

Recommandé
Contenu connexe
Tendances
Tendances (20)
Similaire à CDH AND DDH
Similaire à CDH AND DDH (20)
Dernier
Dernier (20)
CDH AND DDH
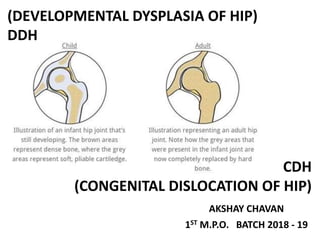
- 1. AKSHAY CHAVAN 1ST M.P.O. BATCH 2018 - 19 CDH (CONGENITAL DISLOCATION OF HIP) (DEVELOPMENTAL DYSPLASIA OF HIP) DDH
- 2. CONGENITAL DISLOCATION OF HIP (CDH) This is spontaneous dislocation of the hip occurring before, during or shortly after birth. DEVELOPMENTAL DYSPLASIA OF THE HIP ( DDH ) It is the abnormal development of Acetabulum or Head of femur
- 3. CDH DDH 1. IT IS CAUSED DURING BIRTH OR SHORHTLY AFTER BIRTH. 1. IT IS CAUSED DURING EMBRYONIC , FOETAL, OR INFANTILE STAGE 2. COMPLICATIONS OF DDH ARE NOT SEEN IN CDH 2. COMPLICATIONS OF CDH ARE DIAGNOSED HERE. EG:SUBLUXATION 3. ETIOLOGY: EDIOPATHIC 3. EDIOPATHIC: GENETIC AND ETHNIC 4. HEAD OF FEMUR IS TOTALLY DISLOCATED FROM HIP 4. THE HEAD OF THE FEMUR MAY OR MAY NOT BE DISLOCATED 5. IT IS NOT A HEREDITORY DISEASE. 5. IT IS A HEREDITORY DISEASE.(23% of chances of it being passed on to generations)
- 4. • AETIOLOGY C D H a) Contracted pelvis cause tighten the space in uterus . b) Increased estrogen level before birth lead to laxity of capsule . c) Ethnic factors (Americans). D D H a) Hereditary predisposition to joint laxity ,chromosome no 13. b) Hormone induced joint laxity: CDH is 3-5 times more common in females. c) Breech malposition.
- 5. It is uncommon in India and some other Asian countries, probably because of the culture of mother carrying the child on the side of her waist with the hips of the child abducted. • This position helps in reduction of an unstable hip, which otherwise would have dislocated. • The general term “dysplastic hip” is sometimes used for these congenital malformations of the hip. • In western countries, it is one of the commonest congenital disorder. 25 to 50 babies per 1000 birth. • India it is 2 babies per 1000 birth.
- 6. • Depth of acetabulum • Tension and strength of ligaments & surrounding muscles • Length & obliquity of the neck of femur STABILITY OF HIP JOINT
- 7. PATHOLOGY • Femoral head is dislocated upwards and laterally; its epiphysis is small and ossifies late. • Femoral neck is excessively anteverted. • Acetabulum is shallow, with a steep sloping roof. • Ligamentum teres is hypertrophied. • Fibro-cartilaginous labrum of the acetabulum (limbus) may be folded into the cavity of the acetabulum (inverted limbus). • Capsule of the hip joint is stretched. • Muscles around the hip, especially the adductors, undergo adaptive shortening.
- 8. CLINICAL FEATURES • CDH may be detected at birth or soon after Sometimes not noticed until the child starts walking. • Routine screening of suggestive sing in every newborn baby especially those who are at high risk. • Asymmetrical groin fold ,clicks, limitation of moments. • Girls are affected 6 times more often than boys. • In 1/3 of all cases both hips are affected Or left hip is commonly affected .
- 10. FOR OLDER CHILD • Limitation of movement , limb may be short . • Higher buttock fold on the affected side, asymmetrical tight fold . • Galeazzi’s sign: The level of the knees are compared in a child lying with hip flexed to 700 and knees flexed. • Ortolani’s test may be positive. • Trendelenburg’s test is positive: This test is performed in unilateral an older child. - Trendelenburg’s gait B/L - waddling gait • The limb is short and slightly externally rotated. • There is lowering of the knee on the affected side.
- 11. RADIOLOGICAL FEATURES In child below the age of 1 year it is difficult to diagnose a dislocated hip on plain X-rays. Ultrasound examination is useful in early diagnosis at birth. • Delayed appearance of the ossification • Sloping acetabulum. • Lateral and upward displacement of the ossification center
- 12. Treatment ORTHOTIC GOAL • To attain a concentric reduction of hip • To produce normal Acetabulum & Femoral Head development . • To avoid complications like stiffness , infection & avascular necrosis of head of femur . • To avoid unnecessary patient & parental hardship . • Splint should be maternal. Aim is to achieve reduction of the head into the acetabulum and maintain it until the hip becomes clinically stable and a “round” acetabulum covers the head Most cases closed reduction possible, else open reduction done.
- 13. Birth to 6 month • Where facilities for ultrasound scanning are available, all new-born infants at risk are examined by USG. • If hip is reduced and has a normal cartilaginous outline, no treatment is required, observe for 3-6m. • If acetabular dysplasia or hip instability, the hip is splinted in a position of flexion and abduction and USG done at intervals. Orthotics intervention • The Pavlik harness • Frejka pillow • Von Rosen’s splint
- 14. Pavlik harness • Arnold Pavlik developed his device ‘harness with stirrups’ in the 1940s. • He considered active movement of the hip joint as the most important therapeutic factor in the treatment of DDH and named his method ‘functional treatment’. • The main aim of Pavlik was to achieve spontaneous and harmless repositioning and centralization of the femoral head in order to reach the best anatomical and functional outcome in children up to one year of age • keeping the hips and knees in flexion and the hips in abduction, allowing active hip movements, first relaxed the adduction contracture and then a spontaneous reduction would occur during the abduction movements
- 15. • Adjustable chest band positioned at the nipple line, with halter strap that should cross in the back to prevent slipping. • Two shoulder strap which crosses posteriorly • The posterior straps should overlie the scapula, and the leg straps should not impinge in the popliteal fossa. • Two anterior & two posterior straps which helps to provide desire amount of flexion & abduction of hip . They should be at anterior auxiliary line, if more medial, they produce an adduction force. • The posterior straps should be tight enough to prevent adduction. • Two ankle stirrups which contain ankle & foot • Once the child has been placed in the harness, a radiograph should be obtained to ensure that reduction has been obtained.
- 16. Points to be remember during fitting of pavlik harness : 1 . Force must not be used for reduction . 2 . Position of the hip must be confirm radiographically . 3 . Hip must be flexed 90 to 110 degree to direct the head into tri-radiate cartilage . 4 . Posterior straps should not be tight in order to avoid forceful abduction . Straps should allows knee to adduct within 1”-2 “ of the midline . 5. Harness allows active movement in all direction except extension & adduction . How long will child need to wear the harness? The amount of treatment time varies based upon the severity of child’s DDH. In the majority of cases, the harness is worn 24 hours a day for 8–12 weeks. After every 3–4 weeks, harness should be adjust according to severity.
- 17. Disadvantages : 1 . Difficult to educate parents for donning & doffing of the harness . 2 . Manual error in tightening of straps causes loss of positioning . 3. Forceful abduction may cause avascular necrosis 4 . Chances of inferior acetabular dislocation . 5 . Transient femoral nerve palsy may happen .
- 18. Frejka pillow splint • It is an analogous treatment , double and triple diapering. • Frejka was one of Pavlik’s professors. • Frejka created the pillow after experiencing some success with abduction treatment. • harnessed to the body by straps and Velcro's. • The splint keeps the legs in an outward rotated position to ensure that the head of the femur locates with the acetabulum or cavities of the pelvis • The treatment lasts normally 3 - 4 months • It did not provide enough flexion to orient properly the proximal femur toward the triradiate cartilage. • The Frejka pillow is constructed as a 9 x 9 x ¾ inch foam pillow, retrained in a cloth harness with encoring ties.
- 19. Von Rosen’s splint • In 1962 Von Rosen reported his use of a special splint in the congenital hip dislocation. • It is passive restraining Or positioning device being adjustable in both abduction and flexion. • made up of malleable aluminum frame which can be molded around shoulder, thighs & waist. • Today the orthosis is made up of malleable plastic with one frame for the shoulders, waist, and thighs. • It has very low rate of AVN but high rate of pressure ulcers .
- 20. 6 month to 18 months • The hip must be reduced – preferably by closed methods but if necessary by operation – and held reduced until acetabular development is satisfactory • Closed reduction : suitable after 6m and is performed under arthrogram to confirm a concentric reduction • Failure to achieve concentric reduction should lead to abandoning this method in favour of an operative approach at approximately 1 year of age
- 21. • Held in a plaster Spica at 60 degrees of flexion, 40 degrees of abduction and 20 degrees of internal rotation. • After 6 weeks the Spica is changed & stability assessed • If satisfactory, Spica retained for 6w, then abduction splint for 6m • If concentric reduction is not achieved, open operation is done • ILFELD ORTHOSIS • DENIS BROWNE BAR • PLASTAZOTE HIP ABDUCTION ORTHOSIS • ABDUCTION SPLINT ORTHOTIC TREATMENT
- 22. ILFELD ORTHOSIS • The Ilfeld orthosis is primarily an abduction orthosis used in the spectrum of DDH. • It promote flexion to some degree. • It differs markedly from the Pavlik harness in that it is a passive device and does not promote motion of the hip joint.
- 23. • It is fabricated with two thigh cuffs and an adjustable metal cross bar that allows variation of abduction. • Suspension is through a waist strap. • It is an effective postoperative treatment to aid in maintain abduction.
- 24. DENIS BROWNE BAR • The DB bar has cuffs that go around the thighs and are attached to a bar. • This holds the hips and knees up (flexed) with the legs apart (abducted). • This position allows contact between the thigh and hip bones and helps the muscles and ligaments to strengthen while the hip is developing.
- 25. PLASTAZOTE HIP ABDUCTION ORTHOSIS • This orthosis maintain 70 – 90 degree of hip flexion & wide • Abduction & allows free motion of the knee . • Consist of one piece pelvic & thigh bands made up of • Plastazote & separated by abduction bar .
- 26. ABDUCTION SPLINT
- 27. Persistence dislocation after 18 month • In older children open reduction arthrography and femoral osteotomy more preferred than close reduction • Traction: help to loosen the tissues and bring the femoral head down opposite the acetabulum. • Acetabular reconstruction procedures- If there is marked acetabular dysplasia,
- 28. ATLANTA SCOTTISH RITE • It is used mainly in CDH post operatively . • Can be used for elderly ambulatory patient . • It has no extension below knee thus has no rotational control . • Ambulation is possible with this brace • Telescopic adjustment bar is given .
- 29. Prevention is better than cure
- 31. Thank you