannot say whether this broadly as possible spurt is 2 cm or 10 cm, etc., likely ina childwithfeatures suchdeserves areviewanda likely treatment with aromatase inhibitors andGH-growthhormone, which will provide the earliest possible compensatory growthfrominitiationof treatment growthhormone deficiency (GHD) occurs. For example:the growthof a boy withGHD, whichdemonstratedaninsufficient progressive growth until six (6) years of chronological age, when treatedwithGH-growth hormone occurs an increase inheight or longitudinal height, including a suitable organic and cognitive developmentoncompensatory growth
- 4. althoughit shouldbe clear that treatment does not recover lost time, because withis emphasizedinseveral studiesinthe scientific literature, the compensationfrom the already establishedonly occur whena specific treatmentadvisedfor medical endocrinologist, neuroendocrinologist or other appropriate area. CONCLUSION:Whenparents, teachers, pediatricians, or other medical assess the manner describedframework, it is commonsense tothink of the possibility of not being the fault of the child, infant, juvenile or youth. Our body is a marvel of nature, however is subject tosmall changes in organic beginning to become stigmatizing anddisastrous sequence inthe quality of human life if not takenpreventive attitudes very clear and premature. Dr. João Santos Caio Jr. Endocrinologia – Neuroendocrinologista CRM 20611 Dra. Henriqueta V. Caio Endocrinologista – Medicina Interna CRM 28930 Como saber mais: 1. Elas devemser interpretadas levando-se emcontaa nutrição, status psicossociais e idade óssea... http://hormoniocrescimentoadultos.blogspot.com 2. O IGFBP-3 é GH-dependentee casosuas concentrações tambémse encontrembaixas, consistememevidências de deficiênciade GH- hormônio de crescimentoemcomparação com a determinaçãoisolada do IGF-1... http://longevidadefutura.blogspot.com 3. A GrowthHormone ResearchSociety estabeleceucritérios que tentam
- 5. regular os diagnósticos de deficiênciade GH-hormôniode crescimento na fase da criança, infância, juventude ouadolescênciaapesar da variabilidade dos métodos... http://imcobesidade.blogspot.com AUTORIZADO O USO DOS DIREITOS AUTORAIS COM CITAÇÃO DOS AUTORES PROSPECTIVOS ET REFERÊNCIA BIBLIOGRÁFICA. Referências Bibliográficas: Caio Jr, João Santos, Dr.; Endocrinologista, Neuroendocrinologista, Caio,H. V., Dra. Endocrinologista, Medicina Interna – Van Der Häägen Brazil, São Paulo, Brasil; Gallahue, D. 1993. Motor development and movement skill acquisition in early childhood education. In Handbook of research on the education of young children, ed. B. Spodek, 24-41. New York: Macmillan; Gardner, H. 1991.The unschooled mind: How children think and how schools should teach. New York: Basic; Goleman, D. (1995). Emotional intelligence. New York: Bloomsburg; Greenspan, S. and Greenspan, N.T. (1989). First Feelings: Milestones in the Emotional Devlopment of Your Baby and Child; Hohmann, M., & D. Weikart. (1995). Educating young children: Active learning practices for preschool and child care programs. Ypsilanti, MI: High/Scope Educational Research Foundation; Jensen, E. (2000). Moving with the brain in mind. Educational Leadership, 58(3), 34-37; Jenson, B. J., & Bullard, J. A. (2002). The mud center: Recapturing childhood. Young Children, 57(3), 16-19; Kamii, C., & J.K. Ewing. (1996). Basing teaching on Piaget's constructivism. Childhood Education 72 (5): 260-64; Schor, E.L. , (January, 1999). Early Brain Development and Child Care. Healthy Child Care America. (3), 1, 5-8; Shore, R. (1997). Rethinking the Brain: New Insights into Early Development. New York: Families & Work Institute. Contato: Fones: 55 11 5087-4404 ou96197-0305 Nextel: ID:111*101625 Rua Estela, 515 - BlocoD - 12ºandar - Conj. 121/122 Paraiso - São Paulo - SP - Cep 04011-002 e-mails:drcaio@vanderhaagenbrasil.com drahenriqueta@vanderhaagenbrasil.com vanderhaagen@vanderhaagenbrasil.com Site Van Der Häägen Brazil www.vanderhaagenbrazil.com.br www.clinicavanderhaagen.com.br www.crescimentoinfoco.com www.obesidadeinfoco.com.br
- 6. http://drcaiojr.site.med.br http://dracaio.site.med.br Joao Santos Caio Jr http://google.com/+JoaoSantosCaioJr Video http://youtu.be/woonaiFJQwY Google Maps: http://maps.google.com.br/maps/place?cid=5099901339000351730&q=Van+Der+Haagen+Brasil&hl= pt&sll=-23.578256,46.645653&sspn=0.005074,0.009645&ie =UTF8&ll=-23.575591,- 46.650481&spn=0,0&t = h&z=17