Microbiolog , Pathology and Pharmacology of Leprosy
•
2 j'aime•1,281 vues

Download from the link: http://adf.ly/1OFFhb (copy and paste it in your browser) For more medical notes , please visit our website: www.mediconotes.com , subscribe and get more than 300 notes like this.

Recommandé
Contenu connexe
En vedette
Dernier
Dernier (20)
Microbiolog , Pathology and Pharmacology of Leprosy
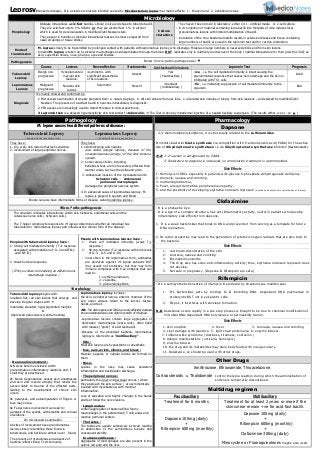
- 1. Microbiology Morphology - Obligate intracellular, acid-fast bacillus, similar in size and shape to tubercle bacilli. - They are acid-fast only to 5% H2SO4 or they are alcohol fast 1% in alcohol which is used for decolourization in modified Ziehl-Neelsen stain. - They appear in bundles or globular intracellular masses in smears prepared from nasal scrapings or tissue biobsy. Culture characters - They haven't been grown in laboratory, either on: 1- artificial media or 2-cell culture. - in vivo injection of material containing lepra bacilli into footpads of mice induces local granulomatous lesions with limited multiplication of bacilli. - inoculation of the nine-banded armadillo results in extensive disease and tissue containing large numbers of bacilli, are used in the lepromin test and for vaccine production. Mode of transmission - M. leprae is likely to be transmitted by prolonged contact with patients with lepromatous leprosy who discharge M.leprae in large numbers in nasal secretions and from skin lesions. - Inhaled M. leprae, is taken up by alveolar macrophages and disseminates through the blood BUT replicates only in relatively cool tissues of the body ( optimal temperature for their growth is 30C) as skin, superficial nerves, nose, pharynx, eyes and tesicles. Pathogenesis Below (micro-patho-pathogenesis) Course Lesions Nerve affection Bacteraemia Acid-fast bacilli in lesions Lepromin Test Prognosis Tuberculoid Leprosy Benign non- progressive Hypopigmented macular skin leasions. Asymmetric, with significant anaesthesia of skin leasions. Absent Few ( Paucibacillary ) +ve , i.e. the cell mediated immunity is intact causing the granulomatous response that causes nerve damage and the skin in infilitrated with Th1 cells Good Lepromatous Leprosy Malignant progressive Nodular skin lesions Summetric Present Abundant ( multibacillary ) -Ve , i.e. indicating suppression of cell mediated immunity to the organism. Bad Diagnosis It's mainly clinical and confirmed by: 1- Microscopic examination of smears prepared from: a- nasal scrapings b- slit skin smears from ear lobe c- ulcerated skin nodules or biopsy from skin leasions .. and stained by modified Ziehl- Neelsen. The presence of acid-fast bacilli in bunches intracellulary is diagnostic. 2- PCR assays are increasingly used to detect M.leprae in clinical specimens. 3-Lepromin test: is a delayed hypersensitivity skin test similar to tuberculin. The Test id done by intradermal injection of a heated bacillary suspension. (The results either +ve or –ve ) Pathogology Pharmacology M. leprae causes two different patterns of disease : Dapsone Tuberculoid Leprosy ( People with the less severe form ) Lepromatous Leprosy ( People with the more severe form ) - 4,4' diaminodiphenylsulphone, it is structurally related to the sulfonamides. It inhibits bacterial folate synthesis via competition with P-aminobenzoic acid (PABA) for the active site of dihydropteroate synthetase i.e via dihydropteroate synthetase inhibiton (Bacteriostatic). N.B, 1- Its action is antagonized by PABA. ……..2- Resistance to dapsone is increased, so combination treatment is recommended. . They have : 1- dry, scaly skin lesions that lack sensation. 2- involvement of large peripheral nerves. They have: 1- skin thickening and nodules. also called anergic leprosy, because of the unresponsiveness (anergy) of the host immune system. 2- Cooler areas of skin, including: Earlobes & feet, are more severely affected than warmer areas, such as the axilla and groin. 3- widespread invasion of the mycobacteria into Schwann cells - endoneural perineural macrophages damages the peripheral nervous system. 4- In advanced cases of lepromatous leprosy, M. leprae is present in sputum and blood Side Effects 1- Hemolysis of RBCs especially in patients with glucose 6-phosphate dehydrogenase deficiency. 2- Anorexia, nausea and vomiting. 3- methemoglobinemia, 4- Fever, allergic dermatitis, peripheral neuropathy, 5- and the possibility of developing erythema nodosum leprosum (a serious and severe skin complication of leprosy). People can also have intermediate forms of disease, called borderline leprosy. Clofazimine Micro-Patho-pathogenesis - It is a phenazine dye. - It is a dye of a complex structure, has anti-inflammatory activity, useful in patients who develop inflammatory side effects from dapsone. 1- It is a weak bactericidal that binds to DNA and prevents it from serving as a template for future DNA replication. 2- Its redox properties may lead to the generation of cytotoxic oxygen radicals that are also toxic to the bacteria. - The organism replicates intracellulary within skin histiocyts, endothelial cells and the cutaneous nerve cells ( Schwann cells ). - - The T-helper lymphocyte response to M. leprae determines whether an individual has tuberculoid or lepromatous leprosy and influences the clinical form of the disease : People with tuberculoid leprosy have : 1- Strong cell mediated immunity ( TH1 response ….associated with production of: IL-2 and IFN-γ …..and TNF-B ). 2- Weak humoral response. ( IFN-γ is critical to mobilizing an effective host macrophage response ) People with Lepromatous leprosy have : 1- Weak cell mediated immunity (weak TH1 response ) 2- Strong humoral (TH2 response with high levels of IL-4 , IL-5 and IL-10) - most often in the lepromatous form, antibodies are produced against M. leprae antigens BUT they usually not protective, but they may form immune complexes with free antigens that can lead to: 1- erythema nodosum, 2- vasculitis, 3- glomerulonephritis. Side Effects 1- red-brown discoloration of the skin. 2- Anorexia, nausea and vomiting 3- Eosinophilic enteritis. 4- The drug also has some anti-inflammatory activity; thus, erythema nodosum leprosum does not develop. 5- Not safe in pregnancy. (Depsone & Rifampicin are safe.) Rifampicin - It's a semisynthetic derivative of rifamycin B produced by streptomyces mediterranei. 1- It's bactercidal, acts by binding to & inhibiting DNA- dependant RNA polymerase in prokaryotic BUT not in eukaryotic cells. 2- IN pox, it interferes with envelope formation. N.B. Resistance occurs rapidly in a one step process is thought to be due to chemical modification of microbial DNA-dependant RNA polymerase or permeability barrier. Morphology Tuberculoid leprosy begins with: localized flat, red skin lesions that enlarge and develop irregular shapes with indurated, elevated, hyperpigmented margins & depressed pale centers (central healing). - Neuronal involvement : 1-Nerves become enclosed within granulomatous inflammatory reactions and, if small they are destroyed. 2- Nerve degeneration causes skin anesthesias and skin and muscle atrophy that render the person liable to trauma of the affected parts, leading to the development of chronic skin ulcers. 3- paralyses, and autoamputation of fingers or toes may ensue. 4- Facial nerve involvement can lead to : paralysis of the eyelids, with keratitis and corneal ulcerations. Lepromatous leprosy involves : the skin, peripheral nerves, anterior chamber of the eye, upper airways (down to the larynx), testes, hands, and feet. N.B. The vital organs and CNS are rarely affected, because the core temperature is too high for growth of M. leprae. -Lepromatous lesions contain large aggregates of lipid-laden macrophages (lepra cells), often filled with masses (“globi”) of acid-fast bacilli. -Because of the abundant bacteria, lepromatous leprosy is referred to as “multibacillary”. - Skin : Most skin lesions are hypoesthetic or anesthetic. - face, ears, wrists, elbows, and knees : Macular, papular, or nodular lesions are formed on them. - Nose : Lesions in the nose may cause persistent inflammation and bacilli-laden discharge. - The peripheral nerves : particularly the ulnar and peroneal nerves ( where they approach the skin surface ) are symmetrically invaded with mycobacteria, with minimal inflammation. Loss of sensation and trophic changes in the hands and feet follow the nerve lesions. - Lymph nodes : contain aggregates of bacteria-filled foamy macrophages in the paracortical (T-cell) areas and reactive germinal centers. - The testes : The testes are usually extensively involved, leading to destruction of the seminiferous tubules and consequent sterility. - In advanced disease : Aggregates of macrophages are also present in the splenic red pulp and the liver. Side Effects 1- skin eruption 2- fever 3- Anorexia, nausea and vomiting 4- Liver damage with jaundice. 5- light chain proteinuria 6- enzyme inducer. 7- Influenza-like syndrome ( dizziness, tiredness, confusion ) 8- Allergic manifestations ( urticaria, hemolysis ) 9- enzyme inducer. 10- the drug and its metabolites may stain body fluids with orange colours. 11- Resistance, so should be used with other drugs. Other Drugs Amithiozone, Ethionamide, Thioacetazone. Corticosteroids & Thalidomide control the lepra reaction during which the administration of sulfone is temporarily discontinued. Multidrug regimen Paucibacillary Multibacillary Treatment for 6 months Treatment for at least 2 years or more if the skin smear remain +ve for acid fast bacilli. Dapsone 100mg (daily) + Rifampicin 600mg (monthly) Dapsone 100mg (daily) + Rifampicin 600mg (monthly) + Clofazimine 300mg (daily) Minocycline or Fluoroquinolones maybe also used. On microscopic examination, All sites of involvement have granulomatous lesions closely resembling those found in tuberculosis, and bacilli are almost never found. The presence of granulomas and absence of bacteria reflect strong T-cell immunity. Leprosy(Hansen's disease), It is a slowly progressive infection caused by Mycobacterium leprae that mainly affects: 1- the skin and 2- peripheral nerves.