

Recommandé
Contenu connexe
Tendances
Tendances (20)
Similaire à Dizziness1
Similaire à Dizziness1 (20)
Plus de Doha Rasheedy
Plus de Doha Rasheedy (20)
Dernier
Dernier (20)
Dizziness1
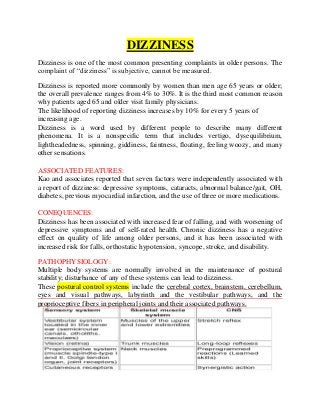
- 1. DIZZINESS Dizziness is one of the most common presenting complaints in older persons. The complaint of “dizziness” is subjective, cannot be measured. Dizziness is reported more commonly by women than men age 65 years or older; the overall prevalence ranges from 4% to 30%. It is the third most common reason why patients aged 65 and older visit family physicians. The likelihood of reporting dizziness increases by 10% for every 5 years of increasing age. Dizziness is a word used by different people to describe many different phenomena. It is a nonspecific term that includes vertigo, dysequilibrium, lightheadedness, spinning, giddiness, faintness, floating, feeling woozy, and many other sensations. ASSOCIATED FEATURES: Kao and associates reported that seven factors were independently associated with a report of dizziness: depressive symptoms, cataracts, abnormal balance/gait, OH, diabetes, previous myocardial infarction, and the use of three or more medications. CONEQUENCES: Dizziness has been associated with increased fear of falling, and with worsening of depressive symptoms and of self-rated health. Chronic dizziness has a negative effect on quality of life among older persons, and it has been associated with increased risk for falls, orthostatic hypotension, syncope, stroke, and disability. PATHOPHYSIOLOGY: Multiple body systems are normally involved in the maintenance of postural stability; disturbance of any of these systems can lead to dizziness. These postural control systems include the cerebral cortex, brainstem, cerebellum, eyes and visual pathways, labyrinth and the vestibular pathways, and the proprioceptive fibers in peripheral joints and their associated pathways.
- 2. The basic idea of sensory systems is to provide information to the system concerning its own state and that of its surroundings. The information is transferred from the sensory receptors to the CNS via afferent pathways. Age-Associated Changes Related to Dizziness: Evidence suggests that age-related changes occur in each of the vestibular, visual, auditory, and proprioceptive systems. Although these age-related changes do not likely cause clinical disease, they may predispose older persons to the occurrence of dizziness by making them more vulnerable to the effects of superimposed impairments and diseases. Degenerative changes and reductions in the number of sensory cells (hair cells) in the semicircular canals, saccule, and utricle have been reported with aging. Age-related visual changes include a decrease in visual acuity, dark adaptation, contrast sensitivity, and accommodation. Age-related decline in proprioception has not been extensively studied. Dizziness is usually categorized into one of four groups: Vertigo (sense of rotation or being pushed) Vertigo is considered to result from a disturbance within the vestibular system or its connections Pre-syncope or impending faint: result from a hypoperfusion of the brain. Imbalance (sensation localized to the body, relieved by sitting or lying down) usually results from Multiple mechanisms; abnormal proprioception, cerebellar, motor vestibulospinal function Ill-defined lightheadedness (cerebral sensation of being woozy, floating, swimming, visual abnormalities) A fifth category, which is common in the elderly, is “mixed dizziness.” CAUSES: 1. VERTIGO: PERIPHERAL CAUSES OF VERTIGO Benign positional vertigo Vestibular neuronitis Labyrinthitis Ménière disease CNS CAUSES OF VERTIGO Posterior circulation transient ischemic attacks or stroke ( Vertebrobasilar ischemia) Brainstem stroke or tumor. Cerebellopontine angle tumors. Posterior fossa pathologies. Multiple sclerosis. Spinocerebellar degeneration.
- 3. Migraine variant. A simple clinical test of the vestibuloocular reflex, called the head thrust or head impulse test: The patient’s head is held and a brief, small-amplitude, high acceleration head turn is applied to one side and then the other. The patient fixates on the examiner’s nose while the examiner watches for corrective rapid eye movements (saccades). In a unilateral peripheral vestibular disorder, the eyes move with the head in one direction instead of staying fixed. A refixation saccade is seen that brings the eye back on to the target. 2. PRESYNCOPE: Diffuse or global cerebral ischemia Cardiac Arrhythmia Vasovagal Orthostatic hypotension Volume depletion Medication effect Autonomic insufficiency 3. Dysequilibrium: Loss of vestibulospinal, proprioceptive, cerebellar function. Ototoxicity Peripheral neuropathy Cerebellar dysfunction Drug intoxication Extrapyramidal syndrome 4. LIGHTHEADINESS: Anxiety Panic disorder Hyperventilation syndrome Affective disorder CO poisoning Evaluation:
- 4. Because dizziness is a symptom that cannot be measured objectively, the history is Essential. After the patient's initial description, the following questions should be asked. 1. How many kinds of dizziness does the patient have? It is not uncommon to hear a very contradictory history only to find that the patient has more than one kind of symptom. 2. What does the patient mean when he says he is dizzy? 3. What is the symptom pattern (acute, recurrent, positional, or continuous)? Are all of the episodes the same? 4. Are there any associated symptoms (hearing loss, tinnitus, nausea, sweating)? 5. What medications (including alcohol) does the patient take or has taken recently (aspirin-like agents, anticonvulsants, antidepressants, aminoglycoside antibiotics,vasodilators, antihypertensives)? 6. What diseases does the patient have? Has he or she been sick recently? 7. What is the general level of activity, and how has this been affected? Episodic Vs. Continuous: If dizziness is episodic, the duration and frequency of the episodes should be identified, ● Episodes of vertigo lasting less than 1 minute suggest benign paroxysmal positional vertigo (BPPV). ● Episodes of vertigo lasting between 15 minutes and several hours suggest a transient ischemic attack (TIA) or migraine. ● Episodes of vertigo lasting between several hours and a couple of days suggest recurrent vestibulopathy or, if accompanied by tinnitus and hearing loss, Meniere’s disease. Continuous dizziness has a broad differential diagnosis. If dizziness begins abruptly and improves or remains the same, common causes include stroke, neurolabyrinthitis, cerebellar degeneration, peripheral neuropathy, physical deconditioning, drugs, anxiety, and depression. If onset is insidious, then psychological causes are particularly common, but acoustic neuroma should be ruled out. Recurrent Vertigo Patients often complain of recurrent episodes of vertigo. The duration of the episodes is important. Transient ischemic attacks usually last minutes, as compared with hours for diseases of the inner ear. The differential diagnosis of recurrent
- 5. attacks of vertigo includes vertebrobasilar ischemia, multiple sclerosis, Ménière disease, autoimmune inner ear disease, syphilis, and migraine. Provocative or Precipitating Factors Determining whether rolling over in bed or changing the position of the head or neck brings on the dizziness is useful; such patients usually have cervical or vestibular etiology. Dizziness on standing from the supine position is seen in postural hypotension. One should ask whether dizziness occurs after eating meals as is seen in postprandial hypotension. Dizziness developing after a change in medication needs careful review of side effects of that medication. Depressive disorders should be sought, using a standardized instrument, such as the Geriatric Depression Scale. Vertigo that is provoked by exertion, loud noise, sneezing, or coughing (Tullio’s phenomenon) is suggestive of perilymphatic fistula. ASSOCIATED SYMPTOMS: Symptoms commonly associated with vertigo are nausea,vomiting, and oscillopsia (the subjective sensation of oscillation of viewed objects).Peripheral causes of vertigo are associated with more severe nausea and vomiting than central causes are. Spontaneous nystagmus: Peripheral origin is indicated by the following characteristics: Horizontal with a torsional component Does not change direction with a change in gaze Slow phase toward affected ear; fast phase toward unaffected ear Decreased by visual fixation. At bedside, remove fixation and assess nystagmus using Fresnel lenses, blank sheet of paper in front of patient’s eyes, or an ophthalmoscope focused on the optic disc with the patient’s other eye covered. Nystagmus should be evident in the primary position. Note that the direction of the nystagmus is inverted when viewed through the ophthalmoscope. Central origin is indicated by the following characteristics: Often purely horizontal or vertical or torsional Changes in direction with changes in the position of the gaze (i.e., bi- or multidirectional). Visual fixation has little effect on nystagmus of central origin.
- 6. hearing loss, tinnitus, ear fullness associated with peripheral causes diplopia, dysarthria, and syncopal episodes associated with peripheral causes CAUSES OF DRUG-INDUCED OTOTOXICITY: Aminoglycosides. Penicillin. Aspirin. Sulfonamide. Antiepileptic drugs. Antihistamines. Causes in details: In benign positional vertigo, patients experience vertigo with a change in head position. The onset of symptoms often occurs when patients get into or out of bed or when they extend their neck, the top shelf syndrome. The diagnosis can be confirmed by eliciting fatigable nystagmus during the positioning maneuver Benign positional vertigo is usually caused by otolithiasis of the posterior semicircular canal. A variant involves the horizontal semicircular canal. Patients with this variant often complain that they have vertigo when they turn over in bed or when they turn their head from side to side while walking. Benign positional vertigo can be treated effectively by procedures designed to rotate the freely moving otoliths around the semicircular canal. One of these methods is the canalith repositioning procedure
- 7. After the procedure has been performed, have the patient keep the head upright for 48 hours. The maneuver is repeated as needed. The variant of benign positional vertigo also responds to a positioning maneuver—one that rotates the head in the plane of the horizontal semicircular canal. Central causes of positional vertigo include multiple sclerosis, brainstem tumor, cerebellar tumor or atrophy, and Arnold–Chiari malformation. These conditions are usually associated with other neurologic findings. Nystagmus due to a central cause is nonfatigable. The vertigo in vestibular neuritis develops over a period of hours, is severe for several days, and resolves within a few weeks. Often, a previous flulike illness is associated with vestibular neuritis. On physical examination, patients have spontaneous peripheral nystagmus, imbalance, and a positive head thrust test. Treatment of vestibular neuritis has been primarily symptomatic for nausea and vomiting. Some advocate the use of these “vestibular sedatives” only for severe nausea and vomiting because they suppress the ability of the nervous system to habituate and compensate for the vertigo. Corticosteroids and antiviral agents have been recommended for the treatment of vestibular neuritis. Because this condition improves spontaneously in most patients, many authorities recommend vestibular exercises and symptomatic treatment of the vertigo Labyrinthitis can develop over minutes to hours and can be associated with systemic ear, or meningeal infection. The physical examination findings of these patients are comparable to those of patients who have vestibular neuritis, with the addition of unilateral hearing loss. Syphilitic labyrinthitis can lead to recurrent episodes of vertigo, hearing loss, and tinnitus.
- 8. Perilymph fistula is an abnormal communication between the perilymph of the inner ear and the middle ear. It should be considered if vertigo develops abruptly in association with trauma, heavy lifting or straining, coughing or sneezing, or barotrauma. Coughing or sneezing can cause severe vertigo because of the change in pressure that is transmitted directly to the inner ear. Patients with chronic otomastoiditis with cholesteatoma are at risk for this. The fistula test is positive when the Valsalva maneuver produces vertigo. Refer the patient to otolaryngology. Labyrinthine ischemia has an abrupt onset and is usually associated with other neurologic signs and symptoms. Infarction confined to the inner ear or brainstem is usually the result of intra-arterial thrombosis of the posterior inferior cerebellar artery, anterior inferior cerebellar artery, or superior cerebellar artery. Isolated episodes of vertigo may represent transient ischemic attacks and may precede infarction of the labyrinth. This diagnosis should be suspected if the patient has cerebrovascular risk factors and suddenly develops hearing loss and vertigo Vertigo due to vertebrobasilar ischemia is usually associated with other neurologic symptoms. However, vertigo can be the only symptom of vertebrobasilar ischemia and should be suspected in a patient who has prominent cerebrovascular risk factors. Ischemia of the vestibular system in the brainstem should be suspected if a patient has unexplained vomiting that seems out of proportion to the symptoms of dizziness. Vertebrobasilar ischemia can cause recurrent attacks of vertigo. Associated symptoms include visual symptoms, unsteadiness, extremity numbness or weakness, dysarthria, confusion, and drop attacks. The most common causes of vertebrobasilar ischemia are embolism, large artery atherosclerosis, penetrating small-artery disease, and arterial dissection. The diagnosis is made on the basis of associated clinical signs and symptoms. Ménière disease is characterized by recurrent episodes of vertigo, tinnitus, and a fluctuating low-frequency hearing loss. All three of these features may not be present initially. Sudden falling spells, called otolithic catastrophes, have been reported in this disorder. In Ménière disease, the volume of the endolymph increases, causing distention of the endolymphatic system. Treatment recommendations include a salt restricted diet, diuretics, and vestibular suppressants. Ablative surgery is performed for intractable cases. Autoimmune disease of the inner ear can cause recurrent episodes of vertigo. The patient may present with a fluctuating hearing loss, tinnitus, and vertigo suggestive of Ménière disease. Unlike Ménière disease, autoimmune disease of the inner ear progresses rapidly over weeks to months and involves both ears. This disorder may involve only the inner ear or may be part of a systemic autoimmune disease such as polyarteritis nodosa or rheumatoid arthritis. Inner ear disease in conjunction with interstitial keratitis is called Cogan syndrome. These disorders have been treated with corticosteroids, cytotoxic drugs, and plasmapheresis. Syphilis, acquired or congenital, can cause recurrent episodes of vertigo and hearing loss. Syphilis can cause meningitis involving CN VIII, and it can cause temporal bone osteitis with
- 9. labyrinthitis. The diagnosis is based on positive findings on a fluorescent treponemal antibody absorption test. The VDRL test is positive in only 74% of cases. Treat syphilitic ear infections with penicillin. The association between vertigo and migraine is strong, and patients with migraine frequently have vertigo as part of their headache syndrome. Motion sensitivity is reported by more than 50% of patients with migraine. Vertigo without headache can be a symptom of migraine. This diagnosis should be suspected in a patient with recurrent attacks of vertigo who has a history of migraine or a positive family history of migraine. Cervical vertigo arises from irritation of proprioceptive receptors in the facet joints of the cervical spine. Osteoarthritis or muscle spasm is usually responsible. Clinically, vertigo or a more vague lightheadedness is reported, accompanied by an occipital headache and neck stiffness or pain. Management involves treating the underlying arthritis or acute neck problem. Two mechanisms have been proposed to explain cervical dizziness: proprioceptive deficits and vascular abnormalities. Proprioceptive deficits in the cervical spine can cause dizziness secondary to stimulation or proprioceptive receptors in the facet joints of the cervical spine. In older persons, cervical osteoarthritis most likely causes dizziness via this mechanism. The patient usually complains of pain in the neck upon movement, along with a worsening of dizziness. There is often a history of arthritis or whiplash injury. Further examination may reveal a decreased range of motion of the neck or signs of radiculopathy or mylopathy and/or spastic gait. A vascular mechanism causing cervical dizziness is thought to result from obstruction of the vertebral arteries. One theory is that when there is extensive blockage of one vertebral artery, rotation of the head can cause sufficient obstruction of the other vertebral artery to cause brainstem ischemia. Another theory is that when a person turns his/her head or neck, an osteoarthritic spur may press on the nearby vertebral artery, causing a transient disruption of the blood flow. If the patient describes imbalance, questions should focus on vision (glaucoma or refractive error), hearing, arthritis of the neck or extremities, alcohol use, and symptoms of peripheral neuropathy. The effect of support while walking (holding the elbow or carrying a cane) is important because a marked improvement in stability with only minimal support is characteristic of multiple sensory deficit. The possibility of Parkinson's disease should be considered. Dilated cerebral ventricles or a midline cerebellar tumor can also produce these symptoms without other specific neurologic findings. ill-defined lightheadedness. Generally, this symptom usually does not suggest a serious underlying disorder. This symptom may be secondary to medication, hyperventilation, or a previous stroke. In the winter months in conjunction with headache, carbon monoxide poisoning should be considered. Affective or anxiety disorders can also be associated with complaints of chronic lightheadedness.
- 10. PHYSICAL EXAMINATION: The physical examination is tailored to the history as described previously. Time spent taking a careful history can save time on the physical examination. Some of the following tests may be useful in evaluating the dizziness whose cause is unclear from the history: 1. Blood pressure taken in the supine position and after standing for 3 minute 2. Head turning (side to side and up and down) 3. Hyperventilation 4. Valsalva maneuver 5. Carotid sinus stimulation 6. Ear inspection and hearing test 7. Neurologic examination including: Evidence of previous stroke or parkinsonian features Sensory examination including joint position and vibration sense Cerebellar testing (past pointing suggests vestibular lesion; intention tremor and abnormal alternating movements suggest cerebellar dysfunction) Romberg's test Gait assessment 8. Hallpike's maneuver The Hallpike maneuver can be useful for assessment of some patients with true vertigo. Under ideal conditions, the patient should wear Frenzel's glasses. These have 20-diopter lenses with accompanying illumination so that the patient is unable to fixate visually and the eyes are under magnification. Peripheral vertigo is easily suppressed if the patient is allowed to focus on an object. The test begins with the patient in a sitting position on the examination table. The examiner quickly lays the patient down with the head hanging over the back of the table at approximately a 30-degree angle and the face turned 45 degrees to the right. The patient is observed for nystagmus and queried about vertigo or reproduction of the symptoms. The head is held there for 1 minute. The patient is then returned to the sitting position and again observed for 1 minute. The test is then repeated with the head held at 45 degrees to the other side. If vertigo is reproduced, the test should be repeated two or three times on the side that caused the most pronounced symptoms to see if the nystagmus and symptoms fade.
- 11. If BPV is present, after being positioned in the supine head-turned position, there will be : a short latency period of 5 to 15 seconds, and then the patient will complain of severe vertigo, and J-shaped, rotatory nystagmus may be observed. This will fade in less than a minute. Back in the sitting position, transient vertigo and nystagmus may be observed again. When tested on the other side, only 20% of patients have recurrent symptoms and findings. The vertigo will fade with repeated testing. During remissions or mild episodes of BPV, the Hallpike maneuver may be negative, and the diagnosis must be made on the history alone. When no nystagmus is elicited, BPV is still a more likely diagnosis than dizziness due to a central cause. A central lesion should be suspected if vertigo is dissociated from the nystagmus and if the nystagmus begins immediately on positioning, is primarily horizontal or vertical, lasts longer than 1 minute, or does not fade with repeated testing. 9. Other Provocative Tests Apart from the history and physical examination, certain provocative tests can be done at the bedside to evaluate the vestibular system. The most common causes of dizziness can be quickly diagnosed by reproducing a patient’s symptoms. However, some of these maneuvers should be performed (if at all) cautiously. To see if the vestibulo-ocular reflex (VOR), which helps to maintain visual stability during head movement, is intact, the following three tests can be done. The sensitivities, specificities, and predictive values of these tests for vestibular lesions in older persons have not been established. Head-Thrust Test In the head-thrust test, the patient is asked to fixate on the examiner’s nose, and the head is moved rapidly by the examiner about 10 degrees to the left or right. In a normally functioning VOR, the eyes will be fixed on the target, whereas in patients with a vestibular deficit, the eyes are carried away from the target along with the head, followed by a corrective saccade back to the target. For example, in a patient with a right-sided vestibular lesion, head thrusts to the right produce a slipping away of the pupils from the target followed by a corrective movement back to the target, whereas head thrusts to the left produce a normal response of the eyes. Post–Head-Shake Test In the post–head-shake test, the head is rotated either passively by the examiner or actively by the subject at a frequency of about 2 Hz in the horizontal plane for about 10 seconds, and then the examiner looks for nystagmus when the head is stopped. In unilateral peripheral
- 12. vestibular lesions, there will be a horizontal nystagmus with the fast phase usually beating toward the stronger ear, whereas in central lesions the nystagmus may be vertical. Dynamic Visual Acuity Testing This test is done by asking the patient to read a fixed eye chart while the examiner moves the head horizontally at a frequency of 1 to 2 Hz. A drop in acuity of two rows or more from the baseline is suggestive of an abnormal VOR. This test is sometimes difficult to perform, because patients may be able to read at times when the head is not in motion (i.e., at turn around points or by resisting movements). These tests are more helpful in detecting unilateral than bilateral vestibular dysfunction. It is important to remember that compensatory mechanisms may mask a vestibular deficit when these maneuvers are used in patients with longstanding vestibular loss. If the findings of these tests are abnormal, then the patient can be referred for more sophisticated vestibular testing such as electronystagmography and rotational testing. Stepping Test This test is positive when there is a lesion in the vestibulospinal system. The patient is asked to stand at the center of a circle drawn on the floor. The circle is divided into sections by lines passing at 30-degree angles. The patient is blindfolded and is asked to outstretch both arms at 90 degrees to the body. The patient is then asked to flex and raise high first one knee and then the other, and to continue stepping forward at a normal walking speed for a total of 50 or 100 steps. The examiner notes body sway while the patient marches in place with the eyes closed. In a unilateral vestibular lesion or in acoustic neuroma, there will be a gradual rotation of the body(more than 30 degrees) toward the affected side. Laboratory testing: depends on the working diagnosis and the site of presentation. In the emergency room, routine glucose determination (for hypoglycemia) and cardiac rhythm monitoring are useful in patients over age 45 who present with dizziness. In patients with acute vertigo, a CT scan to rule out a cerebrovascular event should be considered. In less acute settings, testing of patients with vertigo should include glucose determinations (to exclude hyperglycemia), thyroid function tests, and serologic tests for syphilis to identify potentially reversible causes. When the diagnosis remains unclear, consultation with a subspecialist from either the ear, nose, and throat (ENT) department or neurology department should be considered. They may perform dynamic tests of vestibular function such as electronystagmography and caloric testing. If there is evidence of a central lesion, a computed tomographic (CT) scan
- 13. directed through the petrous pyramids or a magnetic resonance imaging (MRI) scan may be considered, although many asymptomatic elderly patients have abnormal findings on MRI. These imaging techniques are not usually necessary and are best ordered after consultation with a subspecialist. Audiometry, which includes pure tone assessment, speech discrimination, impedance measurement, and evoked responses, is recommended for evaluating dizzy patients with hearing loss. Electronystagmography is the most established and widely used test. The procedure consists of a battery of tests designed to record eye movements in response to visual and vestibular stimuli. These include oculomotor evaluation, positional testing, and caloric testing. The oculomotor evaluation involves saccade testing, pursuit testing, optokinetic nystagmus, and spontaneous and gaze-evoked nystagmus. The positional testing is designed to detect nystagmus evoked when the head is held in different positions. The caloric testing assesses the symmetry of vestibular functions. This test can indicate the side of involvement in unilateral vestibular lesions. Each ear is stimulated fi rst with warm (44°C) and then cool water (30°C), each instilled over 30 seconds. The temperature change stimulates or suppresses the respective horizontal semicircular canals, resulting in nystagmus. There will be a decreased response on the ipsilateral side in peripheral vestibular disorder. Computer dynamic posturography (CDP) is used to test the vestibulospinal reflex and assess balance maintenance. This is a multisensory assessment of balance that has been shown to give insight into an individual’s functional status, compensation, and fall risk. CDP assesses the 3 major senses involved in balance: vestibular, vision, and proprioception. A force plate measures body sway under different visual and postural conditions. The sensory organization test (SOT) measures postural stability under 6 different sensory conditions. The first 3 conditions are tested with the patient standing on a firm surface with eyes open and closed and with perturbed vision (sway-referenced visual enclosure on a fixed platform). The final 3 conditions test the patient while standing on a perturbed surface with the same 3 visual conditions (eyes open, eyes closed, sway-referenced). The patient's reliance on particular sensory information is determined by comparing sway with normative values for each condition. VRT exercises then can be designed to address the specific areas of deficit. Limits-of-stability (LOS) testing is used to determine how well an individual can move the center of gravity over the base of support while maintaining an upright posture. Information from this test battery is useful for predicting fall risk and for determining specific balance exercises to improve movement skills without the patient experiencing a fall.
- 14. Those with pre-syncope should be evaluated in the same way as patients with syncope. Patients with a balance problem should undergo testing as dictated by the history and physical findings. In those with lightheadedness, drug level testing should be performed if appropriate. These patients do not require other diagnostic evaluation unless abnormalities on the above evaluation are identified. Treatment Therapy for vertigo is discussed initially; then recommendations for nonvertiginous dizziness are reviewed. If an elderly patient without a previous history of vertigo develops an acute episode of moderate or severe vertigo, hospital admission for observation and symptom control may be appropriate. It can be very difficult at times to rule out a brain stem or cerebellar infarction. Treatment of symptoms associated with acute vertigo usually includes medications with anticholinergic and antiemetic properties. A good initial choice is promethazine (Phenergan), which has both characteristics. It can be given orally, rectally, or intramuscularly in a dose of 12.5 to 50 mg. If the patient is excessively anxious, a benzodiazepine may also be a useful adjunctive therapy. For patients with mild or moderate bouts of vertigo, promethazine can be used if nausea is present, and meclizine (Antivert) if nausea is not present. One should start with a low dose of either agent (12.5 mg) at bedtime, gradually titrating the dose to the level tolerated. In general, medication should be used for only short periods of time. Chronic therapy is rarely indicated. A set of exercises has been developed to shorten the duration and impact of benign positional vertigo, but these should be reserved for the robust and interested patient. For those with pre-syncope, the specific etiology should be addressed (e.g., orthostatic hypotension, hyperventilation). For patients with balance problems or a multisensory deficit, a referral to physical therapy for gait evaluation, strengthening, and a gait-assist device is important, as is audiologic assessment and ophthalmologic screening. Appropriate treatment of patients with ill-defined lightheadedness begins by discontinuing any offending medications and also includes ophthalmologic assessment. Psychiatric evaluation is appropriate if other features suggest a psychiatric disorder. Physical therapy and exercise programs may be useful. Reassurance and regular follow-up are important. Vestibular Rehabilitation
- 15. Vestibular rehabilitation exercises focus on gaze stability and gait stability. Gait stability includes both static and dynamic balance exercises. VOR stimulation exercises The VOR maintains stable gaze and visual focus during active and passive head motion. This first set of exercises is designed to improve the gain and accuracy of the VOR. The first activity involves moving the head while focusing on a stationary target while attempting to maintain stabilizing gaze on the card. For head movements in phase with a target (X1 viewing), hold a card with lettering at arm's length with eyes focused on the letters. Move the head from side to side, increasing speed with each progression. Repeat the entire cycle 20-30 times. The head can also be moved vertically and diagonally. Progress from sitting to standing with the feet shoulder width apart to standing with the feet together to standing partially pointed (one foot half way ahead of the other) to standing pointed (one foot completely in front of the other). The patient should progress from standing on a firm surface to standing on a compliant surface. Post the card on the wall with a plain background and progress to posting on a wall with a busy patterned background. As function improves, the exercise can be advanced to moving the card opposite to head movement. For head movement “out of phase” with target (X2 viewing), the patient holds a card with lettering at arm's length with eyes focused on the letters. The patient moves the head to the right and the card to the left while keeping the eyes focused on the letters. Then, the patient moves the head to the left and the card to the right keeping the eyes focused on the letters. The patient begins slowly and increases speed as the test progresses but keeps the letters in focus. This is repeated the entire cycle 20-30 times. This test can also be performed in a vertical direction. The patient can progress from sitting to standing to a sharpened stance as described above. Ocular motor exercises To increase pursuit gain, the patient holds a card with lettering at arm's length. Then the patient moves the card left and right across the visual field, tracking with eye movement and keeping the head still. The full cycle is repeated 20-30 times. The test can be performed in the vertical and diagonal directions with increasing speed but being certain to keep the letters in focus. After this the patient can progress from sitting to standing to a sharpened stance as described above (see VOR stimulation exercises above). To improve saccade latency, velocity, and accuracy, the patient can hold a card with lettering in each hand approximately 15 inches apart at arm's length. While keeping the head still, the eyes are moved back and forth from card to card with 1 second per card. This is repeated 20-30 times for the complete cycle. This test also can be performed in the vertical and diagonal planes. The patient can progress from sitting to standing to a sharpened stance as described above (see VOR stimulation exercises above). Habituation exercises Habituation exercises are the focus of vestibular rehabilitation with respect to BPPV. Although 2007 guidelines for management of BPPV recommend initial treatment of BPPV with particle repositioning
- 16. maneuvers (PRMs) such as the Epley, Liberty, or Semont, more recent studies have shown that combining PRM with vestibular rehabilitation improve outcomes. Chang and Chern showed that additional vestibular rehabilitation exercise training that emphasized vestibular stimulation (repeated head movements to habituate vestibular responses) showed improved ability and functional gait performance in patients who had already undergone PRMs.[10] The experimental group demonstrated decreased sway velocity with eyes closed and single-leg stance with eyes closed after four weeks of treatment. Habituation exercises have also been shown to aid in the recovery of patients with vestibular neuritis. Balance exercises The patient stands with the feet together. The patient may maintain balance by reaching out and touching the wall in front of them. The patient begins to take the hands off the wall for progressively longer periods. First the patient begins by taking 1 hand at a time off the wall and alternates hands. Second, the patient sharpens the stance and stands with the feet shoulder-width apart looking at a target on the wall. The patient narrows the base of support by sharpening the stance. This is performed first with arms outstretched, then close to the body, and then folded across the chest. The patient can sit and then stand with the head bent forward 30° and head bent backward 30°. The patient reaches up as though for an object over the head and then bends over as though picking up an object from the floor. The patient can then progress from sitting to standing to a sharpened stance. Exercises are performed in dim lighting and then with eyes closed. The difficulty level is raised by standing on foam or a pillow and then standing to one leg. Another exercise is making a circle with a ball. The eyes focus on the ball and then the patient moves it in a circular fashion in both directions with increasing speed. The head and body moves with the ball. Difficulty level is raised as the patient progresses from sitting to standing to a narrowed stance. Tai chi is an effective adjunct to balance exercises, especially for those with imbalance when standing.[11] Recent studies have demonstrated beneficial effects of the traditional Chinese exercises such as tai chi on balance and decreasing fall risk. These slow and deliberate routines may train balance mechanisms in a different and complementary way to more conventional standing, walking, and head-movement exercises. Gait exercises In walking exercise 1, the patient begins by walking next to a wall with the hand out for support. Then, the patient gradually increases the number of steps without support. *Difficulty is raised by narrowing the stance and by walking heel to toe. In walking exercise 2, the patient walks with the head in motion going left and right with increasing speed. The stance is narrowed and the patient can also move the head in the vertical plane. The patient practices turning when walking, first with large circles, then with gradually smaller turns, in both directions.
- 17. In walking exercise 3 (sit to stand), the patient walks from one chair to another chair position 10 feet away. Upon reaching the first chair, the patient sits without using the hands, waits for 5 seconds, and rises without using the hands. The patient goes to the second chair, touches it, and, with support, practices standing on 1 leg for 5 seconds. The entire cycle is repeated 10 times. The patient can add head movements as the exercise progresses, increase walking speeds, and decrease the width of gait. Combined category exercises For an obstacle course, the patient can step over objects and around furniture. Difficulty is increased by bending over, picking up objects, throwing and catching objects, bouncing them off walls, and walking on differing compliance surfaces. The patient can also practice at the grocery store by pushing a cart. First the patient pushes with minimal support and then no support from the cart. The patient can begin with slow, small head movements, increasing speed and degrees of motion. Also the crowd can play a factor in the rehabilitation. The patient should go when few patients are shopping and then progress to a crowded time of the day. The patient should make an effort to look at items that are on the top and bottom shelves.The patient can also walk at the mall by beginning with slow walks close to the wall and by going with the flow of the crowd. Then the patient can increase speed, move away from the walls, and go against traffic. Window shopping with purposeful head movements is helpful. Computer-aided rehabilitation Recent advances in the ongoing research of vestibular dysfunction and rehabilitation have incorporated technology in the treatment sessions. One group incorporated virtual reality VRT into the traditional VRT sessions and documented improved posturography, vertigo, and mental health scores.At the time of its publication, the 2007 Cochrane review claimed that this study had been the only study which reached statistical significance in comparing different forms of vestibular rehabilitation. The review deemed that evidence was sufficient to support the addition of a simulator based activities to vestibular rehabilitation programs. NASA has used this virtual reality technology and taken it one step further. They hope to train the vestibular system to decrease motion sickness, increase function in disorienting environments, and speed recovery when returning to gravity and solid ground. The use of this technology is definitely exciting. Electrotactile stimulationVestibular rehabilitation has also been incorporated with electrotactile vestibular substitution system (EVSS) for the treatment of bilateral vestibular loss in patients with aminoglycoside-induced ototoxicity. Aquatic physiotherapyGabilan et al studied the use of aquatic physiotherapy as part of vestibular rehabilitation in patients presenting with chronic dizziness with unilateral vestibular hypofunction. All rehabilitation exercises took place in a pool and included tasks such as rotational control of the trunk, gait with thrust, sitting position on a float, upright buoyancy, and balance control during turbulence. The study found that the participants had lower DHI scores, reduction in variation of body displacement by posturography, and significantly lower self-perception of dizziness intensity.