1. Hyperthyroidism partum thyroiditis. <3% will be negative for all 3 autoimmune Abs
Anti-microsomal Ab – may be + in Hashimoto’s thyroiditis
TSI Thyroid stimulating Immunoglobulin – used when Graves’ dz is suspected
Clinical features by all other Abs are negative
Goitre Diffuse ± bruit Nodular Thyroid scan Differentiate btwn types of ↑T4
131
GI LOW Diarrhoea Anorexia (I or Graves’ dz: Diffuse uptake
N/↑ appetite Steatorrhoea Vomiting Technetium MNG: maximal uptake by active nodules
Cardiorespiratory Palpitation Dyspnoea ↑ pulse pressure 99) Toxic adenoma: uptake by adenoma, ↓ uptake by the remaining tissues
Sinus tachycardia Angina Exacerbation of Thyroid U/S Differentiate btwn cystic and solid thyroid nodules
AF CMP asthma FNAC Differentiate nodule into benign, suspicious or malignant (5%)
Cardiac failure Follicular neoplasm – may be either follicular adenoma or CA.
Ankle oedema in Indistinguishable on FNAC
absence of CF
Neuromuscular Nervous / irritable Tremor Proximal
Emotional lability Hyperreflexia myopathy
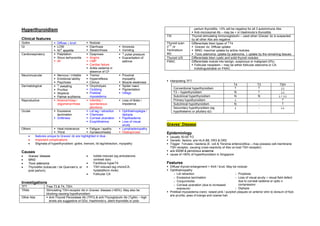
Psychosis Clonus Muscle weakness Interpreting TFT
T4 T3 TSH
Dermatological ↑ sweating Onycholysis Spider naevi
Pruritus Clubbing Pigmentation Conventional hyperthyroidism ↑ ↑ ↓↓
Alopecia Pretibial Vitiligo T3 – hyperthyroidism N ↑ ↓↓
Palmar erythema myxoedema Subclinical hyperthyroidism N N ↓ / ↓↓
Reproductive Amenorrhoea / Infertility / Loss of libido / Primary hypothyroidism ↓ - ↑
oligomenorrhoea spontaneous impotence Subclinical hypothyroidism N - ↑
abortions Secondary hypothyroidism (eg ↓ - ↓↓
Ocular Excessive Lid lag / retraction Ophthalmoplegia / hypothalamic or pituitary dz)
lacrimation Chemosis diplopia
Grittiness Corneal ulceration Papilloedema
Exophthalmos Loss of visual
acuity Graves’ Disease
Others Heat intolerance Fatigue / apathy Lymphadenopathy
Thirst Gynaecomastia Osteoporosis Epidemiology
• features unique to Graves’ dz are highlighted in blue Usually 30-50 YO
• Important complications Genetic factors: a/w HLA-B8, DR3 & DR2
• Stigmata of hyperthyroidism: goitre, tremors, lid lag/retraction, myopathy Trigger: ?viruses / bacteria (E. coli & Yersinia enterocolitica – may possess cell-membrane
TSH receptor, causing cross-reactivity of Abs vs host TSH receptor)
Causes a/w IDDM & pernicious anaemia
cause of >90% of hyperthyroidism in Singapore
• Graves’ disease • Iodide induced (eg amiodarone,
• MNG contrast dye)
• Toxic adenoma • Factitious hyperT4 Features
• Thyroiditis (subacute / de Quervain’s, or • TSH induced (eg chorioCA, Diffuse thyroid enlargement + thrill / bruit. May be nodular
post partum) hydatidiform mole) Ophthalmopathy
• Follicular CA ∼ Lid retraction ∼ Proptosis
∼ Excessive lacrimation ∼ Loss of visual acuity ± visual field defect
Investigations ∼ Conjunctivitis due to corneal oedema or optic n.
∼ Corneal ulceration (due to increased compression
TFT Free T3 & T4, TSH
exposure) ∼ Diplopia
TRAb Stimulating TSH-receptor Ab in Graves’ disease (>90%). May also be
Pretibial myxoedema (rare): raised pink / purplish plaques on anterior shin to dorsum of foot.
blocking causing hypothyroidism
a/w pruritis, peau d’orange and coarse hair
Other Abs Anti-Thyroid Peroxidase Ab (TPO) & anti-Thyroglobulin Ab (TgAb) – high
levels are suggestive of GDz, Hashimoto’s, silent thyroiditis or post-
2. Pathogenesis Papilloedema, loss of visual acuity or visual field defect: Urgent Rx with Prednisolone
TRAb (TSH-receptor IgG Abs) vs thyroid follicular cell stimulates thyroid hormone production 60mg daily. Surgical orbital decompression if no improvement.
Ophthalmopathy & dermopathy: immunologically mediated proliferation of fibroblasts which
secrete hydrophilic glycosaminoglycans causing increased interstitial fluid content + chronic
inflammatory cell infiltrate (usually lymphocytic). May cause optic nerve compression.
Clinical course MNG
Usually women around 60 YO
1. Prolonged periods of ↑T4 of fluctuating severity a/w AF and cardiac failure due to older age group
2. Periods of relapses and remission of ↑T4 Rx:
3. Single short-lived episode with prolonged remission ± eventual onset of ↓T4 1. Radioiodine – hypoT4 less common
2. Partial thyroidectomy – for tracheal compression or retrosternal extension of goitre
Assoc. Non-specific Biochemical Abnormalities 3. Antithyroid drugs NOT useful as relapse occurs after drug withdrawal.
LFT: ↑ bilirubin, ALT, AST, GGT, ALP
Mild ↑ Ca
Glycosuria Toxic Adenoma
Follicular adenoma autonomously secreting excess thyroid hormone – negative feedback
Management inhibits TSH secretion and causes atrophy of the rest of the thyroid gland.
1. Carbimazole Usually females >40YO
Inhibit tyrosine iodination + immunosuppression (↓ serum TRAb conc) Hyperthyroidism may be mild, and 50% have isolated elevation of T3 only (T3 thyrotoxicosis)
Duration: 6-18 mths then try stopping. Consider other Rx if relapse occurs (70%) Rx: Hemithyroidectomy, radioiodine. Post-Rx hypoT4 uncommon due to compensation of
Onset of efx: 3-12 wks. Meanwhile, use propanolol for symptomatic control remaining thyroid gland. Antithyroid drugs not useful as relapse invariably follow drug
2 dosing strategy: either give just enough CBZ to keep PT euthyroid, or give excess CBZ withdrawal.
& correct hypothyroidism with L-thyroxine replacement
ADR: **Agranulocytosis (reversible, requires WBC monitoring. Stop drug and consult Dr Subacute (de Quervain’s) Thyroiditis
immediately in the event of a sore throat / fever!), rash, cholestatic hepatitis, Virus induced (Coxsackie, mumps, adenovirus) thyroid inflammation.
thrombocytopenia, vasculitis, lupus-like syndrome Usually females 20-40YO
Preferred over propylthiouracil due to lower dose (once daily vs tds dosing) a/w pain radiating to angle of jaw and ears, worse on swallowing, coughing, neck movt.
2. Subtotal thyroidectomy Tender enlarged thyroid
Change antiT4 drug to potassium iodate PO 2 wks pre-Sx: short term inhibition of thyroid Raised thyroid hormone levels for 4-6 wks followed by asymptomatic hypoT4. Full recovery
hormone release and reduce gland size and vascularity within 4-6 mths
Outcome 1 yr post-Sx: 5% ↑T4, 15% permanently ↓T4, 80% euthyroid. Late onset ↓T4 or Rx: Aspirin / NSAID for pain, propranolol for ↑T4 symptoms, ± prednisolone.
↑T4 common, therefore require continued follow-up.
3. Radioiodine Post-partum Thyroiditis
Unmasking of subclinical autoimmune thyroid disease
Indications: failed medical/Sx Rx, PT w cardiac dz, PT’s preference
4-12 wks for onset of effects Usually presents with ↑T4 symptoms for the first time within 6 mths post-partum.
Recurs in subsequent pregnancies, progressing to permanent hypoT4 in the long term.
Interim symptom control with β-blocker or carbimazole
Rx: Propranolol.
No a/w ↑ freq of malignancy or congenital malformation in offspring
st
Majority devt hypothyroidism (50% in 1 yr) – need f/u with TFT & thyroxine replacement
CI: pregnant, breastfeeding, severe Graves’ Ophthalmopathy (may worsen it)
4. β-blocker (eg propranolol) Indications for surg:
For short term alleviation of symptoms. • Thyrotoxicosis not controlled by drugs
Useful for pre-thyroidectomy, or before onset of effects of radioiodine or carbimazole • Compressive symps
5. Ophthalmopathy • CA
Eyedrops / glasses + side shields • Cosmesis
Lateral tarsorrhaphy – for corneal ulceration
Extra-ocular muscle Sx: for persistent diplopia. Alternative: prism glasses.
3. Special Problems in Hyperthyroidism Drugs
1. β-blockers IV esmolol, or IV / PO propranolol
Hyperthyroidism & Pregnancy 2. PTU (propylthiouracil) Blocks iodination and conversion of T4 to T3
↑T4 usually cause anovulatory cycles and infertility 3. Iodine solution Inhibit thyroid hormone release
Carbimazole: crosses placenta causing treats fetus which is exposed to TRAb as well. Use 4. Dexamethasone IV 2mg for glucocorticoid support & to block conversion
smallest dose possible to prevent fetal hypothyroidism & goitre of free T4 to T3
Breastfeeding: use PTU which is excreted in breast milk to a lesser extent c.f carbimazole. 5. Treat CVS Cx accordingly Eg digoxin, diuretics
Radioiodine: absolute CI – causes fetal hypothyroidism. 6. Carbimazole Long term control of ↑T4 with carbimazole.
Atrial Fibrillation
Dysrhythmias present in 10% of thyrotoxic patients. Increasing incidence with age.
Establish euthyroidism, then consider cardioversion (establish stable sinus rhythm in 50%). Thyrotoxic periodic paralysis
β-blocker helps control ventricular rate as well. • Periodic weakness a/w hypo K - Cause of hypoK is due to K shift intracellularly
Anticoagulation: aspirin in the elderly, warfarin in younger PTs and those with Cardiomegaly • usu Asian males, onset in early adulthood
/ atrial thrombus. • episodic limb weakness lasting hrs to days
• weakness ppted by exercise, onset usu at night during sleep (after strenuous exercise)
• strength normal btwn attacks
• ECG: ST depression, flattened T waves, U waves
Thyroid Storm
Presentation
Fever From underlying sepsis or thyroid storm (uncontrolled ↑T4 /
post-subtotal thyroidectomy / post-radioiodine Rx)
Agitation / confusion
Tachycardia / AF
Accentuated thyrotoxic S/S LOW, tremors etc
Multiorgan dysfunction CNS: altered mental state, confusion, agitation, coma etc
GI: abdo pain, diarrhoea, vomiting
CVS: AF, heart failure, hyper/hypotension
Volume depletion From fever, diarrhoea and increased metabolism
S/S of precipitating event Eg sepsis, recent surgery
Management
Supportive
1. High flow O2
2. Monitor ECG, vital signs q10mins, pulse oximetry Digitally signed by DR WANA HLA SHWE
3. IV lines and fluid Dextrose-saline with appropriate electrolytes. Beware of DN: cn=DR WANA HLA SHWE, c=MY,
precipitating heart failure. o=UCSI University, School of Medicine, KT-
Campus, Terengganu, ou=Internal
4. Lab invxs FBC Medicine Group, email=wunna.
U/E/Cr hlashwe@gmail.com
LFT Reason: This document is for UCSI year 4
students.
TFT Date: 2009.02.24 14:01:08 +08'00'
CXR: heart failure and infection
ECG; ischaemia, infarction or dysrrhythmia
Urinalysis ± C/S if sepsis suspected
5. Correct precipitating factors eg sepsis, MI
6. Relieve fever Paracetamol, tepid sponging