Improving validity and reproducibility of primary care database studies: An online clinical codes repository

Poster presented at SAPC 2013 at SAPC conference, Nottingham on 3/07/2013. David A. Springate, Evangelos Kontopantelis, David Reeves Primary Care Research group, Centre for Biostatistics, University of Manchester Publications in healthcare research using electronic medical records (EMR) databases are increasing at an exponential rate. Because of the amount of data available in large EMR databases, it has been suggested that they may be able to provide results of equal validity to randomised controlled trials. EMR studies rely on clinical codes (such as Read codes) to provide standardised and expressive means for medical professionals to record clinical information. The validity of these studies is dependent on (among other things) the validity of the clinical codes that are used to define the population of interest and their disease conditions. Clinical codes should be held to scrutiny in the same way as other methods since if the inclusion/exclusion criteria for a given condition is invalid then so will be the rest of the study. Also, it should be possible to replicate a given study (e.g. in a different EMR database) based on the information provided in the original paper, not possible if the lists of clinical code definitions are not provided. Furthermore, access to historical code-lists allows researchers and clinicians to make incremental improvements to disease and other definitions, building on and avoiding unnecessary replication of previous work There is currently no obligation to publish clinical code lists and no centralised repository to hold them. Consequently, the vast majority of database studies do not publish their clinical codes and as such are impossible to be fully validated or replicated. To illustrate this, we looked at 45 UK case-control EMR database studies indexed on PubMed and found that only five had any record of any clinical codes in their methodology sections. Of these five, only two published code lists in online appendices and only one provided a full set of codes that would allow for proper replication of the study. We have built an online repository where researchers can deposit their clinical codes at the time of publication in a standardised way, as well as download historical code lists from previous studies. We have uploaded a complete set of Read codes for all versions of the Quality and Outcomes Framework and encourage all code lists published by major medical organisations to be deposited. Reproducibility and validity of EMR database studies would be greatly aided if deposition of all clinical codes was a prerequisite for publication of all future database studies. The ability to build on code lists from historical studies during the development of new code lists will also ease a considerable bottleneck in database study design, removing the need for a huge deal of “reinventing of the wheel” each time a new EMR-based study is undertaken.
Recommandé

Recommandé
Contenu connexe
Dernier
Dernier (20)
En vedette
En vedette (20)
Improving validity and reproducibility of primary care database studies: An online clinical codes repository
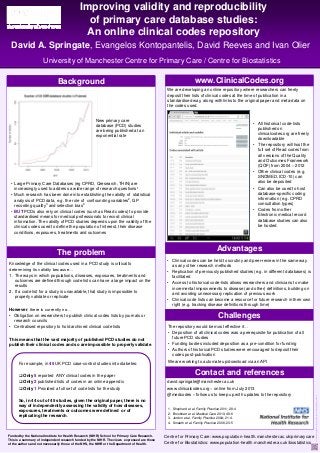
- 1. PosterTemplatefromwww.manchester.ac.uk/photographics Funded by the National Institute for Health Research (NIHR) School for Primary Care Research. This is a summary of independent research funded by the NIHR. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health. Background Centre for Primary Care: www.population-health.manchester.ac.uk/primarycare Centre for Biostatistics: www.population-health.manchester.ac.uk/biostatistics For example, in 45 UK PCD case-control studies into diabetes: Only 5 reported ANY clinical codes in the paper Only 2 published lists of codes in an online appendix Only 1 Provided a full set of code lists for the study So, in 44 out of 45 studies, given the original paper, there is no way of independently assessing the validity of how diseases, exposures, treatments or outcomes were defined or of replicating the research. 1. Shephard et al. Family Practice 2011; 28:4 2. Brookhart et al. Medical Care 2010; 48:6 3. Jordon et al. Family Practice 2004; 21:4. 4. Smeeth et al. Family Practice 2006; 23:5 • All historical code-lists published on clinicalcodes.org are freely downloadable • The repository will host the full set of Read codes from all versions of the Quality and Outcomes Framework (QOF) from 2004 – 2012 • Other clinical codes (e.g. SNOMED, ICD-10) can also be deposited • Can also be used to host database-specific coding information (e.g. CPRD consultation types) • Codes from other Electronic medical record database studies can also be hosted The repository would be most effective if… • Deposition of all clinical codes was a prerequisite for publication of all future PCD studies • Funding bodies included deposition as a pre-condition for funding • Authors of historical PCD studies were encouraged to deposit their codes post-publication We are working to automate up/download via an API Challenges Improving validity and reproducibility of primary care database studies: An online clinical codes repository University of Manchester Centre for Primary Care / Centre for Biostatistics David A. Springate, Evangelos Kontopantelis, David Reeves and Ivan Olier Knowledge of the clinical codes used in a PCD study is critical to determining its validity because… 1. The ways in which populations, diseases, exposures, treatments and outcomes are defined through code lists can have a large impact on the results 2. If a code list for a study is unavailable, that study is impossible to properly validate or replicate However, there is currently no… • Obligation on researchers to publish clinical codes lists by journals or research councils • Centralised repository to hold archived clinical code lists This means that the vast majority of published PCD studies do not publish their clinical codes and so are impossible to properly validate. The problem We are developing an online repository where researchers can freely deposit their lists of clinical codes at the time of publication in a standardised way, along with links to the original paper and meta-data on the codes used. www.ClinicalCodes.org • Clinical codes can be held to scrutiny and peer-review in the same way as any other research methods • Replication of previously published studies (e.g. in different databases) is facilitated • Access to historical code-lists allows researchers and clinicians to make incremental improvements to disease (and other) definitions, building on and avoiding unnecessary replication of previous work • Clinical code lists can become a resource for future research in their own right (e.g. tracking disease definitions through time) Advantages david.springate@manchester.ac.uk www.clinicalcodes.org – online from July 2013 @medcodes – follow us to keep up with updates to the repository Contact and references • Large Primary Care Databases (eg CPRD, Qresearch, THIN) are increasingly used to address a wide range of research questions1 • Much research has been done into establishing the validity of statistical analysis of PCD data, e.g. the role of confounding variables2, GP recording quality3 and selection bias4 • BUT PCDs also rely on clinical codes (such as Read codes) to provide standardised means for medical professionals to record clinical information. The validity of PCD studies depends upon the validity of the clinical codes used to define the population of interest, their disease conditions, exposures, treatments and outcomes New primary care database (PCD) studies are being published at an exponential rate