Circulatory Shock, types and stages, compensatory mechanisms
Rhythm 43, 44, 50 sspresentation
1. Names of Students: Tamara A. Lewis, Heeyeon Lim, Sushil Sharma
Your Answers
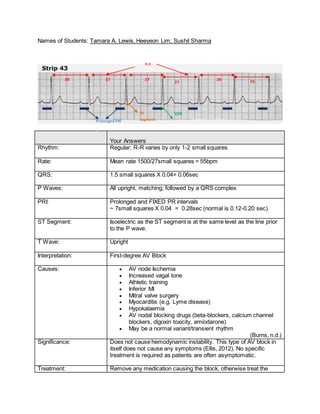
Rhythm: Regular; R-R varies by only 1-2 small squares
Rate: Mean rate 1500/27small squares = 55bpm
QRS: 1.5 small squares X 0.04= 0.06sec
P Waves: All upright, matching; followed by a QRS complex
PRI: Prolonged and FIXED PR intervals
~ 7small squares X 0.04 = 0.28sec (normal is 0.12-0.20 sec)
ST Segment: Isoelectric as the ST segment is at the same level as the line prior
to the P wave.
T Wave: Upright
Interpretation: First-degree AV Block
Causes: AV node Ischemia
Increased vagal tone
Athletic training
Inferior MI
Mitral valve surgery
Myocarditis (e.g. Lyme disease)
Hypokalaemia
AV nodal blocking drugs (beta-blockers, calcium channel
blockers, digoxin toxicity, amiodarone)
May be a normal variant/transient rhythm
(Burns, n.d.)
Significance: Does not cause hemodynamic instability. This type of AV block in
itself does not cause any symptoms (Ellis, 2012). No specific
treatment is required as patients are often asymptomatic.
Treatment: Remove any medication causing the block, otherwise treat the
QRS
~1.5 small squares
Prolonged PRI
=7 small squares
ST
segment
R-R
27 small squares
28 27 27 26 2627
2. underlying cause.
First-degree AV Block
Atrioventricular blocks are a result of an interruption in the conduction of impulses between the
atria and the ventricles. The block can be delayed, partial/total; temporary/permanent.
In First-degree AV block all atrial impulses reaches the ventricles however there is a consistent
delay in the conduction of the impulse at the AV node, as a result PRI is >0.20 on an EKG. 1st
degree AV blocks are considered a benign rhythm as they do not generally cause symptoms
(Ellis, 2012). The rhythm may be transient and is managed by removing the medication or other
causing the rhythm. Although 1st
degree AV blocks are benign it is important to monitor your
patient for worsening AV block (Ellis, 2012).
3. Names of Students: Heeyeon Lim, Sushil Sharma, Tamara A. Lewis,
Your Answers
Rhythm: Irregular
(QRS complexes clustered into groups of 2 separated by a short
pause)
Rate: (1500/23-41small blocks)
HR 37-63bpm with a mean rate of 50 bpm
QRS: Present and upright
2 x 0.04 = 0.08 sec
P Waves: Upright, uniform, some followed by QRS, some non-conducted.
PRI: Present but prolonged (>0.2seconds). Varies with 0.24-0.40sec.
Progressively lengthens until non-conducted P wave (no QRS
followed by P-wave)
ST Segment: Isoelectric
T Wave: Present; Upright and matching, but slightly peaked in shape
Interpretation: Mobitz 1 second-degree AV Block (Wenckebach)
Causes: MI (most commonly inferior MI)
Medication side-effect: beta-blockers, digoxin, calcium
channel blocker, admiodarone
Increased parasympathetic (vagal) tone (i.e. athletes
especially during sleep)
Myocarditis
Following cardiac surgery
(Burns, n.d. & Muma & Ritter,2011)
Lengthening of
PRI
R-R
No QRS following
P wave
ST
segmentQRS
4. Significance: Usually a benign rhythm, causing minimal effect on hemodynamic
stability and unlikely to progress into third degree heart block
(Burns, n.d.)
Treatment: Asymptomatic
Patients do not require treatment
Cautious monitoring
Administer oxygen to help with heart’s workload
Symptomatic
Treat underlying causes
Transcutaneous pacing if decreased cardiac output or
bradycardic
Administer atropine-with extra caution if MI suspected
Monitor for worsening symptoms
(Ellis, 2012 & Muma & Ritter, 2011)
Mobitz I Second-degree AV block
In Mobitz type 1 second-degree AV block (Wenckebach), the sinus impulses progressively
weakens and consequently the AV conduction time increases over several heartbeats until it is
finally unable to send the impulse down to ventricle. This is represented in ECG as P wave
becoming progressively longer until there is no QRS complex after P-wave. Ventricular rate is
slower than atrial rate to some extent because some of impulses are non-conducted. This type
of block usually lasts only a few days (Ellis, 2012). However, cautious monitoring is indicated as
patients may experience symptoms associated with decreased cardiac output or bradycardia.
Also, this condition may indicate potential MI. As well, although unlikely, it may progress into
more serious heart block such as third-degree AV block.
5. Names of Students: Sushil Sharma, Tamara A. Lewis, Heeyeon Lim
Your Answers
Rhythm: Regular
Rate: 40 bpm
QRS: 0.08 sec
P Waves: Present. More p waves than QRS
PRI: Constant on the conducted beat; 0.20 sec
ST Segment: Isoelectric
T Wave: Present and upright
Interpretation: 2:1 AV Block
Causes: Beta blockers, digoxin, ischemia to AV node due to an MI
Significance: Decrease cardiac output due to decreased ventricular HR, chest
pain, SOB. May progress to third degree heart block.
Treatment: - atropine effective only if block is at AV node
- Epinephrine to increase heart rate
- Temporary or permanent pacemaker
Mobitz II second-degree AV block
In Second-degree AV blocks there are intermittent non-conducted p waves, with NO
progressive prolongation of the PRI, some of the sinus impulses are prevented from reaching
the ventricles (Ellis, 2012). According to Burns n.d. and Ellis, 2012, Mobitz II is usually due to
structural damage. That is, patients usually already have a pre-existing bundle branch blocked
therefore, when the second branch becomes blocked the result is no sinus impulse being
conducted, resulting in intermittent missing QRS complexes. A block at the AV node results in
narrow QRS complexes <0.12 sec, while block at the bundle branch results in wide QRS
PRI
R-R
ST
segment
No QRS following
P wave
No QRS following
P wave
No QRS following
P wave
QRS
6. complexes >= 0.12 sec. (Ellis, 2012). There may also be a pattern to the conduction block, e.g.
2:1 or 3:1 (p to QRS).
This rhythm is more likely to be associated with hemodynamic compromise and progress to
third-degree heart block (Burns, n.d.). Treatment ultimately requires transcutaneous pacing.
Patients should be started on oxygen, and infusion of atropine or epinephrine or dopamine
infusion while waiting for pacemaker (Ellis, 2012).
Note: For BBB, indicative with QRS complexes >=0.12 sec, atropine is ineffective as it acts at
the level the AV node and above to speed up rate of sinus impulse.
Fixed ratio AV blocks (2:1 AV blocks)
These are types of second degree AV blocks with a fixed ratio of p waves: QRS complexes.
They may be a result of either Mobitz I or II (Ellis, 2012; Burns n.d.). It is not always possible to
determine the type of conduction disturbance producing the fixed ratio block however Mobitz1
conduction blocks are more likely to have narrow QRS complexes while in Mobitz II the QRS
complexes are typically broad (Burns n.d.). According to Burns n.d. the only way to differentiate
whether a fixed ratio block is a result of Mobitz I vs II is to observe the patient’s cardiac rhythm
for a period of time and observe what happens with the PRI intervals, the longer the observation
time the more likely you will be able to discern whether there are interspersed runs of Mobitz I
sequences vs Mobitz II.
Third-degree AV block (complete heart block)
In third-degree AV block there is dissociation between the sinus node and the ventricles. None
of the impulses originating the sinus node ever reaches the ventricle due to conduction block at
the AV node or lower pacemakers, therefore while the sinus node is firing normally a lower
pacemaker is also providing an escape beat. The result is the atria and ventricles working
independently of each other. The PRI interval varies and again the size of the QRS interval
depends on where the block in occurring (>=0.12 if in BB; <0.12 if at AV node). This type of
block may be caused by an MI, conduction system lesion, medication or hypoxia (Ellis, 2012).
Patient’s with third-degree AV block typically have severe bradycardia and are at high risk of
ventricular standstill and sudden cardiac death (Burns n.d.). If patient is symptomatic treatment
requires immediate transcutaneous pacing and ultimately permanent pacemaker. As with
Mobitz I and II patients should be started on oxygen, and infusion of atropine or epinephrine or
dopamine infusion while waiting for a pacemaker (Ellis, 2012).
7. References
Burns, E. (n.d). AV Block: 1st Degree. Retrieved from http://lifeinthefastlane.com/ecg-
library/basics/first-degree-heart-block/
Burns, E. (n.d.). AV Block: 2nd
degree, Mobitz 1 (Wenckebach Phenomenon). Retrieved from
http://lifeinthefastlane.com/ecg-library/basics/wenckebach/
Burns, E. (n.d.). AV Block: 2nd
degree, “fixed ratio blocks” (2:1; 3:1). Retrieved from
http://lifeinthefastlane.com/ecg-library/basics/fixed-ratio-blocks/
Burns, E. (n.d.). AV Block: 2nd
degree, Mobitz II. Retrieved from http://lifeinthefastlane.com/ecg-
library/basics/mobitz-2/
Burns, E. (n.d.). AV Block: 3rd
degree (complete hear block). Retrieved from
http://lifeinthefastlane.com/ecg-library/basics/complete-heart-block/
Ellis, K. M. (2012). EKG plain and simple (3rd ed.). New Jersey: Pearson
Muma, L. & Ritter, B. (2011). EKG: Section Three. Retrieved from
http://www.usfca.edu/fac_staff/ritter/threeekg.htm
Na’im, M. (n.d.). Atrioventricular Block [ECG]. Retrieved from
http://www.jacknaimsnotes.com/2009/05/artrioventricular-block-ecg.html