Neuromuscular blocking agents & reversal in anesthesia
•Télécharger en tant que PPTX, PDF•
131 j'aime•15,347 vues

dr.mushtaq ahmad consultant anesthetist,BVH,BWP,Pk

Recommandé
Contenu connexe
Tendances
Tendances (20)
Similaire à Neuromuscular blocking agents & reversal in anesthesia
Similaire à Neuromuscular blocking agents & reversal in anesthesia (20)
Dernier
Dernier (20)
Neuromuscular blocking agents & reversal in anesthesia
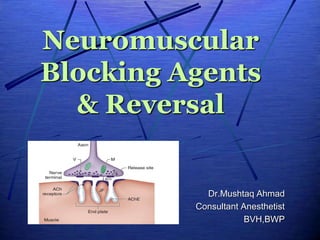
- 1. Neuromuscular Blocking Agents & Reversal Dr.Mushtaq Ahmad Consultant Anesthetist BVH,BWP
- 3. CONTENTS Introduction/history Neuromuscular transmission Distinctions Between Depolarizing & Nondepolarizing Blockade...mechanism of actions Classification depolarizing & Nondepolarizing Muscle Relaxants Reversal ...Cholinesterase Inhibitors & Other Pharmacologic Antagonists to Neuromuscular Blocking Agents
- 4. HISTORY
- 7. in 1942, when Griffith and Johnson in Montreal used Intocostrin, a biologically standardized mixture of the alkaloids of the • Indian rubber plant Chondrodendron tomentosum,to facilitate relaxation during cyclopropane anaesthesia. However, as noted by Beecher and Todd in 1954: • “muscle relaxants given inappropriately may provide the surgeon with optimal operating conditions in . . . • a patient [who] is paralyzed but not anesthetized—a state that is wholly unacceptable for the patient.” • In other words, muscle relaxation does not ensure unconsciousness, amnesia, or analgesia
- 8. Definition NMBA are the drugs that act peripherally at NM-Junction and muscle fiber itself to block neuromuscular transmission. • In order to facilitate muscle relaxation for surgery and • mechanical ventilation during surgery & in ICU.
- 10. Neuromuscular junction Association between a motor neuron and a muscle cell • Synaptic cleft...The cell membranes of the neuron and muscle fiber are separated by a narrow (20-nm) gap • Within the most distal aspect of the motor neuron, vesicles containing the neurotransmitter acetylcholine (ACh) can be found.
- 14. The postjunctional motor membrane ... motor end-plate is • highly specialized and invaginated, and the shoulders of these folds are rich in ACh receptors acetylcholinesterase ...... • Th is enzyme (also called specific cholinesterase or true cholinesterase) is • embedded into the motor end-plate membrane immediately adjacent to the ACh receptors.
- 15. Structure of ACh receptors structure of ACh receptors varies in diff erent tissues and at different times in development…… • Nicotinic & muscurinic Location of ACh receptors • Post junctional nicotinic ACh recepters...... located on the postjunctional motor membrane-.motor end-plate... • approximately 5 million of these receptors, but activation of only about 500,000 receptors is required for normal muscle contraction • Prejunctional ACh receptors .......are present and influence the release of ACh. • The prejunctional and postjunctional receptors have different affinities for ACh. • Extrajunctional ACh receptors .......are located throughout the skeletal muscle in relatively low numbers owing to suppression of their synthesis by normal neural activity.
- 16. Postjunctional ACh receptors, embedded in the lipid layer of the postsynaptic muscle membrane.
- 17. Prejunctional Ach receptors Pre- junctional acetylcholine receptors are present on the shoulders of the axon terminal, Stimulation of the prejunctional receptors mobilizes (MOB) the vesicles of acetylcholine to move into the active zone, • Ready for release on arrival of another nerve im-pulse. The mechanism requires ca2+ ions.
- 18. Maturation of the postsynaptic apparatus . At approximately 14 days after birth, the immature γ-subunit– containing acetylcholine receptors (AChRs) are completely replaced by mature AChRs containing α-subunit. The neuromuscular junction is completely developed at 30 days after birth
- 19. Each ACh receptor in the neuromuscular junction normally consists of five protein subunits; • two α subunits; and • single β, δ, and ε subunits. Only the two identical α subunits are capable of binding ACh molecules. • If both binding sites are occupied by ACh, a conformational change in the subunits briefl y (1 ms) opens an ion channel in the core of the receptor
- 20. Ion channel in the core of the ach receptor Only the two identical α subunits are capable of binding ACh molecules. The channel will not open if ACh binds on only one site. If both binding sites are occupied by ACh, a conformational change in the subunits briefl y (1 ms) opens an ion channel in the core of the receptor
- 22. Voltage-gated sodium channels resulting action potential propagates along the muscle membrane and T-tubule system, opening sodium channels and releasing calcium from the sarcoplasmic reticulum Voltage-gated sodium channels within this portion of the muscle membrane open when a threshold voltage is developed across them When enough receptors are occupied by ACh, the end-plate potential will be sufficiently strong to depolarize the perijunctional membrane. Perijunctional areas of muscle membrane have a higher density of these sodium channels than other parts of the membrane.
- 23. sodium channel is a transmembrane protein that can be conceptualized as having two gates. Sodium ions pass only when both gates are open. Opening of the gates is time dependent and voltage dependent. The channel therefore possesses three functional states. A...At rest, the lower gate is open but the upper gate is closed B...reaches threshold voltage depolarization, the upper gate opens and sodium can pass C...Shortly after the upper gate opens the timedependent lower gate closes
- 25. Fetal or immature extrajunctional ach recepters • another isoform contains a γ subunit instead of the ε subunit. • Th is isoform initially expressed in fetal muscle. • It is also often referred to as extrajunctional because, unlike the mature isoform, it may be located anywhere in the muscle membrane, inside or outside the neuromuscular junction when expressed in adults.
- 26. Steps in normal NM transmission. Sodium and calcium flow through the open receptor channel generating an end- plate potential. Opening receptor channels. Receptors do not open unless both α receptors are occupied by ach Ach molecules bind to the α subunits of the ach receptor on the post junctional membrane, generating A conformational change and Ach is released from storage vesicles at the nerve terminal. Enough ach is released to bind 500,000 receptors. Nerve action potential is transmitted, and the nerve terminal is depolarized.
- 27. Aft er unbinding ACh, the receptors’ ion channels close, permitting the end- plate to repolarize. Calcium is resequestered in the sarcoplasmic reticulum, and the muscle cell relaxes. ACh is rapidly hydrolyzed into acetate and choline by the substrate- specific enzyme acetylcholinesterase . when a threshold voltage is developed across them, a muscle action potential (MAP) is generated When between 5% and 20% of the receptor channels are open and a threshold potential is reached, ....Voltage-gated sodium channels within perijunctional portion of the muscle membrane open
- 28. CLASSIFICATION DISTINCTIONS BETWEEN DEPOLARIZING & NON DEPOLARIZING BLOCKADE (Mechanism of Actions)
- 29. Basis of Classification Mechanism of action Response to peripheral nerve stimulation Reversal of block. Duration of action Chemistry
- 31. Classification-mechanism & duration of action Depolarizing Short-acting • Succinylcholine Nondepolarizing Short-acting • Gantacurium • Mivacurium • Rocuronium Intermediate-acting • Atracurium • Cisatracurium • Vecuronium • Rocuronium Long-acting • Pancuronium • Pipecuronium • Doxacurium
- 32. Classification- Chemistry Benzylisoquinolinium Atracurium Cisatracurium Mivacurium Doxacurium AV002 (CW002) Historical interest • tubocurarine • metocurine • gallamine, • alcuronium, , • decamethonium Steroidal Pancuronium Vecuronium Rocuronium Pipecuronium rapacuronium...historical interest Others- chlorofumarates Gantacurium
- 33. MECHANISM OF ACTION of depolarizing NMBA 1 • Depolarizing muscle relaxants closely resemble ACh and readily bind to ACh receptors, generating a muscle action potential. 2 • Unlike ACh, however, these drugs are not metabolized by acetylcholinesterase, and their concentration in the synaptic cleft does not fall as rapidly, resulting in a prolonged depolarization of the muscle end-plate. 3 • Continuous end-plate depolarization causes muscle relaxation 4 • because opening of perijunctional sodium channels is time limited (sodium channels rapidly “inactivate” with continuing depolarization)
- 34. Phases of block in Depolarizing NMBA Phase-1 block • Perijunctional VGSC cannot reopen until the end- plate repolarizes. • Th e end-plate cannot repolarize as long as the depolarizing muscle relaxant continues to bind to ACh receptors; this is called a phase I block. Phase ii Block • Aft er a period of time, prolonged end-plate depolarization can cause poorly understood changes in the ACh receptor that result in a phase II block,
- 35. Characteristics of Depolarizing Neuromuscular Block In the presence of a small dose of succinylcholine: 1.a decreased response to a single • low-voltage (1 Hz) twitch stimulus applied to a peripheral nerve is detected. 2.Tetanic stimulation (e.g. at 50 Hz) produces a small, but sustained, response 3.if four twitch stimuli are applied at 2 Hz over 2 s (train-of-four stimulus), followed by a 10-s inter-val before the next train-of-four • no decrease in the height of successive stimuli is noted 4.the application of a 5-s burst of tetanic stimula-tion after the application of single twitch stim-uli,…. followed 3 s later by a further run of twitch stimuli • produces no potentiation of the twitch height; there is no post-tetanic potentiation (sometimes termed facilitation)
- 36. neuromuscular block is potentiated by the ad- ministration of an anticholinesterase such as neostigmine or edrophonium. OR if repeated doses of succinylcholine are given, the characteristics of this depolarizing block alter; • signs typical of a non-depolarizing block develop • Initially, such changes are demonstrable only at fast rates of stimulation, • but with further increments of succinylcholine they may occur at slower rates. This phenomenon is termed ‘dual block’. muscle fasciculation is typical of a depolarizing block.
- 38. Mechanism of action of non- depolarizing NMBA depolarizing muscle relaxants act as ACh receptor agonists, whereas nondepolarizing muscle relaxants function as competitive antagonists. Nondepolarizing muscle relaxants bind ACh receptors but are incapable of inducing the conformational change necessary for ion channel opening. Because ACh is prevented from binding to its receptors, no end-plate potential develops. Neuromuscular blockade occurs even if only one α subunit is blocked.
- 40. Characteristics of Non-Depolarizing Neuromuscular Block If a small, subparalysing dose of a non-depolarizing neuromuscular blocking drug is administered, the following characteristics are recognized: 1. decreased response to a low-voltage twitch stimulus (e.g. 1 Hz) which, • if repeated, decreases further in amplitude. This effect, which is in con-trast to that produced by a depolarizing drug, 2.also occurs to a greater degree when the train-of-four (TOF) twitch response is applied, and even more so with higher, tetanic rates of stimulation. It is referred to as ‘fade’ or decrement.
- 41. 3. post-tetanic potentiation (PTP) or facilitation (PTF) of twitch response may be demonstrated 4.neuromuscular block is reversed by administration of ananticholinesterase. 5 no muscle fasciculation is visible.
- 44. OTHER MECHANISMS OF NEUROMUSCULAR BLOCKADE Interference with the function of the Ach receptor without acting as an agonist or antagonist. • Example.... • Inhaled anesthetic agents • local anesthetics • ketamine. Interfere with normal functioning of the Ach receptor binding site or with the opening and closing of the receptor channel.
- 45. • During closed channel blockade • the drug physically plugs up the channel, preventing passage of cations • whether or not ACh has activated the receptor. • Open channel blockade • use dependent, • because the drug enters and obstructs the ACh receptor channel only aft er it is opened by ACh binding • Example...channel block in the laboratory include • neostigmine, • some antibiotics, • cocaine, and • quinidine. closed or open channel blockade Other drugs may impair the presynaptic release of ACh
- 46. MONITORING NEUROMUSCULAR BLOCKADE Indications for Neuromuscular Monitoring….. preferable always to monitor neuromuscular function when a muscle relaxant is used during an- aesthesia • 1.during prolonged anaesthesia, when repeated increments of neuromuscular blocking agents are required • 2.when infusions of muscle relaxants are given ( including in the ICU)
- 47. 3.in the presence of renal or hepatic dysfunction 4. in patients with neuromuscular disorders 5.in patients with a history of sensitivity to a muscle relaxant or poor recovery from block 6.when poor reversal of neuromuscular block is encountered unexpectedly
- 48. AAccelometer
- 49. Nerve Stimulator Characteristics Response of the nerve to electrical stimulation depends on three factors: • The current applied • The duration of the current • The position of the electrodes Black electrode of the stimulator is negatively charged, and the red electrode is positively charged Usually, a nerve which is readily accessible to the anaesthetist • The ulnar • Facial • Common peroneal nerve The muscle response assessed by either • Visual or tactile means, or it may be • more sophisticated methods. • Mechanomyography • Electromyography • Accelerography
- 50. Modes of Stimulation Single stimulus TOF stimulation Tetanic stimulation Posttetanic facilitation and posttetanic count Double-burst (DB) stimulation
- 52. Single twitch stimulus of short duration (0.1–0.2 ms) delivery of single impulses separated by at least 10 seconds. It is of limited clinical use • if applied re-peatedly, before and after a dose of a muscle relaxant, it may be possible to assess the effects of the drug.
- 53. Train-of-Four (TOF) Twitch Response Four stimuli (at 2 Hz) are applied over 2 s, with at least a 10-s gap between each TOF small dose of a non-depolarizing muscle relaxant • fade of the am -plitude of the TOF may be visible. The ratio of the amplitude of the fourth to the first twitch is called the train-of-four ratio (TOFR).
- 54. larger dose of such a drug, • the fourth twitch disappears first, then the third, followed by the second and, finally, the first twitch • On recovery from neuro -muscular block, the first twitch appears first, then the second then the third, and finally the fourth at least three of the four twitches must be absent ……for upper abdominal surgery. Full reversal can only be relied upon if at least the ……second twitch is visible when an anticholinesterase is given.
- 56. After reversal • good muscle tone – as assessed clinically ….being able to cough, raise his or her head from the pillow for at least 5 s, protrude the tongue and have good grip strength – may be anticipated when the TOFR has reached at least 0.7 • TOFR of 0.9 has now been shown to be necessary prior to extubation if the airway is to be protected completely.
- 57. Why Fade ? Fade may be due to a prejunctional efect of nondepolar- izing relaxants • that reduces the amount of ACh in the nerve terminal available for release during stim-ulation (blockade of ACh mobilization). Adequate clinical recovery correlates well with the absence of fade. Because fade is more obvious during • sustained tetanic stimulation or double-burst stimulation than following a train-of-four pattern or repeated twitches, • the first two patterns are the preferred methods for determining adequacy of recovery from a nondepolarizing block.
- 58. Tetanic Stimulation Most sensitive form of neuromuscular stimulation. • Loss of contraction during tetanic stimulation, known as tetanic fade , is a sensitive indicator of residual neuromuscular blockade. Repetitive high-frequency stimulation frequencies of 50–100 Hz are applied to a peripheral nerve to detect even minor degrees of residual neuromuscular block • Tetanic fade may be present when the twitch response is normal. Tetanic rates of stimulation may be applied under Anaesthesia,….. But in the awake patient painful
- 59. Post-Tetanic Potentiation or Facilitation Assess more profound degrees of neuro-muscular block produced by non-depolarizing neuromuscular blocking agents. If a single twitch stimulus is applied to the nerve with little or no neuro-muscular response,…. >But after a 5 s delay a burst of 50-hz tetanus is given for 5 s….,> The effect of a further twitch stimulus 3 s later is enhanced Profound block, ….The effect of repeated single twitches applied after the tetanus until the response disappears can be counted; this is termed the …..Post-tetanic count • The number of twitches observed is inversely related to the degree of blockade.
- 61. Why postte-tanic potentiation ? ability of tetanic stimulation during a par- tial nondepolarizing block to increase the evoked response to a subsequent twitch is termed postte-tanic potentiation. Due to a transient increase in ACh mobilization following tetanic stimulation
- 62. Double-Burst Stimulation (DBS) More accurate assessment of residual block by visual or tactile means than fade of the TOF response Application of two or three short bursts of 50-hz tetanus,…. Each comprising two or three impulses ….Separated by a 750-ms interval. ……Each impulse lasts for 0.2 ms
- 63. Three short (0.2 ms) high- frequency stimulations separated by a 20-ms interval (50 Hz) and followed ……750 ms later by • two (DBS 3,2 ) or • three (DBS 3,3 ) additional impulses.
- 64. Recording the Response 1. Visual and tactile evaluation • is the easiest and least expensive way to assess the response to electrical stimulation applied to a peripheral nerve • The disadvantage of this technique is the • subjective nature of its interpretation (present or absent, weak or strong)
- 65. 2. Measurement of force-Mechanomyography • using a force transducer provides accurate assessment (quantitative or objective) of the response elicited by electrical stimulation of a peripheral nerve. 3. Electromyography • measures the electrical rather than mechanical response of the skeletal muscle. 4. Accelerometry devices • are usually attached to the thumb • a digital readout is obtained • The use of accelerometry is helpful in the diagnosis of residual paralysis
- 66. Choice of Muscle Muscles do not respond in a uniform fashion to NMBAs…..differences in • time to onset • maximum blockade • duration of action muscles of physiologic importance • abdominal muscles during surgery • upper airway muscles postoperatively • A common strategy is to monitor one site adductor pollicis…Usually
- 67. 1. Adductor pollicis muscle • Supplied by the ulnar nerve • This muscle is relatively sensitive to nondepolarizing muscle relaxants(blocked SOONER than respiratory) • During recovery, it is blocked more than some respiratory muscles such as the diaphragm and laryngeal adductors(recover LATE than respiratory) 2. Muscles surrounding the eye • Innervated by the facial nerve • A. The response of the orbicularis oculi over the eyelid is similar to that of the adductor pollicis. • B. The response the eyebrow (corrugator supercilii) parallels the response of the laryngeal adductors. • (Onset is more rapid and recovery is sooner than at the adductor pollicis.) This response is useful for predicting intubating conditions.
- 68. Clinical Applications 1. Monitoring Onset. • After induction ,determine the time for tracheal intubation • (maximum relaxation of laryngeal and respiratory muscles). • Single-twitch stimulation is often used to monitor the onset of neuromuscular blockade. 2. Monitoring Surgical Relaxation • Adequate surgical relaxation is usually present when fewer than 2 or 3 visible twitches of the TOF are observed in response to stimulation of the adductor pollicis muscle
- 69. 3. Monitoring Recovery. • Complete return of neuromuscular function should be achieved before extubation • Respiratory and upper airway function does not return to normal unless the TOF ratio at the adductor pollicis muscle is ≥0.9. • Anticholinesterase agents should be given only when four twitches are visible • The presence of spontaneous breathing is not a sign of adequate neuromuscular recovery. • (The diaphragm recovers earlier than upper airway muscles that recover in parallel with the adductor pollicis muscle.) • the visual or tactile evaluation of TOF response is not reliable for ruling out residual blockade
- 71. SUCCINYLCHOLINE Succinylcholine quaternary ammonium compound—also called diacetylcholine or suxamethonium— • consists of two joined ACh molecules only depolarizing relaxant now available in clinical practice is succinylcholine. • Decamethonium was used clinically in the UK for many years
- 74. Mechanism of action Depolarizing muscle relaxants very closely resemble ACh and readily bind to ACh receptors, generating a muscle action potential Phase i block Phase ii block
- 75. Metabolism & Excretion Rapid onset of action (30–60 s) and • Small volume of distribution due to its very low lipid solubility • Relative overdose that is usually administered. Short duration of action (usually less than 10 min). In circulation.....Rapidly metabolized by pseudocholinesterase into succinylmonocholine. • 10% of the drug is excreted in the urine; there is very little metabolism in the liver although some breakdown by non- specific esterases occurs in the plasma.
- 76. Causes of prolonged effect of Suxamethonium Limited duration of action....Recovery from neuromuscular block may start to occur within 3 min and is complete within 12–15 min. • Drug levels fall in blood, succinylcholine molecules diffuse away from the neuromuscular junction Can be prolonged by • High doses • Infusion of succinylcholine • Abnormal metabolism • Hypothermia, • Reduced pseudocholinesterase levels, • Genetically aberrant enzyme
- 77. Decreased level of pseudocholinesterase Reduced pseudocholinesterase levels...Generally produce only modest prolongation of succinylcholine’s actions (2–20 min). • Pregnancy, • Liver disease, • Renal failure, and • Carcinomatosis and starvation, • Also because of reduced enzyme synthesis • Hypothyroidism., • Cardiopulmonary bypass • Plasmapheresis Certain drug therapies • Echothiophate......Organophosphate use for glaucoma • Neostigmine ,pyridostigmine....Cholinesterase inhibitors • Phenelzine.....Monoamine oxidase inhibitor • Cyclophosphamide....Anti neoplastic • Metoclopramide...Antiemetic & prokinetic • Esmolol...Beta blocker • Pancuronium....Non depolarizing nmba • Oral contraceptives
- 78. Inherited factors atypical/abnormal pseudocholinesterse Structure of plasma cholinesterase is determined genetically, by autosomal genes, 1.Heterozygote for the atypical gene • One in 25-30 patients of european extraction is a heterozygote with one normal and one abnormal (atypical) pseudocholinesterase gene, resulting in a slightly prolonged block (20–30 min) 2.Homozygous atypical pseudocholinesterse gene.....1 in 3000 patients have two copies of the abnormal gene (homozygous atypical) that produce an enzyme with little or no affinity for succinylcholine. • Will have a very long blockade eg, 4–8 h
- 79. Types of Homozygous Pseudocholinesterse 1.The dibucaine-resistant (variant) allele • Which produces an enzyme with 1/100 of normal affinity for succinylcholine, is the most common. 2.Fluoride-resistant 3.Silent (no activity) alleles.
- 80. Measurement of Atypical Pseudocholinesterse 1.Qunatitative....determined in the laboratory quantitatively in units per liter (a minor factor) 2.Qualitative.......qualitatively by dibucaine number (the major factor)
- 81. Dibucaine Number Dibucaine, a local anesthetic, inhibits normal pseudocholinesterase activity by 80%, but inhibits atypical enzyme activity by only 20%. Serum from an individual who is heterozygous for the atypical enzyme is characterized by an intermediate 40% to 60% inhibition percentage of inhibition of pseudocholinesterase activity is termed the dibucaine number
- 82. Method for detecting structurally abnormal cholinesterase. Dibucaine is also added to the water bath, this reaction is inhibited; no light is produced. The percentage inhibition is referred to as the dibucaine number 1.Normal plasma cholinesterase has a high dibucaine number of 77–83. 2.A heterozygote for the atypical gene has a dibucaine number of 45–68 3.In a homozygote, the dibucaine number is less than 30. A chemical reaction occurs with plasma cholinesterase, emitting light of a given wavelength, which may be detected spectrophotometrically. Plasma from a patient of normal is added to a water bath containing a substrate such as benzoylcholine
- 83. When plasma sample should be taken? Plasma cholinesterase activity is reduced by the presence of succinylcholine, a plasma sample to measure the patient’s cholinesterase activity should not be taken for several days after prolonged block has been experienced, by which time new enzyme has been synthesized.
- 84. Detection of geno type of Atypical Pseudocholinesterse ? If there is no reaction in the presence of the substrate only,....... the silent gene is present. If fluoride is added to the solution instead of dibucaine, the ....fluoride gene may be detected plasma from a patient is added to a water bath containing a substrate such as benzoylcholine
- 85. Management of succinylcholine Apnoea This condition is not life-threatening, but the risk of awareness is considerable • especially after the end of surgery, when the anaesthetist, who may not yet have made the diagnosis, is attempting to waken the patient. Anaesthesia must be continued until full recovery from neuromuscular block is demonstrable. • In such patients, non-specific esterases(10% metabolism) gradually clear the drug from plasma. source of cholinesterase, such as fresh frozen plasma, should be administered
- 86. patient who is found to have reduced enzyme activity and structurally abnormal enzyme should be given a warning card or alarm bracelet monitor neuromuscular transmission accurately, until full recovery from residual neuromuscular block. Prolonged paralysis from succinylcholine caused by abnormal pseudocholinesterase (atypical cholinesterase) should be treated with continued mechanical ventilation and sedation until muscle function returns to normal by clinical signs. plasma sample should be taken..... Quantitative & Qualitave measurements of Atypical cholinesterase
- 88. Drug interaction sepcial considerations 1.Cholinesterase Inhibitors……markedly prolong a depolarizing phase I block by two mechanisms. • 1. inhibiting acetylcholinesterase....higher ACh concentration at the nerve terminal, which intensifies depolarization • 2.inhibiting pseudocholinesterase....reduce the hydrolysis of succinylcholine Example • Organophosphate pesticides, for ......irreversible inhibition of acetylcholinesterase and can prolong the action of succinylcholine by 20–30 min. • Echothiophate eye drops......can markedly prolong succinylcholine
- 89. 2. Nondepolarizing Relaxants small doses of nondepolarizing relaxants • antagonize a depolarizing phase I block. ....drugs occupy some ACh receptors,.....so • partial prevention of depolarization by succinylcholine If enough depolarizing agent is administered...... to develop a phase II block, • then a nondepolarizer will potentiate paralysis.
- 90. Dosage & Storage usual adult dose of succinylcholine for intubation is 1–1.5 mg/kg intravenously. • Doses as small as 0.5 mg/kg will oft en provide acceptable intubating conditions if a defasciculating dose of a nondepolarizing agent is not used. Repeated small boluses (10 mg) or a succinylcholine drip (1 g in 500 or 1000 mL, titrated to eff ect) can be used during surgical procedures that require brief but intense paralysis • ENT procedures...endoscopy • Neuromuscular function should be frequently monitored with a nerve stimulator to prevent overdosing and to watch for phase II block.
- 91. Pediatric patients are often need greater than for adults..... • Suxamethonium not lipid soluble & infants and neonates have a larger extracellular space than adults Intramuscularly to children • A dose as high as 4–5 mg/kg does not always produce complete paralysis. Storage... • Stored under refrigeration (2–8°C), and should be used within 14 days after removal from refrigeration and exposure to room temperature.
- 92. Side Effects & Clinical Considerations Succinylcholine is still useful for rapid sequence induction and for short periods of intense paralysis succinylcholine is considered relatively contraindicated in the routine management of children and adolescent patients...undiagnosed myopathies Most clinicians have also abandoned the routine use of succinylcholine for adults
- 94. 1.Cardiovascular Suxamethonium acts cholinergic ach receptors in addition to those at the neuromuscular junction • Entire parasympathetic nervous system and • Parts of the sympathetic nervous system • Sympathetic ganglions • Adrenal medulla • Sweat glands
- 95. Stimulation of nicotinic receptors in parasympathetic and sympathetic ganglia, and muscarinic receptors in the sinoatrial node of the heart......complex effects increase or decrease blood pressure and heart rate. Low doses of succinylcholine can produce negative chronotropic and inotropic effects higher doses usually increase heart rate and contractility and elevate circulating catecholamine levels
- 96. Children are particularly susceptible to profound bradycardia following administration of succinylcholine. in adults Bradycardia will sometimes occur when a second bolus of succinylcholine is administered approximately 3–8 min after the first dose • succinylmonocholine, sensitizes muscarinic cholinergic receptors in the sinoatrial node • Intravenous atropine (0.02 mg/kg in children, 0.4 mg in adults) is normally given prophylactically to children prior to the first and subsequent doses in adults. arrhythmias.....nodal bradycardia and ventricular ectopy
- 97. B. Fasciculations • Visible motor unit contractions called fasciculation Onset of paralysis by succinylcholine..... • Pretreatment with a small dose of nondepolarizing relaxant...Then Prevented by • (1.5 mg/kg) Larger dose of succinylcholine is required • Young children and • Elderly patients. Not observed in
- 98. C. Hyperkalemia • to increase serum potassium by 0.5 mEq/L. • insignificant in patients with normal baseline potassium levels • can be life- threatening in patients with preexisting hyperkalemia. succinylcholine- induced depolarization • can prove to be quite refractory to routine cardiopulmonary resuscitation • requiring calcium, insulin, glucose, bicarbonate, and even cardiopulmonary bypass Hyperkalemic cardiac arrest
- 99. Conditions causing susceptibility to succinylcholine-induced hyperkalemia Burn injury Massive trauma Severe intraabdominal infection Spinal cord injury Encephalitis Stroke Guillain-Barré syndrome Severe Parkinson’s disease Tetanus Prolonged total body immobilization Ruptured cerebral aneurysm Polyneuropathy Closed head injury Hemorrhagic shock with metabolic acidosis Myopathies (eg, Duchenne’s dystrophy)
- 101. Mechanism of hyperkalemia succinylcholine to effect widespread depolarization and extensive potassium release. Life-threatening potassium release is not reliably prevented by pretreatment with a nondepolarizer risk of hyperkalemia usually seems to peak in 7–10 days following the injury risk of hyperkalemia from succinylcholine is minimal in the fi rst 2 days after spinal cord or burn injury. Immature isoform of the Ach receptor may be expressed inside and outside the neuromuscular junction (up-regulation). Denervation injuries (spinal cord injuries, larger burns)
- 103. D. Muscle Pains • Rocuronium (0.06–0.1 mg/kg) prior to succinylcholine has been reported to be effective Increased incidence of postoperative myalgia…..Prevention by • Myoglobinemia and increases in serum creatine kinase can be detected following administration of succinylcholine Myalgias are theorized to be due to the initial unsynchronized contraction of muscle groups • Use of nonsteroidal antiinfl ammatory drugs may reduce the incidence and severity of myalgias. Treatment
- 104. E. Intragastric Pressure Elevation Abdominal wall muscle fasciculations offset by an increase in lower esophageal sphincter tone. no evidence that the risk of gastric reflux or pulmonary aspiration is increased by succinylcholine
- 105. F. Intraocular Pressure Elevation Extraocular muscle.....multiple motor end-plates on each cell. Prolonged membrane depolarization and contraction of extraocular muscles transiently raise intraocular pressure and theoretically could compromise an injured eye • no evidence that succinylcholine leads to worsened outcome in patients with “open” eye injuries Prevention • not always prevented by pretreatment with a nondepolarizing agent.
- 106. G. Masseter Muscle Rigidity • Some difficulty .... In opening the mouth Transiently increases muscle tone in the masseter muscles. • Premonitory sign of malignant hyperthermia Marked increase in tone preventing laryngoscopy is abnormal .......
- 107. H. Malignant Hyperthermia Acute hypermetabolic disorder of skeletal muscle..... • Pharmacogenetic pathology • Potent volatile anaesthetics with suxamethonium Succinylcholine is a potent triggering agent in patients susceptible no need to avoid use of succinylcholine in patients with NMS.
- 108. I. Generalized Contractions Patients afflicted with myotonia may develop myoclonus after administration of succinylcholine. Patients with reduced levels of normal pseudocholinesterase may have a longer than normal duration of action, Whereas patients with atypical pseudocholinesterase will experience markedly prolonged paralysis.
- 109. J. Prolonged Paralysis Patients with reduced levels of normal pseudocholinesterase may have a longer than normal duration of action, Whereas patients with atypical pseudocholinesterase will experience markedly prolonged paralysis.....Sux. apnea
- 110. K. Intracranial Pressure Succinylcholine may lead to an activation of the electroencephalogram Slight increases in cerebral blood flow and intracranial pressure Fasciculations stimulate muscle stretch receptors, which subsequently increase cerebral activity.
- 111. Prevention • Increase in intracranial pressure can be attenuated by maintaining good airway control and instituting hyperventilation. • Pretreating with a nondepolarizing muscle relaxant • Administering intravenous lidocaine (1.5–2.0 mg/kg) 2–3 min prior to intubation. Succinylcholine is NOT contraindicated for rapid sequence induction of patients with intracranial mass lesions or other causes of increased intracranial pressure....If benefits overweights
- 112. L. Histamine Release Slight increase in histamine after suxamethonium administration
- 114. 1.Unique Pharmacological Characteristics classified as • benzylisoquinolinium, • steroidal, or other compounds. In general, steroidal compounds can be vagolytic, but this property is most notable with pancuronium Benzylisoquinolines tend to release histamine Because of structural similarities, an allergic history to one muscle relaxant strongly suggests the possibility of allergic reactions to other muscle relaxants, particularly those in the same chemical class.
- 115. A. Suitability for Intubation None of the currently available nondepolarizing muscle relaxants equals succinylcholine onset of nondepolarizing relaxants can be quickened by using • either a larger dose or • a priming dose. ED 95 of any drug ....is the eff ective dose of a drug in 95% of individuals But for neuromuscular blockers ED95 is.... the dose that produces 95% twitch depression in 50% of individuals.
- 116. larger intubating dose speeds onset, it exacerbates side eff ects and prolongs the duration of blockade. • For example, a dose of 0.15 mg/kg of pancuronium may produce intubating conditions in 90 sec, but at the cost of more pronounced tachycardia—and a block that may be irreversible (by neostigmine) for more than 60 min
- 117. Why potent NMBA has slow onset of action? What is priming dose ? General rule,..... The more potent the nondepolarizing muscle relaxant, the slower its speed of onset • More the no. Of molecules available at receptors for effect …..More rapid onset • Less number of molecules required will be available at receptors to get the response…..In case of potent drug Priming doses...Giving 10% to 15% of the usual intubating dose 5 min before induction will occupy enough receptors so that paralysis will quickly follow when the balance of relaxant is administered. • Can produce conditions suitable for intubation as soon as 60 sec following administration of rocuronium or 90 sec following administration of other intermediate-acting nondepolarizers
- 118. Priming dose.....Not usually lead to clinically significant paralysis, which requires that 75% to 80% of the receptors be blocked (a neuromuscular margin of safety). Side effects of priming dose... • Distressing dyspnea, diplopia, or dysphagia; • In such instances, the patient should be reassured • Induction of anesthesia should proceed without delay. • Oxygen desaturation in patients with marginal pulmonary reserve Muscle groups vary in their sensitivity to muscle relaxants..Laryngeal muscle recover first
- 119. B. Suitability for Preventing Fasciculations To prevent fasciculations and myalgias, 10% to 15% of a nondepolarizer intubating dose.........5 min before succinylcholine. Shortly before succinylcholine, myalgias, but not fasciculations, will be inhibited. Tubocurarine and rocuronium have been most popular for precurarization
- 120. C. Maintenance Relaxation Following intubation, muscle paralysis may need to be maintained • To facilitate surgery, (eg, abdominal operations), • To permit a reduced depth of anesthesia, • To control ventilation Prevention of over- and under dosing ...... to reduce the likelihood of serious residual muscle paralysis in the recovery room... Use nerve stimulator for monitoring neuromuscular function Techniques of maintenance doses...Should be guided by the nerve stimulator and clinical signs • Intermittent boluses or • Continuous infusion
- 121. D. Potentiation by Inhalational Anesthetics Volatile agents decrease nondepolarizer dosage requirements by at least 15% Postsynaptic augmentation depends on • Inhalational anesthetic (desflurane > sevofl urane > isofl urane and enfl urane > halothane > N 2 O/O 2 / narcotic) • Muscle relaxant employed (pancuronium > vecuronium and atracurium)
- 122. E. Potentiation by Other Nondepolarizers Synergistic • combinations of nondepolarizers produce a greater than additive (synergistic) neuromuscular blockade. Additive • Th e lack of synergism (ie, the drugs are only additive) by closely related compounds (eg, vecuronium and pancuronium)
- 123. F. Autonomic Side Effects Nondepolarizers differ in their relative effects on nicotinic and muscarinic cholinergic receptors. Autonomic ganglion blockade • Reducing the ability of the sympathetic nervous system to increase heart contractility and rate in response to hypotension and other intraoperative stresses....Eg,tubocurarine and, to a lesser extent, metocurine Block vagal muscarinic receptors in the sinoatrial node.... • Tachycardia.Eg,pancuronium Newer nondepolarizing relaxants, including atracurium, cisatracurium, vecuronium, and rocuronium, are devoid of significant autonomic effects
- 124. G. Histamine Release Histamine release from mast cells • bronchospasm • skin flushing • hypotension atracurium and mivacurium are capable of triggering histamine release, particularly at higher doses Prevention • Slow injection rates • H 1 and H 2 antihistamine pretreatment
- 125. H. Hepatic Clearance Only pancuronium and vecuronium are metabolized to any significant degree by the liver. • Active metabolites likely contribute... clinical effect. Vecuronium and rocuronium depend heavily on biliary excretion. liver failure • prolongs pancuronium and rocuronium blockade • less eff ect on vecuronium, • no eff ect on pipecuronium. Extra hepatic metabolism • Atracurium,cisatracurium &mivacurium, although extensively metabolized, depend on extrahepatic mechanisms Severe liver disease....decrease in pseudocholinesterase levels may slow the metabolism of mivacurium.
- 126. I. Renal Excretion Action is prolonged in patients with renal failure...... • Doxacurium, pancuronium, vecuronium, and pipecuronium are partially excreted by the kidneys, Independent of kidney function. • Elimination of atracurium, cisatracurium, mivacurium, and rocuronium
- 129. 2.General Pharmacological Characteristics of Non depolarizing MNBA
- 130. A. Temperature Hypothermia prolongs blockade by 1.decreasing metabolism (eg, mivacurium, atracurium, and cisatracurium) and 2.delaying excretion (eg, pancuronium and vecuronium).
- 131. B. Acid–Base Balance Respiratory acidosis potentiates the blockade of most nondepolarizing relaxants and antagonizes its reversal. due to coexisting alterations in extracellular pH, intracellular pH, electrolyte concentrations, or structural diff erences between drugs
- 132. C. Electrolyte Abnormalities Hypokalemia and hypocalcemia ....augment a nondepolarizing block. Th e responses with hypercalcemia are ......unpredictable. Hypermagnesemia..... potentiates a nondepolarizing blockade by competing with calcium at the motor end-plate.
- 133. D. Age Neonates have an increased sensitivity to nondepolarizing relaxants because of their immature neuromuscular junctions does not necessarily decrease dosage requirements, as the neonate’s greater extracellular space provides a larger volume of distribution.
- 134. Additional considerations in special populations.
- 135. E. Drug Interactions many drugs augment nondepolarizing blockade multiple sites of interaction: prejunctional structures postjunctional cholinergic receptors muscle membranes
- 137. F. Concurrent Disease neurological or muscular disease can have profound eff ects on an individual’s response to muscle relaxants Cirrhotic liver disease and chronic renal failure increased volume of distribution and a lower plasma concentration for a given dose of water- soluble drugs, such as muscle relaxants drugs dependent on hepatic or renal excretion may demonstrate prolonged clearance greater initial (loading) dose—but smaller maintenance doses
- 139. G. Muscle Groups The onset and intensity of blockade vary among muscle groups. differences in blood flow, distance from the central circulation, or different fiber types. choice of muscle relaxant. diaphragm, jaw, larynx, and facial muscles (orbicularis oculi) respond to and recover from muscle relaxation sooner than the thumb. Glottic musculature is also quite resistant to blockade, as is often confirmed during laryngoscopy. intubating conditions are usually associated with visual loss of the orbicularis oculi twitch response. However...Wide variability in sensitivity to nondepolarizing muscle relaxants is oft en encountered in clinical practice
- 142. ATRACURIUM Physical structure • Atracurium has a quaternary group Benzylisoquinoline structure • Is responsible for its unique method of degradation. Hofmann degradation may be considered as a ‘safety net’ in the sick patient with impaired liver or renal function • A mixture of 10 stereoisomers.
- 143. Metabolism & Excretion Extensively metabolized …automatic degradation….Ph & temperature dependent Pharmacokinetics are independent of renal and hepatic function Less than 10% is excreted unchanged by renal and biliary routes.
- 144. Two separate processes are responsible for metabolism A. Ester Hydrolysis • nonspecifi c esterases, not by acetylcholinesterase or pseudocholinesterase B. Hofmann Elimination • spontaneous nonenzymatic chemical breakdown occurs at • physiological pH and • temperature.
- 145. Dosage & Storage Onset....2.0 - 2.5 mins Intubation • 0.5 mg/kg ...intravenously for intubation After succinylcholine, intraoperative relaxation • 0.25 mg/kg initially, then • in incremental doses of 0.1 mg/kg every 10–20 min infusion • 5–10 mcg/kg/min can effectively replace intermittent boluses. Storage & availability • available as a solution of 10 mg/ mL • It must be stored at 2–8°C • loses 5% to 10% of its potency for each month it is exposed to room temperature. • At room temperature, it should be used within 14 days
- 146. Side Effects & Clinical Considerations Dose-dependent histamine release ...Significant at doses above 0.5 mg/kg. 1.Hypotension and tachycardia • Unusual unless doses in excess of 0.5 mg/kg • Transient drop in systemic vascular resistance and • Increase in cardiac index independent of any histamine release. • Prevention • A slow rate of injection minimizes these eff ects.
- 147. 2.Bronchospasm • Avoided in asthmatic patients. • Severe bronchospasm is occasionally seen in patients without a history of asthma 3.Laudanosine toxicity • Tertiary amine, is a breakdown product of atracurium’s hofmann elimination • Associated with central nervous system excitation, • Resulting in elevation of the minimum alveolar concentration • Precipitation of seizures. • Laudanosine is metabolized by the liver and excreted in urine and bile.
- 148. 4.Temperature and pH Sensitivity • Hoffman degredation... pH & temperature dependant • duration of action can be markedly prolonged by hypothermia and to a lesser extent by acidosis. 5.Chemical Incompatibility • Atracurium will precipitate as a free acid if it is introduced into an intravenous line containing an alkaline solution such as thiopental.
- 149. 6.Allergic Reactions • Histamine release....local wheal and flare around the injection site • Anaphylactoid reactions ... but rare • Proposed mechanisms include • direct immunogenicity • acrylate-mediated immune activation. • IgE-mediated antibody reactions directed against substituted ammonium compounds...muscle relaxants, • Reactions to acrylate, a metabolite of atracurium and a structural component of some dialysis membranes
- 150. CISATRACURIUM Physical Structure • Cisatracurium is a stereoisomer of atracurium • four times more potent. • Atracurium contains approximately 15% cisatracurium.
- 151. Metabolism & Excretion • Hofmann elimination .... • degradation in plasma at physiological pH and temperature …. organ-independent . • metabolites (a monoquaternary acrylate and laudanosine) have no neuromuscular blocking eff ects • Nonspecific esterases are not involved in the metabolism of cisatracurium. • Metabolism and elimination are independent of renal or liver failure.
- 152. Dosage & Storage • intubating dose .......0.1–0.15 mg/kg within 2 min and results in muscle blockade of intermediate duration. • maintenance infusion rate ranges from 1.0–2.0 mcg/kg/min. • Refrigeration (2–8°C) • used within 21 days after removal from refrigeration and exposure to room temperature.
- 153. Side Eff ects & Clinical Considerations • does not produce a consistent, dose- dependent increase in plasma histamine levels • does not alter heart rate or blood pressure, nor does it produce autonomic effects • Cisatracurium shares with atracurium the • production of laudanosine, • pH and temperature sensitivity & chemical incompatibility.
- 154. ROCURONIUM Physical Structure • monoquaternary steroid • analogue of vecuronium rapid onset of action. 6-8 times less potent than vecuronium but has approximately the same molecular weight....... • greater number of drug molecules may reach the postjunctional receptors within the first few circulations.......faster development of neuromuscular block
- 155. Metabolism & Excretion….. • no metabolism and is eliminated primarily by the liver and slightly by the kidneys. Duration of action.... • prolonged by severe hepatic failure and pregnancy • Elderly patients may experience a prolonged duration of action due to decreased liver mass. • Not significantly affected by renal disease • does not have active metabolites....better choice than vecuronium in the patient requiring prolonged infusions in the intensive care unit
- 156. Dosage • Rocuronium is less potent than most other steroidal muscle relaxants (potency seems to be inversely related to speed of onset) • for intubation........0.45–0.9 mg/kg intravenously and 0.15 mg/kg boluses for maintenance. • A lower dose of 0.4 mg/kg may allow reversal as soon as 25 min after intubation. • Intramuscular rocuronium (1 mg/kg for infants; 2 mg/kg for children) .....for intubation ...after 3–6 min..... can be reversed aft er about 1 hr. • infusion requirements for rocuronium range from 5–12 mcg/kg/min.
- 157. Side Effects & Clinical Considerations • Rocuronium (at a dose of 0.9–1.2 mg/kg) has an onset of action that approaches succinylcholine (60–90 s), making it a suitable • alternative for rapid-sequence inductions, but at the cost of a much longer duration of action • Rocuronium (0.1 mg/kg) has been shown to be a rapid (90 s) and effective agent ) for precurarization prior to administration of succinylcholine • decreased fasciculations and postoperative myalgias • drug stimulates little histamine release or cardiovascular disturbance, although in high doses it has a mild vagolytic property • Anaphylactic reactions are more common after rocuronium than after any other aminosteroid neuromuscular blocking drug. ...at a similar rate to anaphylactic reactions to atracurium and mivacurium.
- 158. PANCURONIUM Physical Structure • steroid ring on which two modifi ed ACh molecules are positioned (a bisquaternary relaxant). Metabolism & Excretion • metabolized (deacetylated) by the liver to a limited degree. • Its metabolic products have some neuromuscular blocking activity. • Excretion is primarily renal (40%), although some of the drug is cleared by the bile (10%)
- 159. renal failure...... • elimination of pancuronium is slowed and neuromuscular blockade is prolonged cirrhosis....... • may require a larger initial dose due to an increased volume of distribution but have reduced maintenance requirements because of a decreased rate of plasma clearance.
- 160. Dosage • intubation..... 0.08–0.12 mg/kg of pancuronium provides adequate relaxation in 2–3 min. • Intraoperative relaxation .... 0.04 mg/kg initially followed every 20–40 min by 0.01 mg/kg. Storage • available as a solution of 1 or 2 mg/mL • stored at 2–8°C but • stable for up to 6 months at normal room temperature.
- 161. Side Effects & Clinical Considerations A. Hypertension and Tachycardia • vagal blockade • sympathetic stimulation. • ganglionic stimulation, • catecholamine release from adrenergic nerve endings • decreased catecholamine reuptake Large bolus doses of pancuronium.....caution to patients in whom an increased heart rate would be particularly detrimental • (eg, coronary artery disease, hypertrophic cardiomyopathy, aortic stenosis)
- 162. B. Arrhythmias • ventricular arrhythmias...due to • Increased atrioventricular conduction and • catecholamine release • pancuronium, tricyclic antidepressants and halothane...arrhythmogenic C. Allergic Reactions • hypersensitive to bromides may exhibit allergic reactions to pancuronium (pancuronium bromide).
- 163. VECURONIUM Physical Structure • pancuronium minus a quaternary methyl group (a monoquaternary relaxant). • alters side effects without affecting potency. Metabolism & Excretion • metabolized to a small extent by the liver. excretion...... • primarily on biliary excretion and secondarily (25%) on renal shorter elimination half-life and more rapid clearance compared with pancuronium
- 164. Long-term administration in ICU.....prolonged neuromuscular blockade (up to several days) • from accumulation of its active 3-hydroxy metabolite, changing drug clearance, and in some patients..... polyneuropathy. • Risk factors ۔۔۔gender, renal failure, long-term or high-dose corticosteroid therapy, and Tolerance to non depolarizing muscle relaxants can also develop after long term use. Dosage • equipotent with pancuronium, and the intubating dose is 0.08–0.12 mg/kg. • maintenance of relaxation.40.0۔۔ mg/kg initially followed by increments of 0.01 mg/kg every 15–20 min provides intraoperative relaxation. • infusion of 1–2 mcg/kg/min produces good
- 165. Women seem to be approximately 30% more sensitive than men to vecuronium, .....(this has also been seen with pancuronium and rocuronium). • cause .......gender-related diff erences in fat and muscle mass, protein binding, volume of distribution, or metabolic activity. Side Effects & Clinical Considerations • 1.Cardiovascular • No significant cardiovascular effects. • Potentiation of opioid-induced bradycardia . • 2.Liver Failure • dependent on biliary excretion, • duration of action of vecuronium is usually not signifi cantly prolonged in patients with cirrhosis unless doses greater than 0.15 mg/kg are given.
- 168. Gantacurium New class of nondepolarizing neuromuscular blockers called chlorofumarates. It is provided as a lyophilized powder, because it is not stable as an aqueous solution ultrashort duration of action, similar to that of succinylcholine. undergoes nonenzymatic degradation by two chemical mechanisms: • rapid formation of inactive cysteine adduction product and • ester hydrolysis
- 169. Dosage • dose of 0.2 mg/kg (ED 95 ), the onset of action has been estimated to be 1-2 min, with a duration of blockade similar to that of succinylcholine. Its clinical duration of action ranged from 5-10 min; recovery can be accelerated by • edrophonium • exogenous cysteine. Cardiovascular effects • histamine release were observed following the use of three times the ED 95 dosage.
- 170. AV002 (CW002) is another investigational nondepolarizing agent. It is a benzylisoquinolinium fumarate ester-based compound intermediate duration of action metabolism and elimination similar to that of gantacurium.
- 171. OTHER RELAXANTS (Historical interest) no longer manufactured or not clinically used Tubocurarine • the first muscle relaxant used clinical • Histamine release • produce or exacerbate bronchospasm • often produced hypotension and tachycardia through histamine release • ability to block autonomic ganglia . • Tubocurarine is not metabolized significantly, • elimination is primarily renal and secondarily biliary.
- 172. Metocurine • shares many of the side effects of tubocurarin • primarily dependent on renal function for elimination. • Patients allergic to iodine (eg, shellfish allergies) could exhibit hypersensitivity to metocurarine.... contain iodide. Gallamine • the most potent vagolytic properties of any relaxant, • entirely dependent on renal function for elimination. Alcuronium • long-acting nondepolarizer • mild vagolytic properties • primarily dependent on renal function for elimination Rapacuronium • has a rapid onset of action, • minimal cardiovascular side eff ects, and a • short duration of action. • withdrawn by the manufacturer following multiple reports of serious bronchospasm, Histamine release may have been a factor.
- 173. Decamethonium • An older depolarizing agent Mivacurium • Benzylisoquinolinium derivative, • Metabolized by pseudocholinesterase • Duration of action may be prolonged in pathophysiological states that result in low pseudocholinesterase levels. • Intubating dose is 0.2 mg/kg, ... infusion rate being 4-10 mcg/kg/ min. • Releases histamine to about the same degree as atracurium; the • Cardiovascular effects can be minimized by slow injection. • Mivacurium is useful particularly for surgical procedures requiring muscle relaxation in which even atracurium and vecuronium seem too long-acting, and when it is desirable to avoid the side-effects of succinylcholine, tonsillectomy • E.G. For bronchoscopy, oesophagoscopy, laparoscopy or tonsillectomy
- 174. Doxacurium • Potent long-acting benzylisoquinolinium compound • Primarily eliminated by renal excretion. • Intubating conditions are achieved in 5 min with 0.05 mg/ kg. • Devoid of cardiovascular and histamine-releasing side eff ects. Pipecuronium • A bisquarternary steroidal compound similar to pancuronium • Without the vagolytic eff ects. • Onset and duration of action are also similar to pancuronium; • Elimination is primarily through renal (70%) and biliary (20%) excretion. • Intubating dose ranges from 0.06-0.1 mg/kg
- 175. REVERSAL AGENTS Cholinesterase Inhibitors & Other Pharmacologic Antagonists to Neuromuscular Blocking Agents
- 176. Anticholinesterases Inhibit the action of acetylcholinesterase at the neuromuscular junction, • Thus prolonging the half-life of acetylcholine and potentiating its effect, especially in the presence of residual amounts of non-depolarizing muscle relaxant at the end of surgery. The primary clinical use of cholinesterase inhibitors, also called anticholinesterases, is to reverse nondepolarizing muscle blockade. Some of these agents are also used to diagnose and treat myasthenia gravis. Newer agents, such as cyclodextrins and cysteine, with superior ability to reverse neuromuscular blockade from specific agents, are being investigated
- 177. Cholinergic Pharmacology cholinergic .....effects of the neurotransmitter acetylcholine • as opposed to the adrenergic eff ects of nor adrenaline (norepinephrine). Synthesis & metabolism of ACh • Acetylcholine is synthesized in the nerve terminal by the enzyme cholineacetyltransferase, which catalyzes the reaction between acetylcoenzyme A and choline • Aft er its release, acetylcholine is rapidly hydrolyzed by acetylcholinesterase (true cholinesterase) into acetate and choline. Acetylcholine is the neurotransmitter for • the entire parasympathetic nervous system (parasympathetic ganglions and effector cells), • parts of the sympathetic nervous system (sympathetic ganglions, adrenal medulla, and sweat glands), • some neurons in the central nervous system, and • somatic nerves innervating skeletal muscle
- 179. Cholinergic receptors subdivided...... based on their reaction to the alkaloids muscarine and nicotine 1.Nicotine stimulates the…nicotinic receptors • autonomic ganglia and • skeletal muscle receptors (nicotinic receptors) 2. muscarine activates end-organ eff ector cells....muscarinic receptors • bronchial smooth muscle, • salivary glands, and the • sinoatrial node (muscarinic receptors).
- 180. Blockade of ACh receptors Nicotinic receptors are blocked by muscle relaxants (also called neuromuscular blockers), and muscarinic receptors are blocked by anticholinergic drugs....atropine. Although nicotinic and muscarinic receptors differ in their response to some agonists (eg, nicotine, muscarine) and some antagonists (eg, vecuronium vs atropine), they both respond to acetylcholine
- 181. Methacholine...primarily muscarinic agonists • by inhalation used as a provocative test in asthma bethanechol...primarily muscarinic agonists • used for bladder atony, carbachol has both muscarinic and nicotinic agonist activities. • used topically for wide-angle glaucoma.
- 185. Goals of Reversal of NM Blockade primary goal is to maximize nicotinic transmission with a minimum of muscarinic side effects.
- 186. MECHANISM OF ACTION Normal neuromuscular transmission critically depends on acetylcholine binding to nicotinic cholinergic receptors on the motor endplate. Nondepolarizing muscle relaxants act by competing with acetylcholine for these binding sites, thereby blocking neuromuscular transmission. Reversal of blockade • spontaneous reversal • redistribution, • metabolism, and • excretion from the body • pharmacological reversal Cholinesterase inhibitors indirectly increase the amount of acetylcholine available to compete with the nondepolarizing agent, thereby reestablishing normal neuromuscular transmission.
- 187. Cholinesterase inhibitors inactivate acetylcholinesterase by reversibly binding to the enzyme covalent bonds....neostigmine & pyridostigmine... Long duration electrostatic attraction and hydrogen bonding....edrophonium...short duration clinical duration of the cholinesterase inhibitors used in anesthesia......influenced by the rate of drug disappearance from the plasma.
- 188. Mechanisms of action other than acetylcholinesterase inactivation Edrophonium seems to have prejunctional effects that enhance the release of acetylcholine. Neostigmine has a direct (but weak) agonist effect on nicotinic receptors. • Acetylcholine mobilization and release by the nerve may also be enhanced (a presynaptic mechanism). In excessive doses, acetylcholinesterase inhibitors • paradoxically potentiate a nondepolarizing neuromuscular blockade....may cause receptor channel blockade
- 189. Cholinesterase inhibitors prolong the depolarization blockade of succinylcholine. Two mechanisms may explain this latter effect: • increase in acetylcholine (which increases motor end-plate depolarization) • inhibition of pseudocholinesterase activity. Neostigmine and to some extent pyridostigmine display some limited pseudocholinesterase-inhibiting activity, but their effect on acetylcholinesterase is much greater. Edrophonium has little or no effect on pseudocholinesterase. In large doses, neostigmine can cause a weak depolarizing neuromuscular blockade.
- 190. Organophosphates special class of cholinesterase inhibitors, form very stable, irreversible bonds to the enzyme Acetalcholinesterase.... • ophthalmology • pesticides.
- 191. CLINICAL PHARMACOLOGY General Pharmacological Characteristics Cholinesterase inhibitors can act at cholinergic receptors of several other organ systems Cardiovascular receptors —Th e predominant muscarinic eff ect on the heart is • bradycardia that • sinus arrest. Pulmonary receptors —Muscarinic stimulation can result in • bronchospasm (smooth muscle contraction) and • increased respiratory tract secretions.
- 192. Cerebral receptors — • Physostigmine is a cholinesterase inhibitor that crosses the bloodbrain barrier and can cause • diffuse activation of the electroencephalogram by stimulating muscarinic and nicotinic receptors within the central nervous system. • Unlike physostigmine, cholinesterase inhibitors used to reverse neuromuscular blockers do not cross the blood–brain barrier. Gastrointestinal receptors — • Muscarinic stimulation increases peristaltic activity (esophageal, gastric, and intestinal) • glandular secretions (eg, salivary). • Postoperative nausea, vomiting, • fecal incontinence
- 193. Unwanted muscarinic side eff ects are minimized by • Prior or concomitant administration of anticholinergic medications, such as • Atropine sulfate or • Glycopyrrolate. Clearance • Hepatic metabolism (25% to 50%) • Renal excretion (50% to 75%). • Any prolongation of action of a nondepolarizing muscle relaxant from renal or hepatic insufficiency will probably be accompanied by a corresponding increase in the duration of action of a cholinesterase inhibitor.
- 195. When reversal agent should be given? no amount of cholinesterase inhibitor can immediately reverse a block that is so intense that..... cannot be reversed if • there is no response to tetanic peripheral nerve stimulation. • Moreover, absence of any palpable single twitches following 5 sec of tetanic stimulation at 50 Hz . Some evidence of spontaneous recovery ...(ie, the first twitch of the train-of-four [TOF]) should be present before reversal is attempted. The posttetanic count (the number of palpable twitches after tetanus) generally correlates with the time of return of the first twitch of the TOF and therefore the ability to reverse intense paralysis.....
- 196. Example intermediate-acting agents, such as atracurium and vecuronium..... • a palpable posttetanic twitch appears about 10 min before spontaneous recovery of the first twitch of the TOF for longer-acting agents, such as pancuronium..... • a palpable posttetanic twitch appears about 40 min before spontaneous recovery of the first twitch of the TOF
- 197. Factors effecting The time required to fully reverse a nondepolarizing block 1.Choice cholinesterase inhibitor administered 2.Dose of cholinesterase inhibitor administered 3.The muscle relaxant being antagonized, 4.Extent of the blockade before reversal.
- 199. example • reversal with edrophonium is usually faster than with neostigmine • large doses of neostigmine lead to faster reversal than small doses • intermediate-acting relaxants reverse sooner than long-acting relaxants • a shallow block is easier to reverse than a deep block (ie, twitch height >10%). intermediate-acting relaxants require a lower dose of reversal agent (for the same degree of blockade) than long-acting agents, and • concurrent excretion or metabolism provides a proportionally faster reversal of the short- and intermediate-acting agents.
- 200. Factors associated with faster reversal are also associated with • a lower incidence of residual paralysis in the recovery room and a • lower risk of postoperative respiratory complications A reversal agent should be routinely given to all patients who have received nondepolarizing muscle relaxants unless • full reversal can be demon-strated or • postoperative plan includes continued intubation and ventilation.
- 201. Has patient reversed adequately? A peripheral nerve stimulator should also be used to monitor the progress and confirm the adequacy of reversal. In general, the higher the frequency of stimulation, the greater the sensitivity of the test • (100-Hz tetany > 50-Hz tetany or TOF >single-twitch height). Clinical signs of adequate reversal also vary in sensitivity • (sustained head lift >inspiratory force > vital capacity > tidal volume). Thus ....end points of recov-ery are • sustained tetanus for 5 sec in response to a 100-Hz stimulus in anesthetized patients or • sus-tained head or leg lift for at least 5 sec in awake patients.
- 202. NEOSTIGMINE Physical Structure • consists of a carbamate moiety......provides covalent bonding to acetylcholines-terase. • quaternary ammonium group.....renders the molecule lipid insoluble, so that it cannot pass through the blood–brain barrier. Dosage & Packaging • The usual dose of neostigmine ........0.04-0.08mg / kg in combination with either • atropine 0.02 mg /kg OR 0.4 mg of atropine per 1 mg of neostigmine or • glycopyrrolate 0.01 mg/kg OR 0.2 mg glycopyrrolate per 1 mg of neostigmine Neostigmine takes at least 2 min to have an initial effect, and recovery from neuromuscular block is maximally enhanced by 10 min.
- 203. OR 0.01 mg/kg a 0.02 mg /kg OR 0.4 mg of atropine per 1 mg of neostigmine
- 204. Clinical Considerations Effects of neostigmine (0.04 mg/kg) are usually apparent in 5min, peak at 10 min, and last more than 1 hr. Many clinicians use a dose of • 0.04 mg/kg (or 2.5 mg) if the preexisting blockade is mild to moderate • 0.08 mg/kg (or 5 mg) if intense paralysis is being reversed Neostigmine crosses the placenta, resulting in fetal bradycardia. .........Atropine may be a better choice of an anticholinergic agent than glycopyrrolate in pregnant Neostigmine is also used to treat myasthenia gravis, urinary bladder atony, and paralytic ileus.
- 205. OTHER CONSIDERATIONS Recovery from neuromuscular blockade is influenced by the • Depth of block at the time of antagonism • Clearance and half-life of the relaxant used • Other factors that aff ect neuromuscular blockade • Drugs • Electrolyte • Acid/base balance • Temperature
- 207. NON-CLASSIC REVERSAL AGENTS Two unique drugs , under investigation these agents act as selective antagonists of nondepolarizing neuromuscular blockade. Sugammadex....Able to reverse aminosteroid- induced neuromuscular blockade L-cysteine....Reverse the neuromuscular blocking effects of gantacurium and other fumarates.
- 208. SUGAMMADEX modified gamma-cyclodextrin ...... • SU- refers to sugar • gammadex ...... refers to the structural molecule gamma-cyclodextrin Sugammadex is a novel selective relaxant- binding agent that is currently available for clinical use in Europe
- 211. Physical Structure three-dimensional structure resembles a hollow truncated cone or doughnut with a hydrophobic cavity and a hydrophilic exterior. MECHANISM • Hydrophobic interactions trap the drug (eg, rocuronium) in the cyclodextrin cavity (doughnut hole), resulting in tight formation of a water-soluble guest–host complex in a 1:1 ratio. • terminates the neuromuscular blocking action and restrains the drug in extracellular fluid where it cannot interact with nicotinic acetylcholine receptors. • eliminated unchanged via the kidneys.
- 212. Clinical Considerations doses of 4–8 mg/kg. • injection of 8 mg/kg, given 3 min after administration of 0.6 mg/kg of rocuronium, recovery of TOF ratio to 0.9 was observed within 2 min. produces rapid and effective reversal of both shallow and profound rocuronium-induced neuromuscular blockade Due to hypersensitivity and allergic reactions, sugammadex has not yet been approved by the US Food and Drug Administration.
- 213. L -CYSTEINE An endogenous amino acid that is oft en added to total parenteral nutrition regimens to enhance calcium and phosphate solubility. Reverse the neuromuscular blocking effects of gantacurium and other fumarates. Mechanism • Ultrashort-acting neuromuscular blocker, gantacurium, and other fumarates rapidly combine with L -cysteine in vitro to form less active degradation products (adducts). • L -cysteine (10–50 mg/kg intravenously) given to anesthetized monkeys 1 min after these neuromuscular blocking agents.... • Abolished the block within 2–3 min Antagonism was found to be superior to that produced by anticholinesterases Unique method of antagonism by adduct formation and inactivation is still in the investigative stage in humans.
- 214. THANKS