Meningioma
•Télécharger en tant que PPTX, PDF•
14 j'aime•6,065 vues

Meningioma is a brain tumor emerging from meninges

Recommandé
Contenu connexe
Tendances
Tendances (20)
Similaire à Meningioma
Similaire à Meningioma (20)
Plus de Nisha Mathew
Dernier
Dernier (20)
Meningioma
- 2. INTRODUCTION Although meningiomas are considered a type of primary brain tumor They do not grow from brain tissue instead arise from the meninges 3 thin layers of tissue covering the brain and spinal cord. These tumors most commonly grow inward causing pressure on the brain or spinal cord they may also grow outward toward the skull, causing it to thicken Most meningiomas are benign, slow-growing tumors Some contain cysts (sacs of fluid), calcifications (mineral deposits), or tightly packed bunches of blood vessels
- 3. MENINGES These are the membranes that envelop the brain and spinal cord of the central nervous system. It consist of three layers: the dura mater, the arachnoid mater , and the pia mater. The primary function of the meninges is to protect the central nervous system.
- 4. NAMING One system names meningiomas by the type of cells in the tumor: Syncytial (or meningothelial) meningiomas are the most common and feature unusually plump cells Fibroblastic meningiomas feature long, thin shaped cells Transitional meningiomas contain both types of cells.
- 5. Another system uses the terms benign, atypical and malignant (or anaplastic) to describe the overall grade of meningiomas. Benign meningiomas: easily recognized, well- differentiated cell & grow slowly. Atypical tumors : proliferating cells, faster growing & may grow back after treatment. Malignant or “anaplastic” : poorly differentiated cells that recur rapidly.
- 6. INCIDENCE Meningiomas account for about 34% of all primary brain tumors. They are likely to be diagnosed in adults older than 60 years of age. The incidence appears to increase with age Meningiomas are rarely found in children They occur about twice as often in women as in men.
- 7. CAUSES Presence of an abnormal chromosome 22. Extra copies of platelet-derived growth factor (PDFGR) and epidermal growth factor receptors (EGFR) Previous radiation to the head History of breast cancer Neurofibromatosis type 2
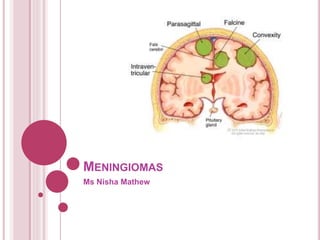
- 8. SYMPTOMS Meningiomas they may grow to a large size before causing symptoms. These tumors are most often found in the coverings of the parasagittal/falcine region (near the top of the brain) and the convexity (the outer curve) of the brain. Other common sites include the sphenoid ridge at the bottom of the brain, called the skull base. As the tumor grows an increased ICP is seen Headache and weakness in an arm or leg Nausea & Vomiting Seizures personality change visual problems Pain and loss of sensation
- 10. DIAGNOSIS Physical examination & clinical history neurological examination MRI and/or a CT scan. MR angiography (a MRI scan of the blood vessels) Arteriogram (a blood vessel X ray) to plan embolization. Biopsy
- 11. TREATMENT Surgery The goals of surgery are to obtain tissue for diagnosis and to remove as much tumor as possible If the tumor cannot be removed, a biopsy to obtain a sample of tumor tissue may be performed. the surgeon may use stereotactic imaging and instrument guiding technologies to navigate through the brain. Occasionally, surgery is performed within a specialized MRI (intraoperative MRI), which allows the surgeon to view the tumor during the operation and determine the extent of tumor that is removed High powered microscopes may be used to help the surgeon to better see the tumor. Ultrasonic aspirators are used to break up and suction out parts of the tumor. In cases where the tumor cannot be removed completely, partial removal can help decrease symptoms. Radiation may then be used to treat the remaining tumor.
- 13. Radiation Therapy Conventional EBRT is given five days a week for five or six weeks. Stereotactic radiosurgery Stereotactic radiation therapy
- 14. Medical treatment Anti epileptic drugs Cortcosteroids pre & post operatively Antiemetics
- 15. Chemotherapy & Biotherapy •Alpha interferons & Hydroxyurea •Targeted molecular agents • Epidermal growth factor receptor (EGFR) inhibitors • Platelet-derived growth factor receptor (PDGFR) inhibitors • Vascular endothelial growth factors (VEGF) inhibitors • Immunotherapy or the use of biological agents to stimulate the immune system Progesterone receptor inhibitors Somatostatin analogs