Siliguri Escorts Service Girl ^ 9332606886, WhatsApp Anytime Siliguri
Matua raki-newsletter-september-2014
1. Matua
Raki
News
September 2014 Passion
Commitment
Excellence
Inside:
Youth treatment exemplar services • Living Sober with
Mrs D • Addiction Leadership Day and more...
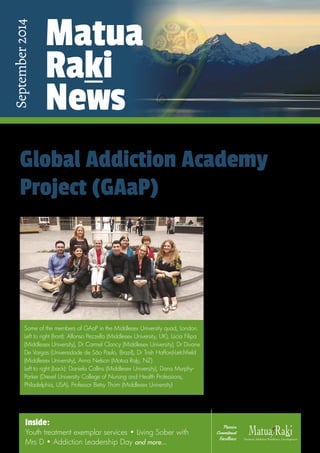
Global Addiction Academy
Project (GAaP)
In 2013 Anna Nelson (programme
lead at Matua Raki) was asked by former
colleagues at Middlesex University to be a
founding member of the Global Addiction
Academy Project (GAaP) to be hosted by
Middlesex University in London. Anna was
funded to go to London by the Middlesex
initiative in May this year to meet with the
rest of the founding members and discuss
the global phenomenon of addiction
and the vision of GAaP. The founding
members come from Middlesex University,
Universidade de São Paulo (Brazil), Drexel
University College of Nursing and Health
Professions, Philadelphia (USA) and Matua
Raki (NZ). They were also joined at the
inaugural meeting by representatives
from Australia (Allan Trifonoff from
the National Centre for Education and
Training on Addiction (NCETA), Flinders
University); Norway (Ian Dawson from
Nordlandssykehuset Hospital, Bodø) and
Albania (Alma Pulma, a mental health
nurse). Continued on page 9.
Some of the members of GAaP in the Middlesex University quad, London.
Left to right (front): Alfonso Pezzella (Middlesex University, UK), Lúcia Filipa
(Middlesex University), Dr Carmel Clancy (Middlesex University), Dr Divane
De Vargas (Universidade de São Paulo, Brazil), Dr Trish Hafford-Letchfield
(Middlesex University), Anna Nelson (Matua Raki, NZ)
Left to right (back): Daniela Collins (Middlesex University), Dana Murphy-
Parker (Drexel University College of Nursing and Health Professions,
Philadelphia, USA), Professor Betsy Thom (Middlesex University)
2. Contents
To download electronic
copies of this newsletter
or any of Matua Raki’s
workforce resources,
visit our website:
matuaraki.org.nz
To inquire about our
resources or request
hard copies, contact us at
matuaraki.org.nz/contact
Matua
Raki
News
September
2014
edition
For more details please contact Patricia Rainey (patricia.rainey@matuaraki.org.nz).
Would you like your event listed here? Go to our website, www.matuaraki.org.nz,
click on the events calendar and complete the Add your event form.
Cover Global Addiction Academy Project (GAaP)
2 Coming events
3 The road ahead…
4 The road travelled…
5 Recent developments
7 Watch this space
8 Getting to know Tanya Cook
9 Youth treatment exemplar services
11 Living Sober with Mrs D
13 Second time around – a profile of Alistair Herring
14 Addiction Leadership Day, 24 July 2014, Auckland
22 A year at the top at CareNZ
24 Fraser Todd at the American Psychiatric Association
25 New Zealand and the International Initiative for Mental Health Leadership
26 A tribute to Paraire Henare Tomoana Huata
Coming Events
8
17
17
18-19
20
TBC
TBC
7
9-12
20
4-5
Dunedin
Dunedin
North Island
Adelaide
Dunedin
Wellington
Christchurch
Auckland; Wellington;
Christchurch
Dunedin
Dunedin
Tauranga
September
October
November
November
December
September
September
September
September
October
November
Substance Withdrawal Management
Meeting of the National Association of Opioid Treatment Providers
Pre-Cutting Edge Hui and Fono
Cutting Edge conference
APSAD
Addiction Nurses Seminar Series
An Introduction to Working with Older People in the Addiction Sector
Older Persons in the Addiction Sector –
Advanced Practice Workshop
Pre-Cutting Edge site visits
Cutting Edge workshops
Addiction Leadership Day
2014
2 Matua Raki News September 2014
3. The road ahead…
Election lobbying is in full swing and now is a good time
to ask questions and listen to the policies and priorities
of our political parties particularly in relation to health and
welfare.
Even if politics has never really been your thing, we all have a role to play in advocating
to get the best for our tangata whaiora and for our committed workforce. Politics and the
political agenda of the day have a large bearing on our sector and those involved in it; how it
is resourced and how it is perceived by the wider community, so having our say is critical to
our success. Regardless of the overall outcome we will be having a new Minister of Health,
so this does give our sector an opportunity to put addiction treatment on his or her agenda
and collectively influence the key priorities for the next couple of years. Here are a couple of
campaigns that are currently underway and I would encourage you to get familiar with these
issues; take part in the debates and advocate where you can.
• www.fairfunding.org.nz aims to re-establish a fair funding system between DHBs
and NGOs
• Equally Well (www.tepou.co.nz/improving-services/physical-health) looks to address
the health inequalities experienced by those with serious mental health and/or
addiction issues
• www.cpag.org.nz working to eliminate child poverty in Aotearoa, New Zealand
• Revision of the New Zealand Drug Policy via the Ministry of Health (which has yet to
be drafted)
Rethinking leadership
We were fortunate at our recent addiction leadership day to have Associate Professor
Trish Hafford-Letchfield, a reader from Middlesex University UK, facilitate a session for us
on Rethinking leadership. She encouraged us all to examine the areas of our practice in which
we have “wilful blindness”. These are areas where we know that things are not right but we
either choose to do nothing or assume that someone else will do something about them. All
the issues noted above are areas where we have tended to be wilfully blind as a sector and I
would encourage each of us to take part in the discussions and support the changes that are
needed. We can all be leaders in our workplaces irrespective of our job titles, as well as in our
communities and our families and whānau – it is up to us to speak for those who don’t have a
strong voice.
Collaboration and coordination for change
One thing is clear, higher levels of collaboration and coordination across all our various
agencies and sectors are necessary to effect the changes required for our country to really
prosper and for all New Zealanders to have the opportunity to succeed. Matua Raki is keen
to see our sector make a collective impact to make a difference in our communities. We
can all see the problems so let’s be part of the solutions. There are some great examples
of collaboration occurring within our sector including the development of a recovery
community website, a partnership between the New Zealand Drug Foundation, Health
Promotion Agency and Matua Raki. This website (www.livingsober.org.nz) has just been
launched and follows the release of the bestselling book Mrs D is Going Without. It aims to
encourage help-seeking and give support to those who would otherwise not access traditional
treatment services. Mrs D received over 30,000 hits and several thousand comments to her
Vanessa Caldwell
national manager,
Matua Raki
Equality means
everyone gets the same
thing; equity means
everyone has the
opportunity to have
the same outcome.”
Passion Commitment Excellence 3
4. It is almost three years since Matua Raki and Te Pou came together as one entity under the Wise Group. It’s been a great journey, but the building blocks for our relationship began in formative years when I was working at the Ministry of Health and managing the workforce development portfolio for mental health and addiction. I had to get to grips with how to develop a national plan (Tauawhitia te Wero, 2006, MOH) and a framework to describe the competencies and skills of our combined workforce (Let’s get real, 2008, MOH).
During this time I learned about the differences between workforce issues in mental health and addiction, but also the challenges we had in common. I met with some amazing leaders, such as Professor Doug Sellman who managed the inaugural workforce programme for the addiction sector at Otago University. He was a champion for an evidence-based approach to workforce development – with a strong emphasis on training. When the programme moved from a University setting to a workforce centre, there were some challenges with ensuring workforce development moved beyond training. Training needs to be coupled with organisational assessment and readiness for practitioners to work differently as a result of the new skills they have learnt: hence our focus on evidence-based workforce planning and being systems- focused. This incorporates organisational development, research and evaluation, infrastructure, recruitment, retention AND training and development. With areas of priority such as workforce planning we are using evidence to describe what we have now, where our gaps might be and where we need to be in the future. This is underpinned by practice and leadership development that ensures we have the right people with the right skills in the right place to deliver services.
I have always thought the addiction sector has been well organised in workforce development – with a workforce that comes from a strong recovery and peer approach, qualifications aligned to dapaanz and a strong focus on evidence- based treatment. It is also quite a tight-knit sector. The addiction leadership days have a good following and there is momentum to continue to build good practice networks. Mental health feels larger, not quite as organised and perhaps more disjointed. So, it has been a bonus to have Matua Raki join us at Te Pou. Vanessa and her team provide great insights into promoting a public health perspective in addiction treatment and workforce development, which has been a struggle in the mental health sector.
During the transition period, we maintained a Matua Raki reference group, chaired by Robert Steenhuisen. The work of this group is now drawing to a close. We have embedded governance arrangements that ensure the work of Matua Raki has a strong mechanism for support and accountability – at the Ministry of
blog following just one interview on TV1 in June – a clear message that there are people keen to engage in an online forum who we have not previously reached. See the full story and interview on
page 11.
A successful transition
Matua Raki has been located within Te Pou for two years now and we continue to find more ways that we can work together to achieve better outcomes. We have been well supported by Robyn Shearer and we have valued highly the ongoing monitoring of the Matua Raki reference group that assisted us in the transition. August brings us to the final meeting of this reference group which has decided to disband as there are several mechanisms in place at all levels of this organisation to ensure that the specific needs of the addiction workforce are being tabled and addressed. I would personally like to thank Robert Steenhuisen, Sheridan Pooley, Lt Col Lynette Hutson, Te Puea Winiata and Ian MacEwan for their support and commitment to the mahi and purpose of Matua Raki.
Cutting Edge conference
The next big event on our calendar is the Cutting Edge conference in Dunedin with a theme of Co-existing problems. Don’t forget the pre-conference events including the hui, open for Māori addiction workers and the fono for Pacific addiction workers, as well as the site trips to local treatment services. I do hope to see many of you there.
Nga mihi
Nā
Vanessa Caldwell
National manager
The road travelled…
Robyn Shearer
chief executive, Te PouMatua Raki News 4 September 2014
5. Mental Health and Addiction Service and workforce
co-existing problems capability - 2014 Integrated Solutions CEP Questionnaires
Tēnā tātou katoa, Talofa lava, Malo e lelei, Kia orana, Bula vinaka, Fakalofa lahi atu and Ni hao.
In 2010, Integrated Solutions was published by the Ministry of Health to inform mental health and addiction services about models of care for people with co-existing mental health and addiction problems (CEP) (www.health.govt.nz/publication/service- delivery-people-co-existing-mental-health-and-addiction-problems- integrated-solutions-2010).
Following this, general managers of mental health and addiction services and planners and funders were asked by the Ministry to provide plans for how their region would develop CEP capable services and workforces. Over the past four years the national workforce programmes have been working with services to support the development of CEP capable services and workforces. Activities have included:
•
knowledge and skills training – e.g. formulation workshops
•
enhanced practitioner train the trainer workshops
•
service checklist workshops – CEP Service Checklist
(www.matuaraki.org.nz/cep-service-checklist)
•
resource development – Te Whare o Tiki
(www.matuaraki.org.nz/te-whare-o-tiki) and CEP in Youth (www.werrycentre.org.nz)
•
national symposium, Wellington – CEP Symposium
(www.matuaraki.org.nz/cep-symposium).
Services across the country have actively worked to improve CEP capability over this period of time through activities such as developing cross service and regional CEP steering groups, initiating regional symposia, supporting workers to be trained as CEP champions and encouraging whole of workforce participation in introductory training.
It is timely to establish an overview of what has been achieved to
date and gather information about what will be needed in the future to support people with CEP.
The Ministry of Health, Matua Raki and Te Pou have developed and distributed online questionnaires that will gather information based on the goals of Integrated Solutions. The questionnaires have been sent to the managers of DHBs and larger NGO services and to DHB planners and funders. The responses to the questionnaires will be collated by Matua Raki and Te Pou for the Ministry of Health. A summary report will be compiled and distributed to the sector.
The information provided by responses to the questionnaires will contribute to the wider evaluation of the workforce programmes’ CEP project. The evaluation will provide a summary of the contribution of the workforce programmes to the development of service and workforce CEP capability. It will also help to identify those areas where there is potential for improvement and as such it will significantly contribute to planning for the workforce programmes’ future CEP service and workforce development activities.
If you have any questions please contact:
Ashley Koning (ashley.koning@matuaraki.org.nz)
Suzette Poole (suzette.poole@tepou.co.nz)
Health/HWNZ with our contracts; with Robert being a member of the Te Pou board; through the clinical reference group which has direct links to me and the Te Pou board (Sheridan Pooley, Fraser Todd, Daryle Deering and Phil Grady are members of this group) and Vanessa being part of the Te Pou senior leadership team. This year there will be a strong focus on CEP being part and parcel of routine practice across both sectors; implementation of ADOM; workforce planning and leadership and practice development.
From my perspective our merger has been a success. Like any relationship we need to work at it and grow. We have that commitment and a strong basis to continue building our programmes together – celebrating our uniqueness and our collaborative strengths. Thank you to the many practitioners and leaders who are engaging with us to ensure we are building the capacity and capability of future services.
Nga mihi nui
Robyn Shearer
Chief executive, Te Pou
Recent developmentsPassion Commitment Excellence 5
6. Guide to the Addiction
Treatment Sector updated
Matua Raki has recently
updated the Guide to the
Addiction Treatment Sector in
Aotearoa New Zealand, which
was originally published
in 2012. Changes in the
guide reflect the changing
landscape of the addiction
treatment sector and the need
for allied workforces to have
current information about
the sector. Changes include
acknowledgement of the impact of DSM5 on the language used
to describe and diagnose addiction disorders, information about
synthetic cannabinoids, updated statistical information and links to
relevant organisations and websites.
The revised Guide to the Addiction Treatment Sector in Aotearoa
New Zealand is available in hard copy from
administrator@matuaraki.org.nz or for download at
www.matuaraki.org.nz.
OST and you: a guide to Opioid
Substitution Treatment
OST and you: A guide to Opioid Substitution Treatment was launched
as a companion document to the Ministry of Health’s NZ Practice
Guidelines for Opioid Substitution Treatment at the National Association
of Opioid Treatment Providers’ meeting in April this year. The
guide was developed by Matua Raki for people who are receiving or
contemplating receiving OST and was written by Sheridan Pooley
and the Matua Raki Consumer Leadership Group.
In less than a month the entire stock of 5,000 copies had been
ordered and distributed
to DHBs, NGOs, needle
exchanges and pharmacies
who deal with people receiving
opioid substitution treatment.
Stocks of a reprint of 2,500
have also been exhausted.
With such large numbers of
the publication in circulation
in targeted areas it is hoped
that they will be accessible to
those who need them.
Physical health risks for people
with mental health and addiction
problems sparks a call to action
We now have a better understanding of why people with
mental health and addiction problems have poor physical health
and what we can do about it. This is thanks to recent research by
the University of Otago, and an evidence review undertaken by
workforce agency Te Pou and Platform Trust, a national network of
non-government mental health and addiction organisations.
Recent research from Dr Ruth Cunningham and her colleagues
at the University of Otago shows that people using mental health
services in New Zealand are two to three times more likely to die
prematurely than the general population, and much of this greater
risk is due to cardiovascular disease and cancers.
The evidence review summarises the drivers of this health
disparity and importantly how to tackle it.
Robyn Shearer, chief executive of Te Pou, says the research
shows health services and related agencies need to work together on
a plan of action.
“We know from the evidence review that there are effective ways
to improve physical health outcomes for people with experience of
mental health and addiction problems. We have to work together
on solutions to known risk factors - particularly the side effects of
medication and access to and quality of health services. All health
services need to acknowledge and prioritise the physical health of
people with experience of mental health and addiction problems.”
A new initiative by Platform Trust and Te Pou called the Equally
Well project, aims to facilitate collective action on this issue (www.
tepou.co.nz/equallywell).
Marion Blake, chief executive of Platform, says the New Zealand
findings support an international trend. “While life expectancy for
most people living in developed countries around the world has
been improving over the last few decades, it has been getting worse
for people with mental health problems and addictions. This is
unacceptable. We must act collectively and we must act now.”
1
OST and you
A guide to Opioid Substitution Treatment
A Guide to the Addiction Treatment Sector
in Aotearoa New Zealand
June 2014
6 Matua Raki News September 2014
7. Takitaki mai - a promise of a new dawn
Takitaki mai: A guide to motivational interviewing for Māori is a new resource to strengthen MI training for Māori. The term ‘takitaki mai’ comes from the phrase ‘Takitaki mai i te ata’ which talks to the harbingers of dawn. MI practitioners have a role to play in picking up and accentuating signs of shift in motivation, potential for transformation. They also have a role in supporting sustained change.
This resource grew out of participation in a Matua Raki MI training opportunity for Māori and Pacific practitioners, the work of Tohi Tohiariki and Daryl Gregory at He Waka Tapu in Christchurch and discussions with Eileen Britt, a member of the MI network of trainers. Matua Raki is pleased to have been a part of bringing this work to fruition and bringing it to print.
MI like other talking therapies sits within a cultural context when working with Māori and so practitioners still need to understand the therapeutic value of integrating MI with pōwhiri processes and practices such as manaaki, whakangahau or karakia.
Takitaki mai was blessed and launched on Thursday 7 August at He Waka Tapu in Christchurch. E-copies will be available on the Matua Raki and He Waka Tapu web sites and copies are available to support MI training.
Ka Pō, Ka Ao, Ka Awatea! Tihei Mauri Ora!
Working with older people in the addiction sector
In response to a growing need in the community and to support those working in the addiction sector, Matua Raki developed a workshop for practitioners interested in knowing more about working with the older people who appear to be accessing addiction services in great numbers. Suzy Morrison has delivered An introduction to working with older people in the addiction sector to 296 participants since April 2012. The workshops continue to be well received by a broad cross-section of the addiction workforce but evaluations indicated that some people wanted a more advanced course.
Dr Helen Warren is in the process of developing an advanced practice workshop on behalf of Matua Raki. This workshop will be delivered in the three main centres before the end of the year. The advanced workshop is intended for experienced practitioners working directly with older persons and their substance use or providing support to those who do.
Helen’s workshop will include:
•
assessing alcohol and drug problems in the older person using principles from the Alcohol-related Problems Survey (ARPS)
•
a screening measure to identify harmful and hazardous drinking in older persons
•
information on drug interactions
•
the cognitive assessment process using the Montreal Cognitive Assessment Test (MoCA).
There will also be a focus on working with the families of those with problematic alcohol and drug use.
Keep your eye on our website and the NZAANDD Mailing List for further information on the advanced practice workshop.
Refugee training
Addiction services in many parts of New Zealand are finding that they are seeing an increasing number of refugees. To be offered protection in New Zealand refugees will have been assessed as having a humanitarian need based on a well-founded fear of prosecution in their countries of origin. For many refugees problems of poverty and social exclusion alongside difficult and traumatic experiences in their countries of origin are profound and make them particularly vulnerable to developing problematic substance use as well as experiencing mental distress.
Matua Raki will work alongside Refugee Trauma Recovery (Wellington) and Refugees as Survivors NZ (Auckland) to develop and deliver training and resources to support the addiction sector to be better equipped to work in a trauma-informed way with refugees who are referred into their services. This training will begin later in the year.
Substance withdrawal management
A series of one-day workshops in substance withdrawal management delivered by Steph Anderson on behalf of Matua Raki were well received in Christchurch, Invercargill and Dunedin in May and June this year. The workshops are intended for nurses and addiction practitioners directly supporting withdrawal management. They are based on the Matua Raki publication Substance Withdrawal Management Guidelines for medical and nursing practitioners in primary health, specialist addiction, custodial and general hospital settings.
The training will be repeated in Whanganui, Hawke’s Bay, Lakes and Northland in October 2014. Final dates and an opportunity to register will be publicised shortly.
Watch this spacePassion Commitment Excellence 7
8. Getting to know Tanya Cook
Tanya is the personal assistant to Matua Raki national manager, Vanessa Caldwell. She also provides administrative support for her Matua Raki colleagues.
How did you come to be working in the addiction sector?
I came to Matua Raki with very little knowledge of the addiction sector. I had been working in Wellington City Council’s Parking Services and needed a change in scenery when the opportunity came up for a position within Matua Raki.
What does your job as a PA/Administrator involve day to day?
It involves a LOT of emails and organisation! My main tasks are helping to maintain Vanessa’s schedule, answering queries from services within our sector, organising travel and arranging meetings and bookings for Vanessa and my Matua Raki team members – and anything else Vanessa or the team deem necessary. Oh and I ensure invoices get paid!
What makes you jump out of bed in the morning, keen to get to work and take on another day?
That would be my manager and wonderful work colleagues and the fantastic work that they strive to do each day! I am very proud to be part of such a strong team with such a wealth of knowledge and experience in the addiction sector. With the passion they bring to work each day it is hard to not be motivated.
How do you think you’re making a difference?
My role is pretty minor in comparison to the work my colleagues do so I’m not really sure. I think what I do allows the team to focus more on their particular projects and that’s probably a good thing.
Tell us about your family situation.
I am a single parent, raising my wonderful, if not sometimes testing, 10-year-old son Tremaine. I have a certificate in Make-up Artistry, but I’ve not been able to pursue this as a career mainly due to availability and resources. In saying that, I am constantly kept busy with friends’ weddings and other social events. I have previously worked with the World of Wearable Arts and was also given the opportunity to work on the set of the Kiwi short film Good for Nothing.
When you’re not saving the world, what else do you like to do?
I love to attend concerts and theatre shows. New Zealand has such a large range of talent and, with large international acts constantly visiting our shores, it’s not hard to be spoilt for choice whether it’s watching a street performance with my son or a Fat Freddy’s concert with friends. I constantly find myself pleasantly lost in a world of creativity, imagination and inspiration.
What’s the most awesome film you’ve seen, and why?
I love the film Remember the Titans. It has a great soundtrack with loads of classics and also carries a deeper message, one where you have characters that are not afraid to push the boundaries and challenge society in their thoughts and acceptances. It’s a film based on a true story set in the 70s which explores topics such as racism and discrimination within a school football team. I loved it because it really shows how a few people, and in many cases just one person, can influence a community and bring unity where it was once thought not possible.
Tanya CookMatua Raki News 8 September 2014
9. Global Addiction Academy Project (continued from page 1)
GAaP members presented information on their organisations and about alcohol and drug use and addiction treatment in their respective countries. This provided a platform for the group to discuss the vision of GAaP and some steps for future work together. During the GAaP meeting a seminar and discussion session was also held at Middlesex University for Drug and Alcohol Research Centre (DARC) members, staff and students. Each of the GAaP members offered a ‘State of the Nation’ presentation at the seminar session which clearly articulated the differences between countries.
Some of the most memorable moments from these presentations included Dr Divane De Vargas reporting that Brazil (a country of 198 million people) had less than 400 state-funded outpatient addiction services; Alma Palma from Albania describing how patients share beds in detox facilities and Dana Murphy- Parker suggesting that due to new legislation in the USA (Patient Protection and Affordable Care Act, known as Obama Care, and the Mental Health Parity and Addiction Equity Act) there is likely to be 11 million more people eligible for and requiring services for serious mental illness, psychological distress and/or a substance use disorder, and they are clearly concerned that they do not have the workforce required to meet this need. Comparatively it seems New Zealand is very well served by the range of treatment options available and the existence of an addiction workforce development centre. Many of the GAaP and DARC members and staff were very interested in the idea of ‘workforce development’ and the role of Matua Raki, as this appears to be something they feel is missing in the international context.
A memorandum of international partnership to shape the vision and expectations of GAaP members moving forward was also drafted.
Over the course of the week it was agreed that the GAaP strap line would be:
Addiction is a global phenomenon requiring global solutions from a global community
GAaP’s vision is to:
•
raise the profile of addiction internationally as a health and social care issue
•
provide an online knowledge hub and best practice platform
•
provide a global online classroom
•
bring addiction policy, clinical, education and academia together
•
raise the profile of addiction issues in other areas of health and social care education.
It was agreed that GAaP would focus on five main areas and consider these issues internationally:
•
practice
•
education
•
research
•
workforce
•
lived experience.
Some initial projects were discussed and it was agreed that within the first year GAaP would produce:
•
a global addiction workforce report to be presented to the UN General Assembly in 2016 which has a focus on a global position on drug policy and addiction
•
a scoping paper that investigates other international addiction projects, their roles and responsibilities.
Anna has begun drafting the global addiction workforce paper which will form the basis of the report produced for the UN in 2016.
According to the Ministry of Health, having youth-focused services that are able to deal with mental health, alcohol and drug issues makes it easier for young people to get help if they need it and reduces a huge barrier for young people reluctant to engage with health services.
Unfortunately, the Ministry acknowledges, our youth AOD services have tended to develop in inconsistent, ad hoc ways and without a collective strategic direction.
The Prime Minister’s Youth Mental Health and Addiction programme includes the initiative ‘Improving access to youth AOD services’ which involves establishing and evaluating new ‘exemplar’ services according to a model of good practice.
Being an exemplar service is not about being elite. It’s about providing an excellent service that meets a number of essential pre- defined ‘design features’; can demonstrate results and serve as a role model for others.
Youth treatment exemplar servicesPassion Commitment Excellence 9
10. These ‘design features’ include flexible hours and mobility, inclusion of families/whānau, co-ordinated care across services, appropriate responsiveness, co-existing problem (CEP) capability, evidence-based interventions and cultural responsiveness.
Initially six sites were considered, all of which received funding towards progressing improved youth treatment services, but two were selected to become exemplars and receive ongoing funding.
Mirror Services
Dunedin-based Mirror Services’ exemplar programme started in March 2014 with around 30 young people transitioned from existing services provided by Mirror. It receives between 15 and 20 new referrals each month.
The service is available for 12 - 22-year-olds who can self-refer or be referred by a professional. The aim is to see young people promptly and focus on engagement. Staff are youth-focused and deliver age and developmentally appropriate interventions. It is a mobile service, so young people and their whānau can be seen in a setting that is suitable to them.
The urban centre has been set up in Dunedin and a network of services will be established across rural areas where required. The service comprises a multidisciplinary team so all aspects are well-covered from case management, psychiatric and psychological input to whānau therapy and peer support. All staff are CEP capable and qualified in addiction and mental health. Ongoing professional development ensures up-to-date knowledge is integrated in terms of being culturally responsive and youth and CEP-focused.
To make the service family/whānau inclusive, a family therapist has been appointed to work alongside other clinicians. This is to help whānau support their young person to maintain changes.
“It’s an important area to address,” says Mirror Services director, Deb Fraser.
“On the one hand, the family could have significant challenges with supporting change for their child because they also have a substance use issue. On the other hand, the family could be in a position to be part of the solution. If there’s an expectation a young person will change, there needs to be a commitment from other family members who might also need to change, and we work to assist with that.”
Deb says young people experience many barriers to entering and engaging with services so they’ve been working with other services to improve access and ongoing support.
One of the service’s key components is that it is mobile. If there are good reasons why the person needs to be seen somewhere else, and when safety issues have been considered, the team will travel around the greater Dunedin area. Opening times are flexible and staff are happy to see people outside work hours.
“It’s important not to make things hard for people,” Deb says. “It is imperative we address any organisational barriers that prevent people being seen.”
Deb says the response has been over and above expectations.
“We thought it would take a while to get established and to get people accessing the service. But despite very little promotion, people have been able to access us quickly. Referrals have come through faster than we thought, and we’ve even had young people just walking in. This is exactly what we want.”
The service is doing its own internal review and reports and will be evaluated by the Ministry of Health when it has been running for 12 months.
Rubicon Youth Alcohol and Drug Support Services
Whangarei-based Rubicon also began development of its exemplar programme in March this year with a service targeting 11-19-year-olds. They run flexible hours and young people can self-refer or they can be referred through their school or local community agencies. Rubicon runs a youth activity programme and a number of young people have come in through that as well.
The service is based on a ‘hub and spoke’ model. The urban (hub) aspect is centred in the Whangarei and Kaipara districts, with the rural (spoke) aspect focused in the Kaitaia and Far North districts.
“We’re very much about being an outreach and mobile service, so even our specialist and psychologist positions are mobile,” says director Jenny Rooney-Gibbs.
“That’s unique in terms of our service, and it’s a key area that’s working really well; meeting youth and/or their whānau in their schools, homes or wherever is appropriate, thus reducing barriers to access and reaching those who have traditionally been marginalised and left out.”
Jenny’s excited about the exemplar programme and looks forward to sharing the model with others.
“We’re developing a template and, when we’re up and running, other services will be able to come to us and ask how to do this work and what they need to do to deliver a similar service in their community. We can support them to develop what they do. The
Mirror team from left: Deb Fraser (director), Tanya Phillips (CEP practitioner), Pene Muir (clinical psychologist), Lisa Perniskie (peer support worker) and Tangi Noomotu (clinical team leader) Matua Raki News 10 September 2014
11. Living Sober with Mrs D
Lotta Dann, the journalist wife of TVNZ political editor Corin Dann and a mother of three, has outed herself as an alcoholic in recovery and released a book, Mrs D is Going Without, which has quickly become a bestseller.
Dann started writing an anonymous blog about her battle with booze nearly three years ago and now it receives about 2,500 hits a day from others who are sharing their own journey. Dann will reach an even wider audience as the face of a new website (www. livingsober.org.nz) launched in August by the New Zealand Drug Foundation, Matua Raki and the Health Promotion Agency. As well as featuring Dann’s blog, the website offers resources and an interactive online community for people who are looking for support to stop drinking. Lotta supports nearly 500 people who joined this group in its first week of going live. In a shared interview with NZ Drug Foundation, Lotta spoke about her transformation from a “boozy housewife” to a model of happy sobriety.
You have been interviewed on television and in radio interviews since going public and the release of your book, how much impact do you think your story has had?
I’m hoping that the impact has been huge where it counts which is with the people who are like me, and from what I can tell it has been, because I’ve just been inundated with emails and private Facebook messages and they’re all saying, ‘I’m just like you, it used to be just a glass of wine at night and now it’s a bottle, I’m holding down my life but I’m feeling really guilty’. A lot of them are businesswomen, successful people, who are privately battling this addiction and they’ve had no outlet for it, and then I pop up and they’ve gone, ‘Oh my God’.”
The night the Sunday interview aired on TV1 I had 30,000 hits on my blog, it was unbelievable. I remember the overwhelming feeling that I had three years ago was loneliness, and I was married and had a lot of friends, but battling an addiction that isn’t visible is a very tricky, internal place to be so you really do feel quite alone. I wanted to reach out to the people who feel that way too so they know they’re not alone.
How bad did your drinking get and how was it affecting your family life?
It started to really bed in and become much more habitual when I was at home alone with the kids and dealing with the Groundhog Day aspect of that. I don’t think they were suffering from my drinking yet, I got out before I hit a real rock bottom. I would’ve been a bit vacant and full of wine in the evenings, probably a sore head and dragging my hungover body around during the day. But Corin and I didn’t have fights, it wasn’t a drama drinking problem, it was just a sad, heavy, sloppy, personal drinking problem.
How important was it for you to accept the label of being an ‘alcoholic’ with all of the connotations and stigma that comes with that word?
I have sober friends who still haven’t accepted that label. But for me, when I had that thought that I was an alcoholic, it was very
plan is to make ourselves as accessible as possible to others following in our footsteps.”
She says another way the exemplar service is unique is in how it works with families. When a young person enters the mental health service it’s usually family first and then the young person. The exemplar service puts the young person first.
“That way you’ve already got the relationship and trust with the young person, and then you bring in the whānau for more support.”
The service has made tremendous progress linking with other services, especially in Whangarei. In particular they have two registered nurses in each area who are essential in improving links with primary care. In the Far North they are consulting with Iwi to find out what their communities need.
The majority of Rubicon staff are CEP-trained and two are currently training via the Werry Centre’s train-the-trainer programme. Those that still need to be up-skilled have had training programmes established and the aim is to have all staff fully CEP capable.
There hasn’t yet been any official evaluation, but criteria have been set and data is being collected so internal evaluation can occur. Jenny says this is likely to happen in about three months and, of course, the Ministry of Health will officially evaluate the programme after 12 months of operation.
Rubicon Youth director, Jenny Rooney-GibbsPassion Commitment Excellence 11
12. calming, because it was a complete acceptance of the fact that I can’t touch alcohol ever again. It was lovely actually, because it was simpler. It simplified everything and I realised that the combination of my brain and alcohol doesn’t work; I just can’t moderate with that drug.
How important to your recovery was your blog and the online community that developed around it?
My main technique was writing out my thoughts and feelings, you could do that privately and it would still be effective, but because I did it publicly through blogging I was led to my second great sobriety tool - the online recovery community. I didn’t go to any counselling or groups.
My advice to other people who want to stop drinking is, don’t hide from the truth, believe that change is possible, find your like- minded community who can help you, and know that you can get to a place where you are free from all the angsting and cravings. It is hard, but you can get to a place where you don’t miss it. You have to be very strong and determined for the first six months to a year, but after 12 months you start feeling much freer. The new Living Sober website is great because we can all climb in there together and help each other.
Was it a tough decision to publicly admit your drinking problem when your husband has a high-profile career?
I talked to Corin about it, it was a big decision but he was 100 per cent behind me. He would tell you that there was no stopping me, not that he wanted to. He really encouraged me to write my story. We just feel that it’s so real and important and it’s something that matters. I feel so good being sober that I want other people who feel trapped in a boozy hole to know you can get out of it. You do get a bit evangelical about it I think.
How good do you feel now, nearly three years into your recovery, and how certain are you that you’ll never drink again?
It’s so great when you realise fun is fun just if you’re having fun; it’s not about what you’re drinking. I’m figuring out how to deal with the hard things of being a human without pushing them away with alcohol. I love it, it’s amazing being open to this whole world of emotional experiences. I used to wake up at 3am and go to the bathroom and I’d feel nauseous and guilty. That 3am guilt has gone. I slept like crap when I was boozing but I sleep great now, I often wake up and go, “Wow, another night of eight hours sleep!”
I’ve retrained my brain, I don’t need alcohol in my life and I don’t miss it. Even thinking that at my sons’ weddings in 20 years or 30 years’ time I’ll be toasting them with a glass of orange juice in my hand doesn’t bother me, in fact I’m really happy about that.
Lotta Dann
“You people are amazing. I couldn’t even get through one week sober. Am living a life of shame, fear, hangovers and misery. Reading your comments inspires me to try, try, try again. Big thanks for this site.”
“When I tried getting sober before I didn’t change my life style at all and just hung around pubs to keep the peace and go along with everyone else. We need to support each other and the great thing is we have Living Sober which is so helpful to me, stay strong and good luck. xx”
“Hi thank you, Living Sober is a great site. I’ve done AA meetings and they are good I just could never share like I do on here. Need to get to the root of the problem though and I will just need to keep focused and remind myself to check me every day, and not let that bloody voice creep in.
Have great day. xx” Matua Raki News 12 September 2014
13. Second time around – a profile of Alistair Herring
In May 2014 Alistair Herring was appointed to the role of national director of Addictions and Supportive Accommodation Services within The Salvation Army.
The position gives him responsibility for all The Salvation Army’s Bridge AOD and Oasis Gambling programmes along with its Supportive Accommodation and Reintegration Services.
The addiction services include 15 centres across the country and involve 148 full-time and 138 part-time staff. Eleven full-time staff
and 11 part-time staff work in the gambling harm services. In the July 2013 to June 2014 year there were 6,141 AOD service users and 2,700 gambling harm service users.
The Supportive Accommodation service, which offers accommodation and wrap-around services to homeless people with multi-faceted issues including mental health issues, involves two large residential facilities in Auckland and Christchurch with 40 staff. Lastly, the Prisoner Reintegration Service, which supports high-risk people coming out of prison to successfully reintegrate into the community and avoid reoffending, has four centres in Wellington, Hawke’s Bay, Christchurch and Southland and 14 staff.
Each of these four services has an operations manager working under Alistair and there are 14 full or part-time staff altogether in the national office in Auckland.
Alistair has been in The Salvation Army for most of his working life, after joining in his mid-20s. Prior to this he worked in the prison service, which he says gave him an interest in social work and an insight into the areas of disadvantage and dysfunction that many people struggle with, often from a young age.
He says he feels a bit like he’s been “recycled”, having held the same position in 2000 for three years. After that he worked in three different parts of the world which he regards as an enriching and privileged opportunity.
“In 2006 my wife and I went to Russia for five years, which was an amazing experience involving many challenges. While there I also worked across four other Eastern-European countries (Georgia, Ukraine, Moldova and Romania), all of which still had significant societal and economic issues left over from the Soviet era. This was a challenge both for the people living there and for The Salvation Army.
“We found the people to be very resilient, despite the widespread poverty present in their communities, and very open to establishing new services. Addiction was spread across the board, but was mainly manifested in alcohol, especially among the homeless – of whom there are still plenty. Addiction to other drugs is rarely acknowledged and is seen as an embarrassment, but for some reason there had been no real societal acceptance of alcohol and drug addiction as an issue requiring serious attention.”
Due to a lack of funding, Alistair said The Salvation Army’s services in Eastern Europe were mostly implemented in an informal manner. Their programmes tended to be community-based and were usually driven out of existing services for the homeless. They were able to train a number of staff from the community and local churches in motivational interviewing techniques and one-on- one services. They managed to get a little funding and formal recognition for one service in the Russian port city of Rostov-on- Don in partnership with a local hospital and by collaborating with the Orthodox Church.
After five years in Russia, Alistair spent two years based at The Salvation Army’s international headquarters in the UK, where he was responsible for working with The Salvation Army in 18 countries in the South Pacific and Asia. He then moved to Pakistan for a year.
“Pakistan was inspiring. The Christian church has actually been there for centuries and The Salvation Army has been there for 130 years – so it’s fairly well-respected. We have staff at 130 centres throughout the
Salvation Army school in Pakistan
Alistair Herring and his wife AstridPassion Commitment Excellence 13
14. Addiction Leadership Day,
24 July 2014, Auckland
To support existing and emerging leaders and managers, Matua Raki, in collaboration with the National Committee for Addiction Treatment, holds three Addiction Leadership Days each year. The most recent was held on 24 July 2014 in Auckland where we were, once again, kindly hosted by The Salvation Army Addiction Services.
Leadership revisited
Dr Trish Hafford-Letchfield is an Associate Professor in Social Work and a Senior Teaching Fellow and programme leader of an Inter-professional Leadership Programme at Middlesex University in London.
She has a nurse’s background, but has more than 10 years management experience and is widely published on issues relating to management and organisational development. One of her most recent publications is a book written with New Zealander Christine Cocker titled Rethinking anti-discriminatory and anti-oppressive theories for social work practice.
Her Professional Leadership Programme in the UK is aimed at nurses, social workers and mental health practitioners. Most are not in management positions but the programme encourages them to take up a leadership role without necessarily being in a leadership capacity.
“Leadership is a topic everyone talks about, because it’s so important; it’s the most needed thing for transforming and improving services.”
Trish said that leadership is a political activity and she explored some of the rhetoric surrounding the concept. One of the political concepts associated with leadership which merits consideration is that of wilful blindness where people deliberately don’t put
country and these often collaborate with local authorities and other churches. They are very good at operating from a community development model.
“We’re also widely accepted by Muslims and there’s significant collaboration and shared respect between Christianity and Islam, although that’s never been recognised by the media, who prefer to dwell only on bad news.
“There are still instances of persecution, but they come from a small extremist element, which is not seen as acceptable to most Muslims there, and we frequently had evidence of that.”
Alistair says there are three main things he’s most looking forward to accomplishing in his role the second time round.
“Last time I was in this position we put together a model of treatment for our AOD services, which was launched by my successor Lynette Hutson in 2004. Since returning to the country I’ve learned there’s been a decision to review that model with a view to updating it and ensuring it still meets the needs of the community.
“In updating it we’ll be involving the same team who helped develop the original model, as well as re-engaging some of the same advisors across the AOD sector to assist in the process.”
The second is a significant piece of research being conducted in collaboration with Otago University, which was started last year, evaluating the effectiveness of the AOD services The Salvation Army offers throughout the country.
“When we established the model of treatment for our AOD services, we built in the requirement that it needed to be evidence- based. Much of the research has been done with current and former service users across the country, and we’ll be looking to publish the results in the next year or two as the data is analysed. This will give us a better look at the quality of the services we provide, and assist us in the review of our model of treatment.
“I am also looking forward to the continuing development of our gambling harm services having been there at the beginning in the late 90s when I was at the Auckland Bridge Centre.”
Mobile Clinic in MoldoviaMatua Raki News 14 September 2014
15. themselves in a position that would make it obvious something is wrong.
“Wilful blindness is difficult to talk about and consider, because it’s something we’ve all experienced. In our day-to-day actions we see things that aren’t working or could be improved and yet we choose not to talk about them.”
She put it to the audience to come up with their own example of a case of wilful blindness and one member suggested New Zealand’s current efforts to improve legislation around the sale and consumption of alcohol.
“The Government is deliberately ignoring the data that they have collected themselves and so are missing the opportunity to create effective legislation that would bring about less harm from alcohol.”
She said it was unfortunate that wilful blindness has become a part of culture everywhere.
“Everybody knows we should be working in ways that are more integrated – so why is it we’re working in silence and no one is speaking up and being a leader? What are the forces at work that make us deny the issues staring us in the face?
“One barrier is risk. Being a leader means making decisions, which involves taking risks. One way to beat this barrier is for leadership to be distributed throughout an organisation, or between organisations in partnership, while still being owned on an individual level. Leadership needs to be able to be questioned, either from above or below, and a culture of open and critical dialogue needs to be nurtured.”
Trish described in detail four different models of leadership. The first model, transactional leadership, relies heavily on predictability, and doesn’t cope well with change. A transactional leader motivates work by distributing rewards and sanctions, and strongly adheres to planning and schedules.
The second model is the transformational leader, who looks to inspire change and innovation, and deals mainly with abstract and intangible concepts. The third is the charismatic leader, who creates impetus for change and motivates others well. These leaders generally have a grand and idealised vision, and their enthusiasm unites people towards that vision.
The final model is distributed or participatory leadership, which sees leadership being shared throughout an organisation. This leadership is represented by a common culture of team-work and collaboration, and is not associated with a formal position or role.
Each type of leadership has its strengths and weaknesses and is more or less helpful depending on the situation.
One audience member described their experience of participatory leadership shared between organisations in a partnership. He said a number of large Auckland-based organisations had come together to pilot drug courts. Within their shared leadership there had been moments of tension, but by viewing it as positive tension they were able to move forward in a healthy direction.
Trish said working in this co-productive model meant understanding that your organisation has needs, but also has significant contributions to make, including its resources and networks.
“It’s also necessary to have a degree of emotional intelligence, a concept that relates to being able to recognise your own emotions and the emotions of others and tailoring your responses in an appropriate way. This is very important when managing change between organisations because it prevents people from shutting down or becoming defensive when discussing change.”
Towards the end of her presentation, Trish invited the audience to divide into groups and discuss the different models of leadership and the skills and support they’d need to achieve a more participatory and distributed model of leadership.
After the discussions Robert Steenhuisen (CADS Auckland) outlined how his group had discussed the importance of framing the debate.
“We looked at the relationship between a manager and staff, and discussed the importance of framing the debate wide enough so that everyone in the partnership can grow. Many of our staff come to managers and clinical leaders to fix problems, which generally involves money. We need to be able to have mature conversations about how services are organised and what it costs to deliver the interventions.
“The reality is we need to make choices about what we will do and what we can’t do for now. Staff and leaders are equal partners and must be able to see each other’s perspective. It is not the role of leaders to micro-manage staff, nor can staff expect that everything they ask for is financially possible.”
Alastair Herring, Salvation Army national director of Addictions and Supportive Accommodation spoke about the importance of trust when sharing leadership between organisations.
“We talked about the generosity of trust, which isn’t tangible, but is still so powerful. Trust means risk, and distributed and co- productive models of leadership require a lot of trust.
“At the Salvation Army we’ve worked with a wide range of organisations, even the Mongrel Mob. And I remember sitting with some of the Mob leaders, and feeling astounded at how trusting they were, to allow another organisation to work in partnership with them and their whānau.
“I’ve recently been working in Pakistan, and what the world doesn’t know is that Muslims and Christians over there work together – they trust each other. The best examples of this were seen in the villages where, faced with a common need, they came
Dr Trish Hafford- LetchfieldPassion Commitment Excellence 15
16. together and both sides took leadership. Against incredible odds, using generosity and trust, they achieved some amazing things.”
Trish concluded by asking the audience how we are going to know that we’ve developed strong leadership. Some suggested it would be a sense of community connectedness. Others said we’d know when people recognised problems, came forward and developed solutions and felt they were able to talk and contribute without being dismissed.
In her final words, Trish outlined some of the traits of a good leader.
“Good leaders take responsibility for the impact of their decisions on others. They recognise the invaluable asset of common humanity throughout the service system and build spaces in which productive relationships can flourish. And they transform cultures and dismantle structures that concentrate power within rigid hierarchies.”
Employment support and addiction: what works
After morning tea Anna Nelson from Matua Raki introduced a paper (produced by Matua Raki and the Centre for Mental Health in the UK) on individual placement and support (IPS), which seeks to integrate people with addiction issues into the workforce.
“IPS is about offering people employment wherever they are in their journey, regardless of whether they’re still using drugs and alcohol,” Anna said.
“It’s an established and proven approach to supported employment in mental health services, and one of the key factors is that it is offered alongside clinical treatment – not afterwards. It’s also seen as an intervention in itself, intentionally addressing barriers to employment.”
Anna broke IPS down into its eight key principles, which stipulate how the process is to be approached and carried out. To start, the primary goal is competitive employment, and it should be available to anyone who wants it. There shouldn’t be any rules or regulations about who can and can’t be offered employment support, and you don’t need to be drug-free to participate.
Other principles included the job search being in line with individual preferences and strengths, and that the process should be started within four weeks to increase chances of success.
“It’s important that employment specialists and clinical teams work and are located together, and that there is unlimited and individualised support to both the employee and the employer. Welfare benefit advice and information is available and offered during the process, and relationships should be formed with local employers to uncover the hidden job market, and increase chances of success.
“We learned a number of lessons throughout the process, including the need for a vocational champion in service. It was also important that practitioners work on addiction-related issues as part of job seeking and return to work process. We needed to be proactively supporting people to prevent missed appointments, and making use of community-based services to help people wherever we could. We also needed someone to be managing the administrative details, such as organising the criminal record checks and picking up medications.”
Warren Elwin (CEO, Workwise)
Warren Elwin gave a brief overview of the services Workwise offers, and reinforced the need for employment support in treating people with drug and alcohol issues.
“Workwise has been delivering employment solutions since 1999, and we work with all sorts of people to return and stay in work, whether they have personal or health challenges, a history of offending or co-existing problems, including substance dependence,” he said.
“Over the past five years our programmes have enabled more than 5,000 people to improve their employment prospects, and more than 3,000 of them have secured employment, many of whom had addiction issues. Last year alone we helped secure 900 jobs and 150 higher-education outcomes.”
He said Workwise was committed to applying the best available evidence to its practice, and that evidence is now so well The idea that someone with mental health or addiction issues has to be better before they’re able to enter the workforce is still prevalent, but we’re here to say that’s nonsense.”
Warren Elwin
Anna NelsonMatua Raki News 16 September 2014
17. documented, that it’s unethical to provide any service unless it fundamentally adheres to the evidence base.
“The idea that someone with mental health or addiction issues has to be better before they’re able to enter the workforce is still prevalent, but we’re here to say that’s nonsense. The evidence clearly shows that the further forward we can implement employment support in someone’s recovery journey, the better. This approach needs to be routinely available in our health services.”
Sandie Finnigan (CareNZ)
Sandie Finnigan spoke about what’s working well for CareNZ in terms of providing an integrated service. She also shared some of the challenges they’re facing and a few examples of the differences they’re making.
“We’re lucky enough to share a building with the other services we work with, and have made a real effort to build strong relationships with these services. We all want to work together seamlessly and prevent any barriers coming between us.
“One way we’re achieving this is by using a shared health record system, which is a wonderful way of sharing notes and recovery plans as it means there’s only ever one version of notes that we’re all contributing to. This helps to eliminate the duplicating of records, and creates a more holistic picture.
“Another benefit is the informal method of communicating we use between services. When we have something to share with another organisation, rather than organising a meeting, we just approach them and address the issue immediately, so no details get lost in translation.”
Sandie said this also benefits the service user. They only have to tell their story to one service, which is then shared with the other services who are able to add layers to the story as more information comes to light. It also means support is there from both employment and addiction services. So if they get a call from an employer saying he thinks the employee is using again, they have all the services at hand to deal with the situation.
“Our goal is to show that reintegration back into the working community and normal life isn’t a sink or swim thing – but is genuinely supported.”
But Sandie said there are still challenges that can make the process difficult, especially the mind-set that the service user needs to have recovered from their drug and alcohol issues before they can be introduced back into the workforce.
To illustrate their success, Sandie gave the example of Bob, a 52 year-old alcoholic who had lost multiple jobs because of his drinking. Bob came to CareNZ and was put through the withdrawal management process at a treatment centre, but relapsed after being released. He returned again, went through the same process, but continued to relapse. And that’s when the team began thinking about what they could do differently.
“We engaged Workwise and got him a job. Unfortunately he relapsed again, drove drunk and lost his license for 18 months. However, because of the support from CareNZ, Workwise and his WINZ work broker, he didn’t lose his job. He now realises how important that job is to him, and it’s become his motivation to get his life back on track.”
Cassie Isaacs and Clair Cummings
(Odyssey House)
Cassie Isaacs and Clair Cummings are part of the Employment Services team at Odyssey House, a community-based organisation providing employment opportunities to people with mental health and CEP. They also offer youth and school programmes.
“Our employment service is designed to start working with clients at a very early stage of their treatment, and we view our employment service as an integral part of their recovery, and not just an additional service,” Cassie said.
“Our key is to establish goals we can focus on and work towards – and to set these goals we use a range of assessment tools to analyse service users’ education and work history, to identify their skills, and to decide on a career choice that works well for them.
“Once we’ve established the career they want to work towards, we create an employment plan, which sets out how we intend to secure them a job. We also help them write a CV, and meet with them weekly to discuss ways to look for jobs or write cover letters. We even offer interview techniques.”
Cassie and Clair discussed a couple of case studies that highlighted the benefit of their service. The first example was Marie,
Sandie Finnigan Our goal is to show that reintegration back into the working community and normal life isn’t a sink or swim thing.”
Cassie Isaacs and Clair CummingsPassion Commitment Excellence 17
18. who had a varied work history, and was looking to land a job in IT. Using their career assessment tools, they were able to show that a career in IT wasn’t suited to her, and would have resulted in low job satisfaction.
Another example was that of Daniel, a 20 year-old with low self-esteem who had spent time in prison. He wasn’t hopeful of his chances of getting a job, so the team wrote an employment plan and a CV and helped him prepare for interviews, and he landed a work trial doing something he enjoyed.
“The best part of this is that he couldn’t believe it. He’s beaming at landing a job, and goes back into the community talking about it, where others hear his story and wonder if the service will work for them too,” Clair said.
Youth initiatives
The first session after lunch involved presentations from various speakers about what they are doing with rangatahi/youth. The session was opened by Peter Kennerley (Ministry of Health) and Grant O’Brien (Mental Health Commission).
Peter said issues around addiction and mental health for young people have been a focus of the Ministry and other government agencies for some time. Some of the initiatives resulting from this include the exemplar services and improving the transition plan from primary care to secondary services.
He acknowledged the work done by the Werry Centre in developing the Youth Transition Guidelines, and said that from 1 July, all DHB-funded services will be required to report on those plans.
Peter also said the connection between what happens at the central government agency level and frontline services cannot be one way.
“We need to hear about the innovations and ideas of frontline services so we can expand and acknowledge those services across the country.”
Grant spoke about two documents that have relevance to the work we do with young people.
According to the Global Status Report on Alcohol and Health (January 2014) – around the world alcohol is directly responsible for 3.3 million deaths and is a direct cause of around 200 diseases, including metal health problems and addiction. This brings home the importance of the work we do with young people.
“People over the age of 15 consume an average of 6.4 litres of pure alcohol per year. In New Zealand the average is 10.4 litres. So the amount of harm it does in our society is massive,” he said.
He also spoke about the Health Promotion Agency’s June issue of Alcohol in New Zealand. He read from a section ‘Young adults and risky drinking.’
“‘People don’t just get drunk in NZ; they get wasted, totalled, munted and even falling down drunk’. This is the opening statement about what alcohol means to our young people, and this will have implications for everything we do.”
Grant commended the services out there working where things are not always easy.
“It takes a long time to create sustained change and that’s why it’s important to focus on youth and concentrate on the front end of the continuum of care.”
Rubicon Youth Alcohol and Drug Support Services
Rubicon director, Jenny Rooney-Gibbs said the organisation has being doing a lot of work around its exemplar service, which has taken on many of the young people who weren’t getting through their normal programme, mainly due to CEP issues. When these young people had been referred to the local Child and Adolescent Mental Health Service, they often didn’t meet the threshold for
Grant O’Brien It takes a long time to create sustained change and that’s why it’s important to focus on youth and concentrate on the front end of the continuum of care.”
Jenny Rooney- Gibbs
Peter KennerleyMatua Raki News 18 September 2014
19. treatment, so a lot of them were under the radar for mental health issues.
She went on to explain some of the differences with the exemplar service.
“We’ve done some research on what wasn’t working for our young people and out of that has come a real focus on meeting young people’s physical health needs. Our registered nurses, for example, work closely with Police Youth Aid when a young person first presents with AOD or other issues. They have a needs assessment done and we look at getting them the physical care they need including their dental, sexual and behavioural health needs.”
The service works with up to 400 young people at any one time and Jenny said its point of difference is that it is highly mobile.
“And one thing we pride ourselves on is our having no waiting lists, which is one of the criteria for exemplar services. We’re very good at making sure there’s always someone there to see a young person in need.
“We run activity-based programmes, such as our after-school programme which is particularly good for young people with AOD and other problems. So our community support workers will pick them up after school and teach them basic life skills, like how to cook, etc. So we’re looking at their other needs beyond their alcohol and drug issues.”
She said their Whangarei service took its first CEP referrals in April, but that the Kaitaia and Far North CEP service was still a work in progress
“One of the things we’re working on there is building relationships and pathways with the community and that’s going very well. Community organisations have been really welcoming of us.”
You can read more about Rubicon and exemplar services in general on page 10.
Youth AOD primary care liaison
Grant Christie (CADS Youth Service, Waitemata Health) reported on his team’s work developing a new youth AOD primary care liaison service.
He said young people experience poor access to primary care health services and that strategies used to improve this poor access include making health care services more attractive by having young people involved in designing services, removing cost and being mobile – “going to where they are instead of making them come to us”.
He said AOD problems are a central determinant of youth health outcomes and that we need to take every opportunity to offer assessment and treatment, particularly in primary care. Responses to any presentation must be prompt, youth appropriate and effective.
“We’re doing this because if we can start addressing problems early at the primary care end (seeing the school nurse or their GP or a CYFS social worker) and provide a positive experience the first time they access primary care, they’ll be much more likely to seek help from services again later on if they need them.”
Strategies to achieve this include brief intervention training to equip primary care agencies with tools to identify AOD problems. Another way is improving liaison and consultation between primary care and treatment services to develop better pathways for referrals to youth AOD services.
“A lot of the work of the primary care liaison team will be with primary care providers, giving them advice, showing how to do a brief intervention and supporting them to provide AOD interventions to young people. A key factor will be providing access to direct feedback from CADS clinicians so they can check that they’re doing okay. If primary care providers feel supported in their work and know where they can go to for help if they feel out of their comfort zone, then they’ll be more confident about taking on this kind of work.”
The primary care liaison service is fully integrated within CADS’ Altered High Youth Service and is supported by Waitemata DHB’s Child and Adolescent Mental Health Service. It will consist of three senior AOD clinicians who will each have a focus on one of the three Auckland DHBs.
Hikaka te manawa: Making a difference for rangatahi
Ana Sokratov is a consumer consultant to Waitemata DHB and a board member of Te Rau Matatini.
She has been leading a project on behalf of the Mental Health Commission that has been focused on rangatahi. She said the obvious reason for this is the increasing and disproportionate prevalence of mental illness, substance use and suicide among Māori youth who are also less likely to visit mental health services. Perhaps most significantly, Māori are younger, with 43 per cent of the Māori population being 19 years of age or below.
The project began with a literature review. International If we can start addressing problems early at the primary care end and provide young people with a positive experience the first time they access primary care, they’ll be much more likely to seek help from services again later on if they need them.”
Grant ChristiePassion Commitment Excellence 19
20. documents looked at included the United Nations Convention on the Rights of the Child, the United Nations Declaration on the Rights of Indigenous People and the Wharerata Declaration. Local documents included Blueprint II, Rising to the challenge, the Prime Minister’s Youth Mental Health Project, Waka Hourua and Drivers of Crime.
“What’s significant about Blueprint II is its focus on the ‘life course approach’ and we need to look at that in terms of planning and funding. The funding side of things is there but we seem to have lost the planning capacity so we have these arbitrary gaps in services.
“For example a service may only be available to a young person 14 years and older, but we know of young people with alcohol and drug problems who are under that age. So we need to think about some of this in terms of a life course approach to planning services.”
Wharerata Declaration
The aim of the project is to promote improved positive health outcomes for rangatahi, identify and share what’s working well and identify common areas of challenge for services. Ana said the Wharerata Declaration is useful for that.
It was developed out of the 2009 International Initiative for Mental Health Leadership gathering with New Zealand participation and has a strong indigenous focus. It supports indigenous leadership within communities and the health care workforce and recognises the protective power of culture and the need for integrating clinical and cultural models of care. It was signed by our Mental Health Commissioner in 2013.
“The Declaration requires services and practitioners to be culturally competent and safe, so it’s important we develop the Māori workforce at all service levels. It promotes both clinical and cultural evidence-based practice and strong and influential indigenous leadership.
“So based on all this it was determined that there was a need for some advocacy in this area and that we could unite or align the Mental Health Commissioner’s systemic advocacy function with principles from the Wharerata Declaration.
The project has established a partnership between the Mental Health Commission and Te Rau Matatini to ensure Māori leadership. The project team has visited 21 services in total, including DHBs and NGOS (rural and urban); Kaupapa Māori; mainstream; mental health; AOD and health promotion.
“The initial challenges we’ve noted include significant and persistent socio-economic challenges. We need more workforce development including recruitment and retention because we have a shortage in both mental health and AOD, and especially in terms of a rangatahi specific workforce. We also need organisational processes and structures to sustain and grow Māori clinical and cultural competence.
“Some strengths we found included that many services had incorporated Māori tikanga and kaupapa as ways of engaging with Māori. There was Māori leadership in many services and a strong Māori workforce in places. A lot of services are strengths-based, have rangatahi leadership and strong collaboration within their sector and communities.”
Ana said that, while we do need special expertise, the question is whether we need that expertise to be found only in specialist services. It is the expertise not the service that is the driver, the solution and the key.
“We tend to think about access as people coming to us, but we need to look again at how we define access, because access actually means people getting a service. It’s not about how they got there.
“We talk about ‘one stop shops’ and what Grant and Rubicon (see above) are trying to do is work towards what Professor Gluckman called a youth development focus in services. So we don’t separate out mental health from AOD or sexual health and say you go here or here. You do whatever’s needed to put the service in the places where your people need you and it’s not that difficult to do.
“If it’s a funding issue to move to this model then services could use their own funding streams to co-locate so that youth only need to go to one place to have multiple needs addressed.”
A project report has been written and signed off by the Mental Health and the Health and Disability Commissioners, but it has been embargoed until after the election. However, Ana said there are some meaningful recommendations in the report that people can look at when the time comes because they will have some relevance to what they do.
Auckland Police initiatives
Senior Sergeant Ross Endicott-Davies is Auckland’s Police District Mental Health Liaison Officer and Manager of the Alcohol Harm Prevention Unit.
Ross has been in the Police nearly 35 years, and moved into Alcohol Harm Prevention last year. He also holds the portfolios for Psychoactive Substances and Mental Health. But a lot of these issues interact with each other.
“We also deal a lot with suicidal ideation,” he said. “So our role often revolves around better ways of looking at things beyond locking people up.”
About 20,000 people come through the police custody unit every year, and a lot of those people have alcohol and drug related problems.
“So we’ve been pushing pretty hard for a health professional to work in our unit to provide brief interventions and help with referrals. Even just a short conversation can help reduce someone’s
Ana SokratovMatua Raki News 20 September 2014
21. drinking by about three drinks. We’ve got police staff in a custody environment who are not health professionals, but they do have to ask health-related questions, so some assistance would be great.”
Ross said a lot of people out there contact the Police service on the 111 line and sometimes they just call up for a chat. They may suffer from depression or some other mental health issue.
Matua Raki national manager Vanessa Caldwell said that within the sector, a lot of mental health and addiction workers probably don’t acknowledge the work the Police do enough.
“The police often see our clients at their very worst and have to deal with some pretty messy and awful situations, which have often been somewhat stabilised by the time they come to us,” she said. “We’d like to acknowledge our gratitude for that.”
Ross said you have to deal with everybody on a different level. It’s no good just kicking someone out the door and saying you need help. It has to be a whole lot more involved than that. We need some advice from the sector about how to deal with that person because we’re often legally constrained to let a person go, when you don’t want that person to go away and harm themselves.
“We have good working relationships with the various district health boards, but they all work differently and don’t always talk to each other, so it’s often a hard and complex situation for us. But the bottom line is we want better outcomes for people.
“So, somebody comes in with, say, an alcohol or other drug issue, and it’s a case of somebody sitting down with that person, having a brief intervention, and then maybe re-engaging them with one of the services out there.”
Ross said the Police are happy to talk with the sector. Aside from the personal suffering, people who are suicidal or in mental distress cost the country about $10m per year.
“The Ministry of Health and the Police Mental Health Intervention Team are working together to establish a way forward and address current issues and that includes ongoing training and a better understanding of the roles and responsibilities of both agencies.”
Senior Sergeant Ross Endicott- Davies
Some more photos from Leadership Day
Mike Douglas, The Salvation Army
Caro Swanson, Te Pou
Eroni Clarke and members of the Drua
Vanessa Caldwell and Klare Braye, Matua RakiPassion Commitment Excellence 21
22. Looking back on your first year as CEO, what was your most memorable experience?
My first service visit was to Arohata Women’s Prison in Tawa. I wanted to go there – it was our first Drug Treatment Unit and I had worked extensively in prisons before. I walked down the corridor and it could’ve been any prison I’d worked in, it looked very familiar. I got to the unit and the karanga, kapa haka, waiata… all told me this was actually very different.
What’s the most important thing you’ve learned in your first year?
I learned not to take myself too seriously, and that you need to stay grounded!
So how do you do that?
Going home to the West Coast… I stand on Barrytown beach and I feel connected.
We’ve got some family land there, so weekends mean a different work shirt, getting out on the land and doing ‘farm work’. Being in that environment keeps me grounded.
It’s a great antidote to city life and part of what keeps me well. As a leader I’m responsible for modelling self-care.
Talking of care – what’s a significant success CareNZ celebrated in your first year?
Working alongside local iwi and Corrections staff in Whanganui prison is a privilege. I’m proud of the way we are integrating our work with the Te Tirohanga programme.
What would you say are the biggest challenges CareNZ and the sector are facing?
I think we are at a pretty exciting crossroads. We have to find ways to do more, do it better, and quicker and help more people, all with the same money – that’s the reality. So focus, innovation, creativity and opening our minds to think differently are now more important than ever.
As we begin to really engage with the evidence and respond to
service user feedback, we need confidence as NGOs in our approach as professionals and providers of quality services. Let’s also broaden our definition of ‘drug treatment’ and collaborate with building recovery capital and the wellbeing agenda.
We also need to think differently about the workforce. Not everyone wants to spend their working life in our sector, so we need to make it easier for people with transferable skills to come in and out.
We’ve got to expand our cultural competence with Māori and Pasifika. Then there is work with the LGBT community who, sadly, have a high prevalence of alcohol and drug use. Our changing demographics, including increased migration from Asia and an ageing population, call for innovative thinking.
How would you see addiction treatment services developing in the future?
I think in the focus on ‘the treatment’, the initial work of accessing help is often overlooked.
The door into help needs to be wide and easy to walk through. It takes guts to pick up the phone and walk into a service. It’s all about relationships. Service users need to feel listened to, welcomed, respected and not judged. Get people in, give them a positive experience and it’ll be more likely they’ll come back. Then the next step on the road is easier.
Let’s help service users take responsibility from the start, so they can take the credit later. At the same time we continue support, including reminders – that’s simple now with texting. It’s easy to overlook this aspect of ‘treatment’ and think the real work is only in the sessions.
Then how can we more effectively include family and other support? People are with us only a brief time, so getting others involved is essential. At CareNZ, we’re certainly looking at how we can support the supporters.
Let’s also ask ourselves what treatment really involves. Learning to cook, eating a healthy diet, reducing caffeine and nicotine use, physical activity, mindfulness and positive alcohol/drug free social interactions are important. These aspects support therapeutic interventions and are part of clinical work.
CareNZ CEO
Kathryn Leafe
A year at the top at CareNZ
Little more than a year ago Kathryn Leafe was appointed CEO of CareNZ. We thought now would be a good time to catch up, find out about her first 12 months, her future plans and, of course, life on the West Coast. Matua Raki News 22 September 2014
23. Other practical steps can take place immediately – helping with sleep, panic attacks, urge surfing, strategies to stay safe. My best piece of work was with a highlighter and a map. One of my clients had been a street drinker. If he could make it sober to his first AA meeting, he could stay sober for the day. So we plotted his route without passing where he drank or could buy alcohol. It was simple but it worked. We can over-complicate things.
As professionals, we can’t ignore any aspect of a person, just because we feel uncomfortable or don’t know what to do. You need to show me that all of me is okay, whether it’s around sexuality or other diversity issues. I believe we have to get better at this.
How do we hear the service user voice?
In numerous ways – our clients, consumer advocates, our staff in all roles including administration, managers and CEOs and then being open to feedback wherever it comes from. For example, the media is rich with anecdotes and experiences.
What are your plans for the future of CareNZ?
We’ve just moved our national office so the Wellington clinic and central services have their own space and identity.
I’m excited about the results of our internal review – and how we all work together. It’s no easy feat with services across the country. So we have some new structures and training opportunities coming online. Externally, our new regional structure is going to impact positively on how our services work collaboratively, and with other agencies. I think this will really benefit our service users and that’s what we’re here for. Get people in, give them a positive experience and it’ll be more likely they’ll come back. Then the next step on the road is easier.”
Kathryn on the West Coast
Help keep our social page up to date!
Are there any arrivals or departures in your service? Help us keep our social page up to date. Send a short bio and a photograph to patricia. rainey@matuaraki.org.nz.
Stay up-to-date with the latest Matua Raki and addiction treatment sector news.
Check us out on Facebook www.facebook.com/matua-raki and
follow us on Twitter @MatuaRaki.
Subscribe to the electronic edition www.matuaraki.org.nz/enews. Passion Commitment Excellence 23
24. Among the variety of sessions are many presented by world leaders in their field, and most important areas are covered. Taken together, the meeting provides a picture of the state of mental health and addiction research and treatment internationally and an opportunity to gauge where we are in New Zealand.
Mental health and addiction treatment appears to be on the cusp of significant advances. Progress in pharmacogenetics promises to tell us which specific medication a person is likely to respond to best based on the gene variants for metabolising medications. This is already available in the US for response to SSRI antidepressants.
With research having increasingly rejected the limitations of DSM diagnoses, new areas are opening up, especially in terms of importing findings from other areas of health. For example, the common neurobiological pathways that underpin certain cancers and psychoses, and the promise that medications targeting those pathways for melanoma, for example, may have for treatment of psychosis, are leading to trials of new interventions.
Other examples include diabetes and obesity where the latter appears to be a significant factor in treatment resistance in mood disorders and the early indication that perinatal choline supplements may protect against and possibly reverse the mechanisms whereby a certain genetic variation underpins cortical development strongly associated with schizophrenia.
From an addiction and CEP perspective, Henry Kranzler’s impressive work on genetic variants and medication effectiveness for problematic alcohol use is progressing. Naltrexone has now been shown to have a relatively small effect on reducing alcohol consumption but this size effect is due to the fact that some respond very well to it and others do not. A polymorphism of an opioid receptor gene (OPRM1) explains almost all of this difference in response; those with a certain variant of the gene do very well on naltrexone; those without do not. The test is relatively simple to do from a sample of saliva once a laboratory is set up for it.
Kranzler is also researching the effectiveness of the anti- epileptic and mood stabilizer, Topiramate, on heavy alcohol use. Early indications are that a low dose has a moderate to large size effect in reducing heavy drinking. Response is almost entirely predicted by a common genetic variation in the gene coding for a subtype of the glutamate receptor. These gene variants are among
Fraser ToddWith research having increasingly rejected the limitations of DSM diagnoses, new areas are opening up, especially in terms of importing findings from other areas of health.”
Fraser Todd at the American Psychiatric Association
The American Psychiatric Association Annual Meeting is the largest mental health conference in the world, with over 10,000 delegates in attendance and over twenty different streams at any one time. Sessions range from very detailed research presentations on esoteric topics to basic clinical updates for general psychiatrists. Matua Raki News 24 September 2014
25. others that, in the near future, are likely to be tested routinely to indicate which medications individuals are likely to respond to.
Otherwise, there was little new. Early intervention work seems focussed on implementing brief assessments and interventions, something we have been doing for a number of years and are more advanced in. There were very few sessions on CEP, though increasingly other areas of mental health are acknowledging the importance of substance use.
You will probably have noticed that much of what I have mentioned involves biological research and medication. That is still an important window on mental health problems. However, this biological approach is increasingly being matched with related psychosocial interventions. Brain imaging studies have guided the development of specific psychological interventions for PTSD with Dissociative Features. This subtype of PTSD is common, hard to identify and responds poorly to standard PTSD treatments. However the addition of specific strategies to overcome the avoidance underlying dissociation (such as hypnosis or eye movement desensitisation and reprocessing) appears very useful in enhancing the effectiveness of subsequent standard CBT approaches for PTSD.
Perhaps the most useful presentations were those on Borderline Personality Disorder. This is common in people with addiction, but should perhaps be considered a developmental response to stress in adolescents which is often temporary, and which may persist if the skills to cope with the stress are not learned. While we have increasingly looked to highly specialised interventions such as DBT or mentalisation, the research of John Gunderson indicates that as long as certain basic skills and strategies are included, basic case management is as effective as the more specialised interventions.
So to conclude, where are we at in New Zealand with addiction and CEP treatment? I think there are exciting new interventions on the horizon which will take a few years to reach us, but in our approach to the people we work with we are up with the play in most respects and ahead of it in quite a few.
IIMHL organises systems for international networking, innovation sharing and problem solving across countries and agencies. The overall aim is to provide better outcomes for people who use mental health and addiction services and their families.
The philosophy behind the IIMHL Leadership Exchange is that once key leaders are linked together, they have the opportunity to begin collaborating and building an international partnership. The aim is to build relationships and networks that are mutually helpful for leaders, organisations and countries. It’s believed the benefits of such a collaborative effort will cascade down to all staff and consumers.
In 2013 lead exchange and network meetings were held in New Zealand. In 2014 it was the UK’s turn and 35 New Zealand representatives attended in June. Te Pou administrates New Zealand’s participation in IIMHL on behalf of the Ministry of Health.
Thoughts from Donna Blair
This was the third IIMHL exchange attended by Donna Blair, general manager of Te Utuhina Manaakitanga Trust, a kaupapa Māori AOD counselling service in Rotorua.
“For me the exchange was an opportunity to share knowledge and be inspired. The indigenous exchange I attended provided the opportunity to explore cultural competencies, and I was able to share the Takarangi Framework and how we have implemented it as a service. Each country had a different commitment to indigenous populations, but the passion of those who attend IIMHL, who strive
New Zealand and the International Initiative for Mental Health Leadership
The International Initiative for Mental Health Leadership (IIMHL) is a unique international collaborative that focuses on improving mental health and addiction services. IIMHL is a collaboration of eight countries: Australia, England, Canada, New Zealand, the Republic of Ireland, Scotland, USA and Sweden. Passion Commitment Excellence 25
26. to make a difference in their respective countries, was stimulating.
“It confirmed to me that we are on track as a service and, while we have some areas that require tweaking, we continue to grow. Our focus over the past few years has been Whānau Ora and whānau involvement. The exchange reminded me to remain focused and consider the big picture and to observe an ever-changing landscape.”
Donna says attending the exchange benefited addiction and mental health treatment in New Zealand because it encouraged continued conversation about having a culturally competent workforce, inclusive of non-Māori services.
Thoughts from Phil Grady
Odyssey House chief executive Phil Grady has been involved in a number of IIMHL exchanges. He says the value is immense on a number of levels.
“Having international leaders critique the services you provide is both humbling and hugely valuable. However, in my opinion, the true value is only realised if there is a positive change in how services are delivered and if these changes result in better outcomes for service users.
“At Odyssey we have radically changed how we support clients in treatment into employment and we are now seeing employment as a treatment outcome. In the exchange I was involved with this year, the focus was on co-existing problems and how to include, capture and utilise the consumer experience.”
Phil says that what stood out for him the most was the need to have more integrated systems of care, and the importance of finding new ways to support those who may need help.
“For me the exchange forces leaders to think outside the context in which we work. Often there is a tendency to believe that New Zealand leads the world in delivery of mental health and addiction services, and in many areas we do. However, as leaders we need to continue a drive to evolve, develop and improve our services.
“A common theme which ran through the conference was that it takes 17 years to fully embed a new practice, and I heard someone say it takes 24 years to fully remove a practice.
“For leaders, be it those in formal or informal roles, we have both a real challenge ahead but also a genuine opportunity to really make a difference to the lives of the people we see.”
Phil Grady
A tribute to Paraire Henare Tomoana Huata
Ko Takitimu te Waka,
Ko Tamatea-Ariki-Nui te tangata,
Ko Ngāti Kahungunu te Iwi.
To our esteemed Rangatira, Paraire Huata, who passed away on 12 May 2014.
I recall my first encounter with him almost 28 years ago. The Māori addiction workforce was limited and I was given the task to whai korero him into his new job. Let’s just say it was very uncomfortable for the student (me of course, in recovery) to be bestowed the greatest honour, to speak on behalf of the professor. I remember his comment “the wharepaku is two doors down on the left should you wish to know”. Since then we kept in contact supporting Māori development.
Donna Blair
Nā Takurua Tawera Pou WhakahaereMatua Raki News 26 September 2014