
Recommandé
Contenu connexe
Similaire à 352.ppt
Similaire à 352.ppt (20)
Plus de PriyankaSharma89719
Plus de PriyankaSharma89719 (20)
Dernier
Dernier (20)
352.ppt
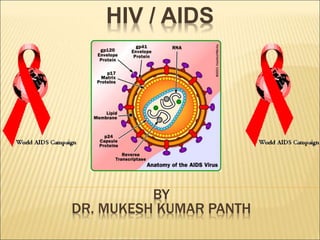
- 1. HIV / AIDS BY DR. MUKESH KUMAR PANTH
- 2. http://naco.gov.in/ https://www.avert.org https://aidsinfo.nih.gov/
- 3. THE GLOBAL AIDS EPIDEMIC 2017 An estimated 36.9 million people were living with HIV worldwide in 2017. 3.0 million were children and adolescents under 20 years of age 19.1 million were women and girls. Each day, approximately 4,900 people were newly infected with HIV Approximately 2,580 people died from AIDS related causes, mostly because of inadequate access to HIV prevention, care and treatment services.
- 4. THE GLOBAL AIDS EPIDEMIC 2017 2017 PEOPLE LIVING WITH HIV (all ages) 36.9 million Adults (aged 15+) 35.1 million Women (aged 15+) 18.2 million Children (aged 0–14) 1.8 million Adolescents (aged 10–19) 1.8 milllion
- 5. THE GLOBAL AIDS EPIDEMIC 2017 AIDS-RELATED DEATHS 2017 All ages 940,000 Adults (aged 15+) 830,000 Women (aged 15+) 350,000 Children (aged 0–14) 110,000 Adolescents (aged 10–19) 38,000
- 6. HIV AND AIDS IN INDIA India has the third largest HIV epidemic in the world. In 2017, HIV prevalence among adults (aged 15- 49) was an estimated 0.2%, this equates to 2.1 million people living with HIV. Overall, India’s HIV epidemic is slowing down, Between 2010 and 2017 new infections declined by 27%. in 2017, new infections increased to 88,000 from 80,000, and AIDS-related deaths increased to 69,000 from 62,000.
- 7. In 2017, 79% of people living with HIV were aware of their status, of whom 56% were on antiretroviral treatment (ART).
- 8. INDIA: HIV INFECTIONS 2005 2010 2017 New HIV infections (all ages) 130 000 120 000 88 000 New HIV infections (0–14) 13 000 7700 3700 New HIV infections (women, 15+) 48 000 45 000 34 000 New HIV infections (men, 15+) 71 000 67 000 50 000
- 9. INDIA: AIDS-RELATED DEATHS 2005 2010 2017 AIDS-related deaths (all ages) 240000 160000 69000 AIDS-related deaths (0–14) 11000 6800 2600 AIDS-related deaths (women, 15+) 88000 58000 20000 AIDS-related deaths (men, 15+) 140000 91000 46000
- 10. INDIA: PEOPLE LIVING WITH HIV 2005 2010 2017 People living with HIV (all ages) 2 800 000 2 300 000 2 100 000 People living with HIV (0–14) 100 000 88 000 61 000 People living with HIV (women, 15+) 1 100 000 900 000 880 000 People living with HIV (men, 15+) 1 600 000 1 300 000 1 200 000
- 11. DR. S.K CHATURVEDI ADULT HIV PREVALENCE High Prevalence States: these are Tamil Nadu, Maharastra, Karnataka, Andhra Pradesh, Manipur and Nagaland
- 12. DR. S.K CHATURVEDI MODE OF TRANSMISSION OF HIV IN INDIA 5.95 3.45 2.07 2.7 85.83 Sexual IDUs Blood & blood proucts Perinatal Unidentified
- 13. HIV “HUMAN IMMUNODEFICIENCY VIRUS” H – Human – This particular virus can only infect human beings. I – Immunodeficiency – HIV weakens immune system by destroying important cells that fight disease and infection. A "deficient" immune system can't protect you. V – Virus – A virus can only reproduce itself by taking over a cell in the body of its host.
- 14. AIDS : Acquired Immune Deficiency Syndrome A – Acquired – AIDS is not something that someone inherit from their parents like other things. You acquire AIDS. I – Immuno – Body's immune system includes all the organs and cells that work to fight off infection or disease. D – Deficiency – Someone get AIDS when their immune system is "deficient," or isn't working the way it should. S – Syndrome – A syndrome is a collection of symptoms and signs of disease. AIDS is a syndrome, rather than a single disease. It is a complex illness with a wide range of symptoms.
- 15. HIV VS. AIDS HIV causes AIDS by attacking the immune system’s CD4 T cells. Normal CD4 count is between 500 – 1500 CD4 T cells per ul of blood, while AIDS CD4 count is less than 200 CD4 T cells per ul of blood. AIDS viral load is about 55,000 HIV RNA copies per ml of blood. On average, it takes approximately 10 years to develop AIDS from initial infection. As a person’s CD4 count decreases, he/she is more prone to opportunistic infections.
- 16. HIV MYTHS • I can get HIV by being around people who are HIV-positive. • I'm HIV-positive…my life is over. • I'm straight and don't use IV drugs - I won't become HIV- positive. • You can’t get HIV from oral sex. • My partner and I are both HIV positive, so there is no need to use a condom. • I can get HIV from mosquitoes. • Coughing, sneezing • Insect bites • Touching, hugging • Water, food • Kissing • Public baths • Handshakes • Work or school contact • Using telephones • Sharing cups, glasses, plates, or other utensils
- 17. TYPES OF HIV HIV-1 More virulent Responsible for worldwide epidemic Severity of infection varies from person to person HIV-2 Primarily found in western Africa Not transmitted as efficiently
- 18. ORIGINS OF HIV HIV-1 likely descended from SIVcpz HIV-2 likely descended from SIVsm Pan troglodytes troglodytes Sooty Mangabey
- 19. ZOONOSIS: HOW DID IT HAPPEN? Human killing and eating of chimpanzees contact with infected blood ingestion of uncooked or undercooked meat
- 20. Three earliest know HIV infections 1959 - serum sample from an adult male living in what is now the Democratic Republic of Congo 1969 - tissue samples from a teenager who died in St. Louis 1976 - tissue samples from a Norwegian sailor January 2000 - study by Dr. Bette Korber estimates first case of HIV infection to be 1930 Study based on complicated computer model of HIV’s evolution and has a 20yr error margin
- 21. HIV A Brief History of the modern epidemic
- 22. IN THE BEGINNING... 1675 - Speculation that HIV was first transmitted from chimpanzees to humans 1926-1946 - Scientists believe HIV first spread from monkeys to humans 1959 - First proven AIDS death 1978 - Gay men in US and Sweden begin showing signs of what is now known as AIDS
- 23. THE FIRST INDICATIONS 1981 - CDC notices increase in cases of Kaposi’s sarcoma and Pneumocystis carinii pneumonia
- 24. DEFINING THE PROBLEM 1982 - The term AIDS (acquired immune deficiency syndrome) is used for the 1st time 1983 - Institut Pasteur isolates HIV-1 CDC issues warning to blood banks about potential problem 1984 - Dr. Robert Gallo claims discovery of HIV
- 25. THE START OF THE WAR 1985 - FDA approves first HIV antibody diagnostic test - First International Conference on AIDS 1986 - HIV-2 isolated 1987 - azidothymidine (AZT) approved by FDA (1st anti- HIV drug)
- 26. FOUR PHASES OF HIV
- 27. • The period of time after you may have been exposed to HIV, but before a test can detect it (at least 3-6 months) • Antibody tests cannot accurately identify infection during this time. Incubation period- Time from exposure to HIV to time when antibodies can be detected through an HIV test.
- 28. PRIMARY HIV INFECTION Asymptomatic Short, flu-like illness, swollen glands, fatigue, diarrhea, weight loss, or fevers - occurs one to six weeks after infection no symptoms at all Infected person can infect other people Lasts for an average of ten years HIV antibodies are detectable in the blood Acute retroviral syndrome
- 29. CLINICAL STAGE 1 . Asymptomatic Short, flu-like illness, swollen glands, fatigue, diarrhea, weight loss, or fevers - occurs one to six weeks after infection no symptoms at all Infected person can infect other people Lasts for an average of ten years HIV antibodies are detectable in the blood . Persistent generalized lymphadenopathy
- 30. . Moderate unexplained weight loss (<10% of presumed or measured body weight) . Recurrent respiratory tract infections . Herpes zoster Angular cheilitis Recurrent oral ulceration . Papular pruritic eruptions Seborrhoeic dermatitis . . . . Fungal nail infections CLINICAL STAGE 2
- 31. CLINICAL STAGE 3 Unexplained severe weight loss (>10% of presumed or measured body weight) Unexplained chronic diarrhoea for longer than one month Unexplained persistent fever (intermittent or constant for longer than one month) Persistent oral candida Oral hairy leukoplakia Pulmonary TB Severe presumed bacterial infections (e.g. pneumonia, or joint infection, meningitis) Unexplained anaemia (<8 g/dl ),
- 32. CLINICAL STAGE 4 . HIV wasting syndrome : The "wasting syndrome" is defined as a weight loss of at least 10% in the presence of diarrhea or chronic weakness and documented fever for at least 30 days that is not attributable to a concurrent condition other than HIV infection itself. Pneumocystis pneumonia Chronic herpes simplex infection (orolabial genital or anorectal of more than one months duration or visceral at any site) Oesophageal candidiasis (or candida of trachea, bronchi or lungs)Oesophageal candidiasis.jpg Extrapulmonary TB
- 33. CLINICAL STAGE 4 . Kaposi sarcoma . Central nervous system toxoplasmosis (headache, fever, confusion, muscle weakness,seizures, abnormal behavior, and coma) . HIV encephalopathy (decline in thinking, or "cognitive," functions such as memory, reasoning, judgment, concentration, and problem solving.) . Progressive multifocal leukoencephalopathy (“Progressive” means that it continues to get worse, often leading to serious brain damage. “Multifocal” means that it affects several parts of the brain. “Leukoencephalopathy” means that the disease affects the white matter of the brain.) Chronic cryptosporidiosis Chronic isosporiasis Disseminated mycosis (extrapulmonary histoplasmosis, coccidiomycosis, penicilliosis) Recurrent septicaemia (including non-typhoidal salmonella) Lymphoma (cerebral or B cell non-Hodgkin) Invasive cervical carcinoma Atypical disseminated leishmaniasis
- 34. HOW IS HIV SPREAD? HIV is passed from person to person through the exchange of bodily fluids. 4 Main Ways: 1. Unprotected sex with people living with HIV (vaginal, oral, or anal) 2. Infected syringe 3. Infected blood 4. Exposure to HIV before or during birth or through breastfeeding
- 35. WHAT FLUIDS CAN TRANSMIT HIV? 8
- 36. THROUGH IV DRUG USE Sharing Needles Without sterilization Increases the chances of contracting HIV
- 37. THROUGH SEX Intercourse (penile penetration into the vagina) Oral Anal
- 38. MOTHER-TO-BABY Before Birth During Birth Postpartum After the birth
- 39. CANNOT GET HIV FROM… Tears Saliva Sweat Urine of an HIV infected person 39
- 40. WHY HIV RATES NOT GOING DOWN? Sex at an early age Little life-skills and sex education Little condom use Multiple partners Stigma and Discrimination Sex for money or sex for .....things Substance abuse: Ganja, cocaine, alcohol Men having sex with men 40
- 41. TESTING OPTIONS FOR HIV
- 42. TESTING 1. Enzyme-linked immunosorbent assay (ELISA); 2. Western blot assay; and 3. Rapid tests.
- 44. ANTIRETROVIRAL DRUGS Nucleoside Reverse Transcriptase inhibitors AZT (Zidovudine) Non-Nucleoside Transcriptase inhibitors Viramune (Nevirapine) Protease inhibitors Norvir (Ritonavir)
- 45. FOUR WAYS TO PROTECT Practice abstinence Avoid multiple partners- Monogamous Relationship (only one sex partner) Protected Sex Don’t share needles, syringes, drug injection equipment, or any item that may put a person in contact with blood
- 46. ABSTINENCE It is the only 100 % effective method of not acquiring HIV/AIDS. Refraining from sexual contact: oral, anal, or vaginal. Refraining from intravenous drug use
- 47. MONOGAMOUS RELATIONSHIP A mutually monogamous (only one sex partner) relationship with a person who is not infected with HIV HIV testing before intercourse is necessary to prove your partner is not infected
- 48. PROTECTED SEX Use condoms (female or male) every time When Using A Condom Remember To: •Make sure the package is not expired •Make sure to check the package for damages •Do not open the package with your teeth for risk of tearing •Never use the condom more than once
- 49. STERILE NEEDLES If a needle/syringe or cooker is shared, it must be disinfected: Fill the syringe with undiluted bleach and wait at least 30 seconds. thoroughly rinse with water Do this between each person’s use
- 50. Clinical risk assessment and HIV pre-test counselling
- 51. SESSION OBJECTIVES Integrate clinical risk assessment, HIV prevention education and counselling into HIV pre-test counselling Conduct a clinical risk assessment and facilitate the development of a plan for risk reduction Assess risks within the HIV test window period Apply basic counselling micro-skills to HIV pre-test counselling Assess client’s coping strategies and
- 52. RISK ASSESSMENT IN HIV/AIDS A major component of test HIV pre- counselling is the completion of risk assessment Assesses actual against perceived level of risk Requires the counsellor to ask explicit questions about various practices of an individual including: —Sexual practices, —Drug-using practices,
- 53. NEED FOR DETAILED CLINICAL RISK ASSESSMENT Promote greater awareness and concern about STIs and HIV Prevention counselling and education Determination of necessary health investigations Feedback to the client regarding levels of risk associated with various practices Implications for treatment
- 54. REASONS FOR DETAILED ASSESSMENT Consideration of the window period Consideration of pregnancy and prophylaxis One-to-one education and clarification Clinical decision-making—early versus late infection management Other medical investigations
- 55. REMEMBER, HOWEVER… Privacy and confidentiality Explanation of the four principles of HIV transmission (ESES) when asking for sensitive information Educate first then question about risk Start with the least controversial area or the area of least concern for the client Use open-ended questions Be non-judgemental
- 56. GUIDELINES FOR CONDUCTING RISK ASSESSMENT Provide space to maintain privacy Assure confidentiality See each individual separately Assume that the client will be embarrassed Ensure client understands the terms used: —clear and simple language —use models or drawings if needed Use neutral language, do not use colloquial, offensive or technical terms
- 57. GUIDELINES FOR CONDUCTING RISK ASSESSMENT (CONTD) Begin with less controversial issues to put the client at ease Obtain detailed information Discuss all practices with all clients Remember your foundation skills in communication: —listening —questioning —non-verbal skills or body language Do not allow your personal values or beliefs to influence the history-taking
- 58. AIMS OF PRE-TEST COUNSELLING To ensure that any decision to take the test is fully informed and voluntary To prepare the client for any type of result, whether negative, positive or indeterminate To provide information on risk reduction To provide options for PPTCT To provide an entry point to treatment and care
- 59. AIMS OF PRE-TEST COUNSELLING (CONTD) Develop an individualized risk-reduction plan Facilitate the enactment of the client’s plan Facilitate the acquisition of coping skills Facilitate the use of social support systems and improved support mechanisms (interpersonal and familiar) Focus on issues regarding the test
- 60. PROCESS OF PRE-TEST COUNSELLING Establish a rapport with the client Determine the purpose of the client’s visit to the centre (information, counselling and testing) Give information on HIV 1. Discuss HIV transmission including the 4 principles—ESES 2. Correct any misconceptions—give simple, factual information
- 61. PROCESS OF PRE-TEST COUNSELLING (CONTD) Explain the HIV test Obtain informed consent Reaffirm the right to decline testing Discuss the advantages and disadvantages of the test for the individual Help clients assess their own level of risk and draw up an individualized risk- reduction plan
- 62. PROCESS OF PRE-TEST COUNSELLING (CONTD) Discuss the importance of disclosure of test results to spouse or partner Summarize the session for the client Demonstrate the use of condoms to ensure that the client knows how to use them
- 63. PROCESS OF PRE-TEST COUNSELLING (CONTD) If the client decides to undergo the test: Inform the client about the procedure for the test Length of time for results— immediate/delayed Amount of and manner in which blood (venepuncture, finger prick, etc.) will be taken Remember to show the client blood
- 64. PROCESS OF PRE-TEST COUNSELLING (CONTD) Some flexibility is required, e.g. if the client is distressed at initial presentation, you will need to address this first
- 65. SUMMARY OF PROCEDURE OF PRE-TEST COUNSELLING Cross-check the personal identification number and other identification data against the client’s details Introduction and orientation Collection of demographic data and filling of the pre-test form Basic facts about HIV/AIDS
- 67. SESSION OBJECTIVES Apply knowledge of basic counselling techniques for post-test counselling Understand the basic requirements for the provision of HIV results Conduct a HIV post-test counselling session for a negative result Conduct a HIV post-test counselling session for a positive result
- 68. RECAP ON PRE-TEST COUNSELLING Reason for testing Knowledge of HIV/AIDS Level of understanding of the client Correction on misconceptions Assessment of personal risk Information on HIV test Discussion of possible results Capacity of the client to cope Potential needs and support
- 69. Taking informed consent from the client Making arrangements for follow-up Recap on pre-test counselling (contd)
- 70. OBJECTIVES OF POST-HIV TEST COUNSELLING To prepare the client for the result To help the client understand and cope with the result To provide further information to the client To refer the client to other services To counsel for risk reduction
- 71. KEY CONSIDERATIONS FOR HIV POST-TEST COUNSELLING • Cross-check the report with the client’s personal identification digit (PID), identification marks, age and sex • Provide results only ‘face-to-face’ • Be aware of the manner in which you call clients from the waiting area • As advised by NACO, all results, whether positive or negative, are to be provided in writing • Provide results as per the format provided by the the State AIDS Control Society (SACS)
- 72. GENERAL PRINCIPLES FOR HIV POST-TEST COUNSELLING Be calm when you call the client in for their result Be direct in giving the result Give an explanation of their result Allow enough time for results to sink in
- 73. GENERAL PRINCIPLES FOR HIV POST-TEST COUNSELLING (CONTD) Build up a relationship by including a greeting/ small talk Confirm that the client is ready to collect the test result: Psychosocial condition: Check what was going on in the client’s mind before coming to the centre and while waiting for the test result? Comprehension: Ask if the client would like to summarize what was discussed last time.
- 74. GENERAL PRINCIPLES FOR HIV POST-TEST COUNSELLING (CONTD) Coping strategies: Ask what would they do if the result is negative? What would they do if it is positive? Provide the client space and time to react Help manage emotional response
- 75. GUIDELINES FOR THE PROVISION OF NEGATIVE TEST RESULTS Check for possible exposure in the window period including any since pre-test counselling Reinforce information on transmission, safe sex/drug use Exploration of constraints to practise of such behaviour Encourage spouse testing Refer to appropriate source for help
- 76. COUNSELLING ISSUES RELATED TO NEGATIVE RESULTS Clients may worry that others will know they have undergone the test and pass judgements about their behaviour Clients fear that employers may consider them ‘risky’ Clients may understand that they need to modify their behaviour but may worry that their partners will not want to change Clients who report HRB but are uninfected may believe they are immune from HIV
- 77. FREQUENT HIV-NEGATIVE TESTERS Often engage in high-risk behaviours Have deep-seated anxiety and belief that they are HIV-positive Should be reassured; if they do not respond then refer to specialist for psychological /psychiatric / mental health follow-up
- 78. POSITIVE RESULT PROVISION Provide a safe, empathetic and accepting environment Allow sufficient time Avoid giving false reassurance Clarify misinformation about the meaning of the result and its implications Assess coping strategies Assess short-term arrangements for leaving the clinic, getting home, etc. Assess support available to the client and
- 79. POSITIVE RESULT PROVISION (CONTD) Discuss partner disclosure and spouse testing Provide information on: health, rest, exercise, diet, risk reduction, home-based care, infection-control issues Ask the client if they have any questions Offer follow-up session Provide written information to read later
- 80. MANAGING EMOTIONAL RESPONSES Crying: Let the client cry; this allows them to vent their feelings Anger: Stay calm, let the client express their feelings, acknowledge that these feelings are normal No response: Due to shock, denial or helplessness Denial: Client has difficulty in accepting the result
- 81. MANAGING EMOTIONAL RESPONSES (CONTD) For all responses, encourage the client to talk about their feelings. Encourage the client to ask questions.
- 82. FOLLOW-UP COUNSELLING HIV tests identify not only infected persons but also several affected ones close to them Important issues need to be addressed Counselling micro-skills and techniques to be used.
- 84. HIV tests identify not only infected persons but also several affected ones close to them Important issues need to be addressed Counselling micro-skills and techniques to be used.
- 85. HIV tests identify not only infected persons but also several affected ones close to them Important issues need to be addressed Counselling micro-skills and techniques to be used.
- 86. HIV tests identify not only infected persons but also several affected ones close to them Important issues need to be addressed Counselling micro-skills and techniques to be used.