
Recommandé
Recommandé
Contenu connexe
Similaire à patholo jaundice.pptx
Similaire à patholo jaundice.pptx (20)
Plus de NatanA7
Plus de NatanA7 (20)
Dernier
Dernier (20)
patholo jaundice.pptx
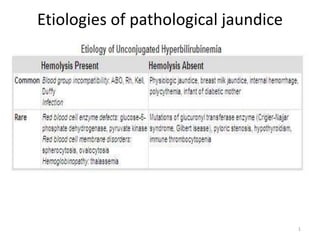
- 1. Etiologies of pathological jaundice 1
- 2. 2
- 3. 3
- 4. Kernicterus ( bilirubin encephalopathy) • Definition: neurological syndrome resulting from deposition of indirect bilirubin in the basal ganglia and brain stem • Multifactorial→ the precise blood level and the duration of exposure is not known 4
- 5. Clinical features of kernicterus Acute form • Phase 1 ( 1st-2nd d): poor sucking, stuper, hypotonia, seizure • Phase 2(middle of 1st wk): hypertonia of extensor muscles, opisthonos, retrocollis,fever • Phase 3(after 1 wk):hypertonia 5
- 6. Chronic form • 1st year: hypotonia, active deep tendon reflexes, obligatory tonic neck reflex, delayed motor skill • After 1st year:movement disorder(choreoathetosis,ballismus, tremor), upward gaize, sensorineural hearing loss 6
- 7. Prevention of kernicterus 1. for any neonate with jaundice within 24hrs, serum bilirubin level should be checked 2. Follow up within 2-3d of discharge for all neonate discharged earlier than 48hr 3. Recognize the presence of possible risk factor 4. Never underestimate the severity of jaundice by visual assessment 5. Early initiation of phototherapy in those with elevated bilirubin 6. Recognize parental concern regarding jaundice, poor feeding, lethargy 7
- 8. Diagnosis of pathological jaundice History and physical examination • Time of onset, duration, color, and pattern of jaundice • Symptoms suggestive of anemia,polycythemia • Family history • Maternal blood group and rh • Perinatal hx (sns&sms of infection, drug) • Term/premature? • Me conium passed /not? • Breast feeding/not? 8
- 9. • Hematoma/ bruising • Nutritional status • Respiratory destress/not • Hepato-spleenomegally • Sns &sms suggestive of sepsis • Vomiting, lethargy, poor feeding, apnea, bradycardia, excessive weight loss • Light colored stool, dark urine 9
- 10. Laboratory investigation • TSB and direct bilirubin level • Blood type(ABO, Rh) • Direct antibody test(coombs test) • Serum albumin • CBC with differential and smear for RBC morphology 10
- 11. • Reticulocyte count • ETCO(end tidal carbon monoxide) • G6PD( Glucose-6-phosphate dehydrogenase) • Urine for reducing agents 11
- 12. Treatment of hyperbilirubinemia Goal: to prevent neurotoxicity while not causing harm. • phototherapy •Exchange transfusion 12
- 13. Phototherapy • Exposure to high intensity of light in the visible spectrum • Maximally in the blue range(420-470nm) • Broad spectrum(white, blue) and narrow- spectrum(super blue) • Photochemical reaction reversible photo-isomerization lumirubin-irreversible structural isomer 13
- 14. • Factors light enery emitted in the effective range distance b/n neonate and the lights surface area of the exposed skin the rate of production, metabolism and excretion • Imtensive phototherapy special blue fluorescent tubes lamp 15-20 fiber optic phototherapy blanket 14
- 15. • Not substitute for exchange transfusion(indicated) • Monitoring: continuous, turned frequently, serum bilirubin and hematocrit every 4-8 hr should continue for at least 24 hr after Rx, skin color is not reliable. • Role of iv fluid supplementation- dehydrated pts , level neat to exchange 15
- 16. 16
- 17. Complications of phototherapy • Loose stool, erythematous macular rash, purpuric rash—transient porphyrinemia • Overheating, dehydration, hypothermia, bronze baby syndrome ( dark, grayish-brown skin discoloration), corneal damage 17
- 18. Exchange transfusion • Indications if intensive phototherapy fails if the risk of kernicterus exceeds the risk of pr if signs of kernicterus are evident if the TSB is in the range for exchange 18
- 19. 19
- 20. • the total amount of blood exchanged is equal to 2x the neonates blood volume Weight(kg) x 85 ml/Kg x 2 • 5-20ml/cycle are withdrawn and infused, 45-90 min • Should remove 85% of infant’s RBC, maternal antibodies, and exchangeable tissue ind.bilirubin • Catheter • Continuation of photherapy-reduces subsequent exchange transfusion. 20
- 21. complications • Blood( transfusion rxn, metabolic instability, infection), catheter(vessel perforation), procedure( hypotension or necrotizing enterocolitis) • Late-anemia 21