shoulder injury.pptx
•Télécharger en tant que PPTX, PDF•
0 j'aime•51 vues

shoulder limb injury and its measurment traction and fracture of upper limb &splints provided.

Recommandé
Recommandé
Contenu connexe
Similaire à shoulder injury.pptx
Similaire à shoulder injury.pptx (20)
Dernier
Dernier (20)
shoulder injury.pptx
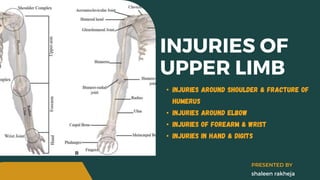
- 1. INJURIES OF UPPER LIMB • Injuries around shoulder & fracture of humerus • Injuries around elbow • Injuries of forearm & wrist • Injuries in hand & digits shaleen rakheja PRESENTED BY
- 2. 1 Fracture of clavicle 2 Fracture of scapula 3 Dislocation of sternoclevicular joint 4 Subluxation of acromioclavicular joint 5 Dislocation of shoulder 6 Fracture of surgical neck of humerus 7 Fracture of grater tuberocity of humerus 8 Fracture of shaft of humerus INJURIES AROUND SHOULDER & HUMERUS
- 3. • It comprises of clavicle, scapula & humerus • The articulation gives unique ROM in all directions SHOULDER GIRDLE • • • • • g l e n o h u m e r a l j o i n t • a c r o m i o c l a v i c u l a r j o i n t • s t e r n o c l a v i c u l a r j o i n t • s c a p u l o t h o r a c i c j o i n t
- 4. • It is only long bone with membranous ossification having two primary centers • medial 2/3 is convex anteriorly and lateral 1/3 is concave ant. • stability provided by acromioclavicular ligament & coracoclavicular ligament attached at conoid tubercle, trapezoid CLAVICLE BONE . muscle attachment site
- 5. • The scapula or shoulder blade is the bone that connects the clavicle to the humerus. • The scapula forms the posterior of the shoulder girdle. • It is a sturdy, flat, triangular bone. SCALPULA BONE . Intrinsic muscles : rotator cuff muscles, teres major, subscapularis, teres minor, infraspinatus(These assist with abduction & externalinternal rotation of the glenohumeral joint) Extrinsic muscles: triceps, biceps, & deltoid. Third group of muscles: levator scapulae, trapezius, rhomboids & serratus anterior (responsible for rotational movements & stabilization of the scapula)
- 6. • The proximal end of humerus consists of the head articulating with the glenoid cavity of the scapula. • The head is separated from the greater and lesser tuberosities by Anatomical neck • The globular upper end of the bone joins the tubular shaft of the bone is called the Surgical neck HUMERUS BONE .
- 7. Pathoanatomy Treatment • common site: at the junction of the middle & outer-1/3 of the clavicle • the outer fragment displace medially & downward by gravity & pectoralis major muscle. • inner fragment displace upwards by sternocleidomastoid muscle • Fracture unite readily, reduction of fragment is not essential • Triangular sling, Figure-of-8-bandage(young adults) is sufficient Back to Agenda 05 Fracture of clavicle Early complication: the fracture fragment may injure the subclavian vessel or brachial plexus
- 8. Pathoanatomy Treatment • less common, not much treatment is required • bone break at four sites: body, neck, acromion process & coracoid process • fracture is undisplaced because the fragments are held in together by surrounding muscles • treatment is to restore shoulder mobility and reduce pain • Triangular sling{usually 1 week-10 days}, Figure-of-8- bandage(young adults) is sufficient Back to Agenda 05 Fracture of scapula
- 9. Back to Agenda 05 Dislocation of sterno-clavicular joint • rare injury, medial end of clavicle is displaced forward or backward • diagnosis by clinically, x-ray • treatment by reduction using direct pressure over dislocated part & Figure-of-8- bandage for stabilization Subluxation/Dislocation of Acromioclavicular joint • uncommon injury may result in partial or complete rupture of acromioclavicular ligament or coracoclavicular ligaments. • ACJ divide into Grade 1,Grade 2 & Grade 3 • G 1&2 are treated by triangular sling, G3 by surgical repair
- 10. PREGLENOID SUBCORACOID SUBCLAVICULAR INTRATHORASIC Anterior dislocation DISLOCATION OF SHOULDER 07 • This is the most common injury of upper limb due to large head of humerus is not stable in the glenoid more likely to dislocate. It occurs more in adults than in children. Anterior dislocation is is much more common than posterior dislocation. • Clinically the patient will appear with abducted & externally rotated arm. • MDI{multidirectional intability}-anterior, inferior, posterior dislocation PATHOANATOMY
- 11. • posterior dislocation: The head of the humerus comes to lie posteriorly bhind the glenoid • inferior dislocation(luxatio erecta): head comes lie in subglenoid position BANKART'S LESION HILL-SACHS LESION pathological changes Dislocation of shoulder Anterior inferior labrum tear A dent on humeral head Tear of top of the labrum
- 12. Diagnosis Treatment Reduction technique • Dugas' test: instability to touch opposite shoulder. • Hamilton ruler test: because of dislocation shoulder is flattened, the ruler will touch the acromion & lateral condyle of humerus simultaneously. • posterior & anterior dislocation will appear in lateral view x-ray • clinical assessment, reduction, anesthesia • chest arm bandage for 3 weeks • Kocher's manoeuver : • Traction • External rotation • Adduction • Internal rotation Early complication: Injury to axillary nerve may result in paralysis of the deltoid muscle Dislocation of shoulder
- 13. Pathoanatomy Treatment • more common in elderly people usually due to fall on shoulder • fracture is of 4 types: • shaft • head • grater tuberosity • lesser tuberosity • open reduction & internal fixation • arm abduction orthosis can be prescribed Back to Agenda 05 Fracture of the surgical neck of the himerus complication: Axillary nerve palsy and shoulder stiffness
- 14. Pathoanatomy Treatment • It occurs in adults, due to fall on shoulder, displaced & comminuted, sometimes it widely separated by muscle pull (supraspinatus muscle) • fracture reduced by holding the shoulder abducted in plaster cast, or by open reduction & internal fixation Back to Agenda 05 Fracture of the greater tuberosity of the humerus complication: Painful arc syndrome and shoulder stifness
- 15. Pathoanatomy Treatment • types: • Transverse fracture. • Oblique fracture. • Spiral fracture. • Segmental fracture. • Comminuted fracture. • Impacted fracture. • Buckle fracture. • Hairline fracture. • If your fracture is mild and your bones did not move far out of place (if it’s non-displaced), you might only need a splint or cast. Splinting usually lasts for three to five weeks. If you need a cast, it will likely be for longer, typically six to eight weeks. In both cases, you’ll likely need follow-up X-rays to make sure your bones are healing correctly. • You might need a sling to hold your shoulder and arm in place, especially if your humerus is fractured at the proximal end near your shoulder. Back to Agenda 05 Fracture of the shaft of humerus complication: radial nerve injury,delayed union & non union
- 16. humeral fracture brace The use of humeral fracture braces has become our preferred method of treatment for fractures of the shaft of the humerus. These braces are easy to apply and adjust; the patient's acceptance of this method of treatment is high. We compared this method of treatment with the traditional method of plaster U- slab immobilization. A group of patients treated with a plaster U-slab were matched for type and level of fracture with a group treated with a humeral fracture brace and compared with regard to fracture healing and functional outcome. There was no difference between groups for healing time and final alignment of the fracture. However, there was a greater range of elbow motion at the time of union in the fracture brace group (11 degrees-126 degrees) compared with the U-slab
- 17. 1 Supracondylar fracture of humerus 2 Fracture of the lateral condyles of humerus 3 Intercondylar fracture of humerus 4 Fracture of medial epicondyle of the humerus 5 Dislocation of elbow 6 Pulled elbow 7 Fracture of olecrone 8 Fracture of neck of radius 9 Fracture of capitulum INJURIES AROUND THE ELBOW
- 18. 1 Fracture of the forearm bone 2 Monteggia fracture dislocation 3 Galeazzi fracture disloction 4 Colle's fracture 5 Smith fracture 6 Barton's fracture 7 Scaphoid fracture 8 Lunate dislocation INJURIES OF THE FOREARM & WRIST