
Recommandé
Contenu connexe
Tendances
Similaire à Sinusitis
Similaire à Sinusitis (20)
Dernier
Dernier (20)
Sinusitis
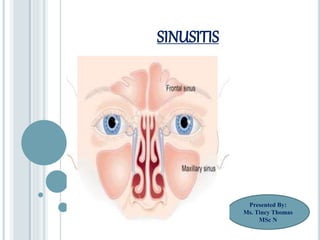
- 1. SINUSITIS Presented By: Ms. Tincy Thomas MSc N
- 3. INTRODUCTION: Sinuses are moist air spaces within the bones of the face around the nose. Sinuses are lined with the same mucus membrane that lines the nose and mouth. When a person has cold and allergies the sinus tissues make more mucous and become swollen. The drainage system for the sinuses get blocked and mucous can become trapped in these sinuses.
- 4. A complication of 5%-10% of URIs in children. Maxillary and ethmoid sinuses are most frequently involved. The sinuses are hollow air-filled sacs lined by mucous membrane. The ethmoid and maxillary sinuses are present at birth. The frontal sinus develops during the 2nd year and the sphenoid sinus develops during the 3rd year.
- 6. DEFINTION: Sinusitis is a condition consisting of inflammation of the paranasal sinuses, which may or may not be as a result of infection from bacterial, fungal, viral, allergic or autoimmune issues.
- 7. It is the inflammation of the Para nasal sinuses. It may be acute or chronic inflammation. It is an acute inflammatory process involving one or more of the paranasal sinuses.
- 8. CAUSES & RISK FACTORS: Bacteria, Fungi, Viruses. Bacterial Agents are Streptococcus pneumonia, Staphylococcus aureus, Haemophilus influenza and Moraxella catarrhalis. It is possible that constant exposure to inhaled allergens such as house dust mites, pets, mold and cockroaches may cause chronic inflammation of the nose and the sinuses.
- 9. PREDISPOSING FACTORS: Allergies, nasal deformities, cystic fibrosis, nasal polyps, and HIV infection. Cold weather Using decongestant nasal sprays too much Structural problems such as Deviated nasal septum High pollen counts
- 10. Adenoids, Infected tonsils or dental infections. Smoking. Infections such as small sinus Ostia, concha bullosa. Reinfection from siblings.
- 11. ETIOLOGY: 70% of bacterial sinusitis is caused by: Streptococcus pneumonia Haemophilus influenza Moraxella catarrhalis
- 12. Other causative organisms are: Staphylococcus aureus Streptococcus pyogenes, Gram-negative bacilli Respiratory viruses
- 14. SUBJECTIVE SYMPTOMS: History of URI or allergic rhinitis History of pressure change Pressure, pain, or tenderness over sinuses Increased pain in the morning, subsiding in the afternoon Malaise
- 15. Low-grade temperature Persistent nasal discharge, often purulent Postnasal drip Cough, worsens at night Mouthing breathing, snoring History of previous episodes of sinusitis Sore throat, bad breath Headache
- 16. CLINICAL PRESENTATION OF SINUSITIS: Periorbital edema Cellulitis Nasal mucosa is reddened or swollen Percussion or palpation tenderness over a sinus Nasal discharge, thick, sometimes yellow or green Postnasal discharge in posterior pharynx
- 17. Difficult trans illumination Swelling of turbinates Boggy pale turbinates
- 18. ACUTE SINUSITIS:
- 19. ACUTE SINUSITIS: Acute inflammation of sinus mucosa is usually precipitated by an earlier upper respiratory tract infection. Most cases of acute sinusitis start with a common cold which is caused by a virus. Colds can inflame sinuses and cause symptoms of sinusitis. If the inflammation produced by the cold leads to a bacterial infection.
- 20. When mucous present inside the sinuses and is unable to drain into the nose it becomes the source of nutrients to the bacteria. On rare occasions acute sinusitis can results in brain infections and other serious complications. The inflammation caused by the cold and nasal problems results in swelling of the mucous membranes of the sinuses, and this can lead to the trapping of air and mucous behind the narrow opening of the sinuses.
- 21. CLINICAL MANIFESTATIONS: Maxillary Sinusitis: It can cause pain or pressure in the maxillary area (cheek, jaw, gums and teeth) and cheeks become reddened, edematous and tender to the touch. Pain is aggravated on stooping or coughing. Frontal Sinusitis: It can cause pain or pressure in the frontal sinus cavity. Pain is localized over the forehead and the patient complains of frontal headache. The pain is severe in the morning and gradually subsides towards noon as the infected material get drained out from the sinus.
- 22. Ethmoid Sinusitis: In ethmoid sinusitis the pain is localized over the bridges of the nose, inner canthus and between or behind the eyes. Sphenoid Sinusitis: Sphenoid Sinusitis can cause pain or pressure behind the eyes but often refers to the vertex or occiput of the head
- 23. Malaise or tiredness Edema of eyelids Body ache Decreased sense of smell Tenderness on applying pressure Cough , severe at the night. Sore throat Bad breath Fever Mucopurulent nasal discharge
- 24. DIAGNOSTIC EVALUATION: History Collection Physical Examination X-ray examination of the paranasal sinuses Anterior and Posterior rhinoscopy reveals the congestion of nasal mucosa and presence of mucous in the nose. A Computed Tomography (CT scan).
- 25. MANAGEMENT: Antibiotic Therapy: The vast majorities of cases of acute sinusitis are due to viral etiology and thus resolves without antibiotics. If the symptoms are prolonged amoxicillin is a reasonable first choice. Amoxicillin or clavulanate (Augmentin) being indicated for the patients who fail amoxicillin alone. Fluoroquinolones and other antibiotics such as Clarithromycin and doxycycline are used in the patients who are allergic to pencillin.The course of the treatment is usually given for 10-15 days.
- 26. Nasal Decongestants: Use of decongestant agents such as pseudoephedrine and oxymetazoline helps in relieving the nasal obstruction and mucosal swelling thereby improving drainage of the sinuses. Guaifenesin, a mucolytic agent may also be effective in reducing nasal congestion.
- 27. Antihistamines: - If allergy is suspected along with sinusitis, antihistaminic drugs required to control allergies. This may include diphenhydramine, cetirizine, fexofenadine and a nasal steroid spray that reduces the swelling around the sinus passages and allows the sinuses to drain. Steam inhalation:- Medicated steam inhalations like Tr. Benzoin or menthol through the nose are soothing.
- 28. Conservative measures: - Over the counter medication such as acetaminophen or paracetamol and ibuprofen can relieve some of the symptoms associated with sinusitis such as headaches, pressure, fatigue and pain.
- 30. In chronic sinusitis the membranes of both the paranasal sinuses and the nose are thickened because they are constantly inflamed for more than 8 weeks. Chronic sinusitis is usually the result of incompletely resolved acute sinusitis. Nasal polyps are grape like growths of the sinus membranes that protrude into the sinuses or into the nasal passages. Polyps make it even more difficult for the sinuses to drain and for air to pass through the nose.
- 31. CLINICAL MANIFESTATIONS: Persistent nasal obstruction Nasal congestion due to the excessive nasal discharge Edema of the nasal mucous membrane Impaired mucociliary clearance Sore throat and dryness of throat Facial pain Headache Night time coughing
- 32. Increase in previously minor or controlled asthma symptoms. Thick green or yellow discharge Epitaxis Feeling facial fullness or tightness due to the presence of nasal discharge. Aching teeth or halitosis Anosmia Reduction in the ability to smell or detect odour. Dental infections
- 33. DIAGNOSTIC EVALUATIONS: History Collection X-ray examination of the paranasal sinuses Anterior and Posterior rhinoscopy Transillumination test Rhino scan Nasal Endoscopy Computed Tomography Magnetic resonance Imaging Blood tests Biopsy of the membranes
- 34. MANAGEMENT: Treatment of chronic sinusitis aims to help in the drainage of discharge from the sinus cavity and remove the predisposing factors. Broad spectrum antibiotics are given after the culture and sensitivity test. Amoxicillin clavulanate (Augmentin) or ampicillin, clarithromycin and third generation cephalosporines such as cefuroxime axetil, cefpodoxime and cefprozil have also been effective. Levofloxacin a quiolone may also been used.
- 35. Antibiotic therapy can be continued for 3-4 weeks. Use of local or systemic decongestants helps in relieving the nasal obstruction and mucosal swelling. Heated mist and saline irrigation also may be effective for opening blocked passages. Anti histamininic drugs and analgesics help to relieve the symptoms. Sometimes local medication in the sinus cavity is also instilled.
- 36. SURGICAL MANAGEMENT: When medicine fails surgery may be the only alternative for treating chronic sinusitis. The goal of surgery is to improve sinus drainage and reduce blockage of the nasal passages. During surgery which is usually done through the nose, the surgeon enlarges the natural openings of the sinuses removes any polyps and correct significant anatomic deformities that contribute the obstruction.
- 37. Antrum Puncture: In this procedure the trochar and cannula put under the inferior turbinate about half inch from the anterior end of the turbinate. After piercing nasoantral wall the trochar entered into antral cavity. The trochar is removed and the cannula is placed properly in the sinus cavity. This procedure is done to irrigate sinus cavity with sterile nasal saline. The discharge comes out through the natural ostium of the sinus. After the procedure local medication is instilled, cannulla is withdrawn and nose is cleaned.
- 38. Intranasal Antrostomy: This is the drainage operation performed on the maxillary sinus to create a permanent window near the floor of antrum to facilitate drainage of discharge. Caldwell –Luc Radical Antrostomy: Incision in the upper gum opening in the anterior wall of antrum removal of the entire diseased maxillary sinus mucosa and drainage is allowed into inferior or middle meatus by creating a large window in the lateral nasal wall.
- 39. Balloon Sinuplasty: This method similar to balloon angioplasty used to unclog arteries of the heart, utilizes balloons in an attempt to expand the openings of the sinuses in a less invasive manner. Functional Endoscopic Sinus Surgery: The normal clearance from the sinus is restored by removing the anatomical and pathological obstructive variations that predispose to sinusitis. The benefit of FESS is its ability to allow for a more targeted approach to the affected sinuses, reducing tissue disruption and minimizing post operative complications.
- 40. NURSING MANAGEMENT: Encourage the client to get plenty of bed rest. Lying down can make sinuses feel more stopped up , so try lying on the side that lets you breathes the best. You can prompt yourself with a pillow. The nurse instructs the patient about the methods to promote drainage such as inhaling steam (steam bath, hot shower), increasing fluid intake and applying local heat.
- 41. Apply moist heat such by holding a warm, wet towel against face or breathing in steam through a cloth or towel. This will relieve sinus pressure and helps to open sinuses. Encourage the patient to avoid bending, lifting heavy objects and stooping.
- 42. Talk with the doctor before using an over the counter cold medicine. Some cold medicines can make symptoms worse or cause other problems. Don’t use a nasal spray with a decongestant in it for more than 3 days. If using it for than 3 days, the swelling in the sinuses may get worse when you stop using the medications.
- 43. PREVENTION: Keep the nose moist as possible with frequent use of nasal saline sprays. Avoid upper respiratory tract infections. Use a humidifier if necessary. If the air in the home is dry such as it is if you have forced hot air heat, adding moisture to the air may help to prevent sinusitis. Be sure the humidifier stays clean and free of mold with regular thorough cleaning. Avoid very dry indoor environments. But be aware that if allergic to molds, house dusts mites, cockroaches; a humid environment may also create problems.
- 44. Avoid exposure to irritants such as cigarette smoking, strong odors from chemicals. Tobacco smoke and air contaminants can irritate and inflame your lungs and nasal passages. Avoid alcohol which can worsen swelling in the sinuses. Avoid long periods of swimming pools treated with chlorine, which irritates the lining of the nose and the sinuses. Avoid water diving which forces water into the sinuses from the nasal passages
- 45. PATIENT EDUCATION: Avoid allergy triggers, antihistamine or nasal corticosteroids Eat fruits & vegetables, Reduces stress, Wash hands and maintain hygiene. Avoid smoke and pollution hydration.
- 46. GUIDELINES FOR REFERRAL: Child with complications or signs of invasive infection. Child needing control of allergic rhinitis. Child with chills and fever. Child with persistent headache. Child with edema of forehead, eyelids. Child with orbital cellulites
- 47. REFERENCES: Lewis's textbook of Medical Surgical Nursing 3 rd edition, Volume- 1 page no: 440-442. Javeed Ansari Textbook of Medical Surgical Nursing PV Books page no: 101- 106. Joycee M Black, Hokanson Hawks Textbook of Medical surgical Nursing Volume 1 &7th Edition Elsevier Publications Page No 1797-1799.