
Recommandé
Contenu connexe
Similaire à 9menengitis.ppt
Similaire à 9menengitis.ppt (20)
Dernier
Dernier (20)
9menengitis.ppt
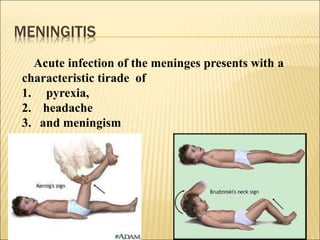
- 1. MENINGITIS Acute infection of the meninges presents with a characteristic tirade of 1. pyrexia, 2. headache 3. and meningism
- 3. BACTERIAL MENINGITIS Acute infection of the meninges presents with a characteristic triade of 1- pyrexia, 2- headache 3-and meningism Meningeal signs : 1- stiffness of the neck 2- Kernig's sign (with the hip joint flexed, extension at the knee causes spasm in the hamstring muscles) 3- Brudzinski's sign (passive flexion of the neck causes flexion of the thighs and knees). Etiology
- 4. MOST CAUSATIVE ORGANISM ACCORDING TO AGE: Neonate E. Coli and Group B Strept , Listeria monocytogens Infants H. Influenza, N. meningitidis . Pneumococcus Teens/ young adults N. Meningitidis /H. Influenza, Pneumococcus Elderly Pneumococcus, N. Meningitidis /H. Influenza, Viral infection is the most common cause of meningitis, and usually results in a benign and self-limiting illness requiring no specific therapy
- 5. Clinical features stiff neck, headache, fever, photophobia, vomiting, irritability, impairment of consciousness, confusion, seizures and, morelikely in pneumococcal meningitis, focal neurological signs and symptoms. Meningism is present in the majority of patients, in deeply comatose patients this meningism might be absent as it may be in the very early stage of the disease or in very elderly patients. The clinical signs and symptoms evolve rapidly, within few or several hours, in some instances bacterial meningitis may also have a more sub acute presentation (more typically in pneumococcal meningitis). The detection of petechiae or a purpura fulminans on presentation is highly suggestive of N. meningococcal infection
- 7. CSF ANALYSIS
- 9. Cell count with differential, Glucose and protein concentration Stain and culture 1. Gram’s stain and bacterial culture 2. India ink and fungal culture 3. Viral culture 4. Acid fast smear and M. tuberculosis culture Polymerase chain reaction 1. Broad range bacterial PCR (16S ribosomal DNA) 2. Specific meningeal pathogen PCR 3. Reverse transcriptase PCR for enteroviruses 4. PCR for herpes simplex virus type 1 and 2 5. PCR for West Nile V 6. PCR for Epstein Barr virus 7. PCR for varicella zoster V 8. PCR for M. tuberculosis 9. PCR for HIV RNA
- 10. Antigens 1-- Cryptococcal polysaccharide antigen 2-- Histoplasma polysaccharide antigen Antibodies 1. Herpes simplex virus (serum and CSF IgG to calculate antibody ratio) 2. Varicella zoster virus IgM, and IgG antibody index 3. Arthropod-borne viruses (West Nile virus IgM) 4. Borrelia burgdorferi antibody index 5. C. immitis complement fixation antibody 6. HHV-6 IgM
- 11. Meningococcal infection purulent meningitis 50% sepsis syndrome in 25-35% both sepsis and meningitis 15% fulminating meningococcal septicemia, 10% Diagnosis -Elevated CSF cell count (>1000 WBC/μl, with more than 60% PMN) -Elevated total protein content (>120mg/dl) -Low CSF glucose concentration (CSF blood glucose ratio of less than <0,3) -Identification of the bacterial pathogen in the CSF culture – CSF, blood, skin biopsy microscopy of a gram stained smear antigen detection (latex particle agglutination test) Polymerase chain reaction (PCR) techniques can be used on both blood and CSF to identify bacterial DNA
- 12. Cerebral complications Brain edema with the risk of herniation Arterial vascular complications: arteritis, vasospasm, focal cortical hyperperfusion, altered cerebrovascular autoregulation Septic sinus/venous thrombosis (in particular of the superior sagittal sinus) and Cortical thrombophlebitis Hydrocephalus Cerebritis Subdural effusion (in infants and children) Rarely as a consequence of meningitis: brain abscess, subdural empyema Vestibulocochlear involvement purulent labyrinthitis Extracranial complications myocarditis Septic shock Disseminated intravascular coagulation Adult respiratory distress syndrome (ARDS) Arthritis (septic or reactive) Electrolyte disturbances (hyponatremia, syndrome of inappropriate ADH secretion (SIADH) or, rarely, central diabetes insipidus) Spinal complications (e.g. myelitis, infarction) complications
- 13. Therapeutic management Empiric antimicrobial chemotherapy initiate an antibiotic therapy without microbiological confirmation (neither by gram stain nor by culture) Recommended antibiotic microorganism Age Cefotaxime plus ampicillin, or ampicillin plus aminoglycoside E. coli, Klebsiella, Enterobacter, Proteus) L. monocytogenes <1months Ceftriaxone, plus vancomycin S. pneumoniae, N. meningitidis , H. Influenzae,E. coli Preschool and young adult Ceftriaxone, plus vancomycin N. meningitidis, S. pneumoniae Listeria, Enterobacteriaceae Ceftriaxone plus vancomycin plus ampicillin S. pneumoniae, N. meningitidis, Listeria >50 years
- 14. Recommended antibodies Typical pathogens Clinical condition Ceftriaxone* plus vancomycin † plus ampicllin S. pneumoniae, N. meningitidis, L. monocytogenes Healthy, immunocompetent (community-acquired) Ceftazidime (or meropenem) plus vancomycin ‡ or fosfomycin Staphylococci, Enterobacteriaceae, P. aeruginosa Nosocomial (e.g. post- neurosurgical Or posttraumatic brain injury) = = shunt infection
- 15. N. meningitidis =======Penicillin G=== Ceftriaxone (or cefotaxime), Ampicillin, rifampin S. pneumoniae, penicillin susceptible=== Penicillin G (or Ampicillin) ====Ceftriaxone (or cefotaxime) Meropenem, cefepime H. Influenzae Group streptococci==== Ceftriaxone (or cefotaxime) Penicillin G (± gentamicin)=====Ampicillin plus chloramphenicol Ceftriaxone, Ampicillin (plus gentamicin), vancomycin Meningococci 7 days Haemophilus influenzae type B 10-14 days Pneumococci 14 days Listeria monocytogenes >3 weeks Gram negatives >3 weeks
- 16. Adjunctive therapy Corticosteroids management of increased intracranial pressure anticonvulsants Chemoprophylaxis recommended for all people of the same household Rifampicin (2x600mg/day for 2 days) is the drug most often recommended for chemoprophylaxis, alternatives are ciprofloxacin (500mg orally once), or Ceftriaxone (250-500mg i. m. once) chemoprophylaxis is also recommended for the index patient at the time of discharge f Vaccination Haemophilus influenzae type B serogroup C meningococcal meningitis pneumococcal vaccine
- 17. I. recommended for patients with terminal complement component deficiency, II. asplenia, III. travellers to areas with epidemic meningococcal disease (so- called meningococcal meningitis belt). IV.splenectomised patients (or with functional asplenia), V. chronic debilitating diseases VI.such as diabetes mellitus VII. with posttraumatic CSF leakage.
- 18. TUBERCULOUS MENINGITIS Tuberculous meningitis, Tuberculoma, or Tuberculous involvement of the spine with myelopathy (Pott's disease) M. tuberculosis and M. bovis Clinical Features low-grade fever, headache, and intermittent nausea and vomiting, followed by more severe headache, neck stiffness, altered mentation, and cranial (usually III, but also II, VII, and VIII) nerve palsies meningeal signs, seizures, and focal neurological deficits, including hemiparesis, increasing drowsiness, and signs of increased ICP choroidal tubercles
- 19. TUBERCULOSIS MODE OF TRANSMISSION: haematogenous dissemination of Mycobacterium tuberculosis from primary pulmonary infection brain and spinal cord sub-pial and sub-ependymal foci of infection (Rich foci) I. rupture and release bacteria into the subarachnoid space causing meningitis II. enlarge to form tuberculomas without meningitis
- 20. Diagnosis. tubercle bacilli on CSF acid-fast bacilli (AFB) smear or culture CSF culture results are positive for M. tuberculosis in 45-70% of patients but may take 6-8 weeks to become positive. CSF examination demonstrates normal or elevated opening pressure, elevated protein {80^400 mg/dL), low glucose (<40 mg/dL), and pleocytosis (averaging 200-400 ]WBC/dL with lymphocytic predominance Tuberculomas, the parenchymal form of TB, occur as single or multiple brain or spinal cord lesions and present with signs and symptoms of space- occupying lesions. polymerase chain reaction (PCR) technique has been applied and is now routinely available for the diagnosis of TB meningitis, with reported sensitivities of 70-75%.
- 21. The diagnostic yield of Nucleic Acid Amplifection [NAA] increases when large volumes of CSF are processed. NAA tests are more useful than conventional bacteriology after the start of anti-tuberculosis treatment. NAA assays can detect the rifampicin resistance genotypes CSF adenosine deaminase activity is not recommended as a routine diagnostic test for CNS tuberculosis . The tuberculin skin test and IGRAs (using peripheral blood) may provide indication of previous tuberculosis Interferon-gamma release(QuantiFERON-TB gold and T-SPOT.TB), are more accurate than skin testing at diagnosing latent tuberculosis
- 22. TB MENINGITIS RADIOLOGICAL TESTS The brain of every patient with TBM should be imaged with contrast enhanced CT either before the start of treatment(as part of the diagnostic work-up), or within the first 48 h of treatment All patients with suspected cerebral tuberculoma or spinal cord tuberculosis should be investigated by MRI which may show: 1. Communicating hydrocephalus 2. 40% vasculitis 3. Basal enhancement 4. Tuberculoma 5. Spinal = T1 isointense enhances with Gd
- 23. 50% of patients with TBM have chest X-rays suggesting active or previous pulmonary tuberculosis Chest CT may reveal abnormalities missed by CXR The commonest cerebral CT features of TBM are hydrocephalus and basal contrast enhancing exudates Infarctions as a result of ongoing vasculitis or tuberculoma are found in approximately 20% of patients at presentation Infarctions most commonly involve the basal ganglia and the territories of the medial striate and thalamoperforating arteries magnetic resonance spectroscopy (MRS) large lipid CH2 peak and choline/creatine ratio >1 Patients should be treated for a minimum of 12 months
- 24. Isoniazid (INH) .5-10 (max 300 mg) PO, add pyridoxine to prevent neuropathy (Child 25 mg/kg/day PO, Adult 50 /mg/kg/day PO) side effect Hepatitis (1-2%), neuropathy (5%), seizures Rifampin (RIF) Child 15 PO, Adult 10 PO" side effect Hepatitis (1-2%), Pyrazinamide 25 (max 2.5 g/day) PO Arthralgia (5%!, hepatitis (1-5%), hyperuricemia, gout, rash Streptomycin Child 30 IM Adult 15 (max 1 g/day) IM Hearing loss, vestibular imbalance (1-5%) Ethambutol 15-25 (max 2.5 g/day) PO Optic neuritis (3%), neuropathy (1-2%), rash
- 25. During treatment CSF is reexamined to monitor treatment efficacy and drug levels. Neuro imaging studies are performed 2-3 months after the start of treatment and again at 3- to 6-month intervals to verify improvement in lesions. Two years of treatment may be necessary for tuberculomas. Chemotherapy alone is effective treatment for most spinal TB without cord involvement. Complications. Progressive hydrocephalus damage to the optic nerves and chiasm in the suprasellar cistern causes blindness the syndrome of inappropriate secretion of antidiuretic hormone vasculitis; stroke; arachnoiditis; spinal cord atrophy; and syringomyelia. 2 1% mortality rate for immunocompetent patients and 33% for HIV-infected patients
- 26. Direct involvements VIRAL INFECTIONS meningitis encephalitis (acute or chronic forms such as subacute sclerosing panencephalitis [SSPE]), myelitis, ganglionitis, polyradiculitis post infectious CNS inflammatory or autoimmune syndromes, such as acute disseminated encephalomyelitis (ADEM) Indirect involvements Herpes viruses 1. HSV-type 1 and type 2 2. Varicella zoster virus (VZV), 3. Cytomegalovirus (CMV), 4. Epstcin-Barr virus (EBV), 5. Human herpes viruses {HHV-6, HHV-7, and HHV-S), 6. the simian {"monkey") Herpes B-virus.
- 27. Herpes Simplex Encephalitis (HSE), HSV-1 is the most common viral cause of acute sporadic encephalitis 1. fever, 2. headache, 3. altered level of consciousness 4. behavioral changes, 5. an amnestic syndrome 6. focal or multifocal neurological deficit 7. focal or generalized seizure activity 8. hallucinations, particularly olfactory hallucinations The diagnosis of HSE should be considered in any febrile patient with an altered level of consciousness
- 28. Examination of cerebrospinal fluid (CSF) Lymphocytic pleocytosis of 10-1000 white blood count (WBC) Virus may be cultured from the CSF in less than 5% of cases HSV DNA can be detected in the CSF with polymerase chain reaction (PCR) techniques. CSF PCR testing has an estimated sensitivity of greater than 95% and a specificity approaching 100% CT and magnetic resonance imaging (MR1) focal abnormalities in fronto-temporal regions Electroencephalogram (EEG) diffuse slowing, focal abnormalities in the temporal regions, or periodic lateralizing epileptiform discharges (PLEDS). Brain biopsy the diagnosis remains in question or those who respond poorly to treatment Therapy Acyclovir[10] mg/kg every 8 hours for[ 14-21] Dosing should be adjusted appropriately in patients with renal insufficiency. Treatment with acyclovir reduces mortality of HSF from 70% to 20% Foscarnet
- 30. Viral encephalitis Tick borne encephalitis Fever, malaise, stiff neck, sore throat, and nausea and vomiting, progressing to stupor, coma, and convulsions. Signs of an upper motor neuron lesion (exaggerated deep tendon reflexes, absent superficial reflexes, pathologic reflexes, and spastic paralysis Cerebrospinal fluid protein and opening pressure often increased, with lymphocytic pleocytosis. Mosquito-borne Eastern equine Venezuelan equine St. Louis Japanese B Murray Valley West Nile Tick-borne complex Far Eastern Central European Russian spring-summer
- 31. AUTOIMMUNE ENCEPHALOPATHY Sub acute encephalopathy Cognitive and behavioral deficit Toxic ,Metabolic and infectious causes should be excluded Elevated CSF protein with normal cells Presence of certain serum and CSF auto antibodies Rapidly progressive causes of dementia should be excluded