1. Safe, Effective, and Well-coordinated
Patient Transition after Elective
Total Joint Replacement:
A “Scheduled Discharge”
BACKGROUND
METHODS
RESULTS
PROJECT AIMS
CONCLUSIONS
CONCLUSIONS
Utilizing the Lean Six Sigma methodology, a process was designed to pilot a discharge appointment for all elective total joint replacement patients.
An “ideal state” discharge process was created after mapping and flow charting the “current state” through consolidation and elimination of steps in order to
move the discharge time 3 hours earlier than the current mean average discharge time. They were given discharge date and time (10:00 am, 10:30 am, or
11:00 am) weeks before the day of surgery. A multidisciplinary checklist was developed and utilized so that scheduled tasks were completed to assure
discharge within 30 minutes of the appointed time. An in-room display of the discharge date and time was posted at the bedside during patient’s admission
to the medical-surgical inpatient nursing unit.
• Scheduling tasks earlier than the day of discharge was practicable.
• During the 6-month period, 36% were discharged by the appointed time; 67% were
discharged on March 2013.
• Average discharge time moved back to 1:10 pm from 4:10 pm.
• The pilot resulted to an initial savings of $28,627.00
• Projected annual savings of $261,000.00
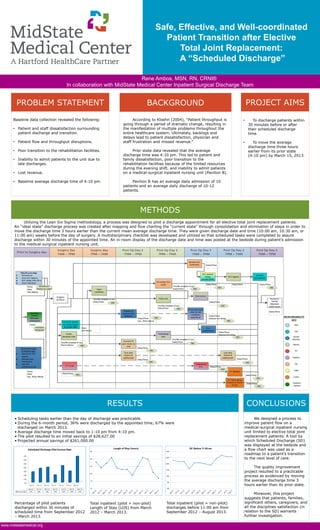
Percentage of pilot patients
discharged within 30 minutes of
scheduled time from September 2012
– March 2013.
We designed a process to
improve patient flow on a
medical-surgical inpatient nursing
unit limited to elective total joint
replacement patients. A tool by
which Scheduled Discharge (SD)
was displayed at the bedside and
a flow chart was used as a
roadmap to a patient’s transition
to the next level of care.
The quality improvement
project resulted to a practicable
process as evidenced by moving
the average discharge time 3
hours earlier than its prior state.
Moreover, this project
suggests that patients, families,
significant others, caregivers, and
all the disciplines satisfaction (in
relation to the SD) warrants
further investigation.
Baseline data collection revealed the following:
• Patient and staff dissatisfaction surrounding
patient discharge and transition.
• Patient flow and throughput disruptions.
• Poor transition to the rehabilitation facilities.
• Inability to admit patients to the unit due to
late discharges.
• Lost revenue.
• Baseline average discharge time of 4:10 pm.
PROBLEM STATEMENT
METHODS
According to Kloehn (2004), “Patient throughput is
going through a period of dramatic change, resulting in
the manifestation of multiple problems throughout the
entire healthcare system. Ultimately, backlogs and
delays lead to patient dissatisfaction, physician and
staff frustration and missed revenue.”
Prior state data revealed that the average
discharge time was 4:10 pm. This led to patient and
family dissatisfaction, poor transition to the
rehabilitation facilities because of the limited resources
during the evening shift, and inability to admit patients
on a medical-surgical inpatient nursing unit (Pavilion B).
Pavilion B has an average daily admission of 10
patients and an average daily discharge of 10-12
patients.
• To discharge patients within
30 minutes before or after
their scheduled discharge
time.
• To move the average
discharge time three hours
earlier from its prior state
(4:10 pm) by March 15, 2013.
Total inpatient (pilot + non-pilot)
Length of Stay (LOS) from March
2012 – March 2013.
Rene Ambos, MSN, RN, CRNI®
In collaboration with MidState Medical Center Inpatient Surgical Discharge Team
www.midstatemedical.org
Total inpatient (pilot + non-pilot)
discharges before 11:00 am from
September 2012 – August 2013.