Presentation1.pptx, radiological imaging of intra cranial calcification.
•Télécharger en tant que PPTX, PDF•
33 j'aime•6,009 vues

Health &health

Recommandé
Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
En vedette (20)
Similaire à Presentation1.pptx, radiological imaging of intra cranial calcification.
Similaire à Presentation1.pptx, radiological imaging of intra cranial calcification. (20)
Plus de Abdellah Nazeer
Plus de Abdellah Nazeer (20)
Dernier
Dernier (20)
Presentation1.pptx, radiological imaging of intra cranial calcification.
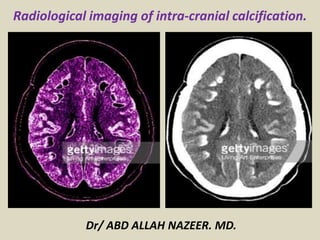
- 1. Dr/ ABD ALLAH NAZEER. MD. Radiological imaging of intra-cranial calcification.
- 2. Normal intracranial calcifications 1- Normal intracranial calcifications can be defined as all age-related physiologic and neurodegenerative calcifications that are unaccompanied by any evidence of disease and have no demonstrable pathological cause. The most common sites include: pineal gland seen in 2/3 of the adult population and increases with age calcification over 1cm in diameter or under nine years old may be suggestive of a neoplasm habenula it has a central role in the regulation of the limbic system and is often calcified with a curvilinear pattern a few millimeters anterior to the pineal body in 15% of the adult population choroid plexus a very common finding, usually in the atrial portions of the lateral ventricles calcification in the third or fourth ventricle or patients less than nine years of age is uncommon
- 3. basal ganglia calcification are usually incidental idiopathic findings that have an incidence of ~1% (range 0.3-1.5%) and increases with age usually, demonstrate a faint punctuate or a coarse conglomerated symmetrical calcification pattern see basal ganglia calcification for specific differential falx, dura mater or tentorium cerebelli occur in ~10% of the elderly population dural and tentorial calcifications are usually seen in a laminar pattern and can occur anywhere within the cranium petroclinoid ligaments common age-related degeneration sites and usually have laminar or mildly nodular patterns superior sagittal sinus common age-related degeneration sites and usually have laminar or mildly nodular patterns
- 4. 2. Post-traumatic. They are chronic sequels after ischemic or parenchymal hemorrhage from infarcts, trauma or surgery. In post radiation or chemotherapy calcification appear long time after treatment and are much more common in young children. 3. Congenital disorders (phakomatoses) - are hereditary disorders with multiple central nervous system and cutaneous abnormalities. Calcifications are commonly reported in tuberous sclerosis and Sturge-Weber syndrome, but can also appear in basal-cell nevus syndrome and neurofibromatosis type I and II. Tuberous sclerosis is a multisystemic autosomal-dominant disorder with typical manifestation of the triad: seizures, mental retardation, and facial angiofibroma. Neurofibromatosis type 1 is a multisystem neurocutaneous disorder associated with increased incidence of different tumors, such as optic nerve glioma and plexiform neurofibroma. Neurofibromatosis type II (MISME - multiple intracranial schwannomas, meningiomas and ependymomas). The most common calcifications seen in neurofibromatosis type 2 are the ones associated with disease-related tumors, such as meningiomas or ependymomas. Non tumoral calcifications are mainly nodular calcifications of the cerebellum, symmetric / often asymmetric calcifications of the choroid plexus and seldom cortical calcifications. Sturge-Weber syndrome also known as encephalotrigeminal angiomatosis, is the only phakomatoses that is not associated with intracranial neoplasms.
- 5. 4. Vascular disorders. Intracranial atherosclerosis. The presence of calcifications in the arterial wall of large intracranial vessels should be mentioned in radiologist report because of their association with atherosclerosis. The carotid siphon (~60%) is the most commonly affected vessel, calcifications in the vertebral artery (~20%) and middle cerebral arteries (~5%) are less common.[2,3] Other causes of vascular intracranial calcifications include: Aneurysm: although patent aneurysms may contain mural calcification, partially or entirely thrombosed aneurysms commonly have calcification. Arteriovenous malformation: are arterio-venous shunting with no capillary bed interfering. They may contain dystrophic calcification along the tortuous vessels and within the adjacent parenchyma with prevalence of 25 - 30%.[11] Cavernous malformation: are abnormal clusters of low-pressure blood vessels embedded in normal brain tissue. Occasionally have been described intracranial calcification in developmental venous anomaly (DVA), and capillary telangiectasia
- 6. 5. Infections. Patient with congenital infection present intracranial calcification with no specific appearance, often similar to any chronic brain injury (dystrophic calcifications). Calcifications in basal ganglia and the cortex are common features of all diseases that compose the TORCH syndrome (toxoplasmosis, other, rubella, cytomegalovirus, herpes simplex virus). Calcifications in patients infected with toxoplasmosis may resolve after treatment. The intracranial calcifications patterns in acquired infections, although not specific are extremely useful in making the correct diagnosis and evaluating disease progression. Cysticercosis, tuberculosis, HIV and cryptococcus are the most common disease typically associated with calcifications. 6. Inflammatory disorders. Systemic lupus erythematosus. In systemic lupus erythematosus cerebral calcifications has been seen in the basal ganglia, centrum semiovale, cerebellum and thalamus. Neurosarcoidosis. The neurosarcoidosis lesion appearance is nonspecific; granulomatous masses are seen as hyperdense nodules or calcification and involves the parenchyma, nerve, the leptomeninges, and dura matter.
- 7. 7. Tumors. Intra-axial: oligodendroglioma, astrocytomas, medulloblastoma, ganglioglioma, DNET, metastases. Extra-axial: meningioma, pineal tumors, pituitary tumors, craniopharyngioma, epidermoid, dermoid, teratoma, colloid cyst, lipoma, metastases. Intraventricular: ependymoma, choroid plexus tumors, central neurocytoma, metastases. The most common intracranial neoplasms associated with calcifications are oligodendroglioma (70-90%), craniopharyngioma (50-80%), germ cell neoplasms, ganglioglioma (35-50%), meningioma (20-25%), choroid plexus papilloma (25%), medulloblastoma (20%), low grade astrocytoma (20%), and pilocytic astrocytoma (10%). Calcifications are rarely described in schwannomas, and dermoid and epidermoid tumor. Craniopharyngioma is a benign tumor derived from Rathke,s pouch epithelium. Calcification is described the hallmark of a craniopharyngioma and occurs in about 90% of tumors. 8. Metabolic/ endocrine pathologies. Hyperparathyroidism/Hypoparathyroidism/Hypothyroidism/MELAS syndrome Endocrine disorders involving calcium homeostasis are frequent associated with intracranial calcification. Most common locations are the basal ganglia, but also subcortical white matter, thalami and cerebellum. Fahr disease, a familial cerebrovascular ferrocalcinosis, is a rare condition starting in childhood presenting with progressive mental deterioration. It is characterised by extensive deposits of iron and calcium in the globus pallidus, dentate nuclei and subcortical white matter.
- 8. NECT (a) Calcified bilateral petroclinoid ligaments. (b) Small calcification along the tentorium. (c) Bilateral choroid plexus (arrowheads), pineal and habenular (arrow) calcification.
- 9. Different pattern of pineal gland calcification: (a) nodular, (b) curvilinear, (c) punctate.
- 10. NECT Linear calcified falx cerebri.
- 11. Axial NECT in two patients. Different type of bilateral globus pallidus calcifications (a) coarse conglomerated and (b) punctate.
- 12. Non-contrast CT of the head shows dense bilateral basal ganglia calcification (black arrows).
- 14. Right caudate head dense calcification in a 55 years old male.
- 15. Post surgery right frontal cortical(red arrows) and dural (white arrow) calcification in a patient with LMNH.
- 16. NECT in a patient with hydrocephaly (star). Left posttraumatic dural calcification (after epidural hematoma)(arrow).
- 17. Right chronic (hypodense) subdural hematoma (stars). NECT - small linear dural calcification (arrows)
- 18. Multiple calcified subependymal hamartomas along the lateral ventricles and foramen of Monro in two different patient with tuberous sclerosis; (a ,c) infratentorial small calcification (b, d) supratentorial partial calcified subcortical tuber (white arrow).
- 19. a, b. Periventricular calcifications of subependymal nodules in two different patients with tuberous sclerosis. Subcortical calcified tuber (arrow) in the right parietal lobe (a).
- 20. Multiple calcified subependymal hamartomas along the lateral ventricles and foramen of Monro.
- 21. Neurofibromatosis Type I; (a)NECT - Multiple small intracerebral calcification, widened optic nerve foramina (large white arrow), (b) MRI with Gd shows multiple intracerebral tumoral lesions (red arrows) little enhancement(green arrows) and enlarged optic nerves and optic chiasm (small white arrow).
- 22. Plain lateral skull radiograph demonstrates the typical gyriform pattern of cortical calcification (arrows) in the occipital region.
- 23. (a) X-ray lateral view of skull showing 'tram-track' calcification. (b) Computed tomography (CT) scan of brain showing atrophy and extensive gyral pattern of calcification of left cerebral hemisphere
- 24. M 55 y, presenting facial angioma and epilepsy. NECT reveal typical left frontoparietal gyral calcification in Sturge-Weber Syndrome (red arrows); left fontal lobe atrophy associated (white arrow).
- 26. Sturge-Weber, Gyriform cortical calcifications with ipsilateral atrophy and enlarged choroid plexus.
- 27. Megadolico vertebro-basilar system and internal carotid artery with multiple small atherosclerotic calcified plaques.
- 28. Calcified plaques in the wall of vertebrobasilar system and bilateral internal carotid (red arrows), middle cerebral artery (white arrow)
- 29. Plain X rays of skull. (a) and (b) Curvilinear midline calcification in the wall of aneurysm of vein of Galen.
- 30. Giant left middle cerebral artery thrombosed aneurysm(red arrows). (a) NCET, Rim like wall calcification and granulosus calcification; moderate edema developed in temporo-insular left region, (b)MRI and (c) CECT confirming partial thrombosed aneurysmal; enhanced residual lumen (green arrow).
- 31. Arterio-venous malformation. Right frontal lobe heterogeneous lesion: (a) with small hypodense central area, multiple serpentines vascular calcification (white arrows), (b) intense enhanced vascular tracks located peripheral (red arrows).
- 32. Angio-CT: MIP and source image - complex vascular malformation: aneurysm of the pericallosal artery and partially thrombosed saccular venous dilatation with peripheral calcifications (arrows).
- 33. Developmental venous anomaly. Right cerebellar hemisphere heterogeneous lesion with small hypodense central area, multiple serpentines vascular calcification (red arrows), vascular tracks with "medusa head" sketch located peripheral with intense enhancement (white arrows).
- 34. Cavernous malformation. (a) NECT Small hyperintense lesion, with punctate calcification in left periventricular white matter, near occipital lateral ventricle horn. (b )MRI. "Popcorn" appearance with hypointense hemosiderin rim on T2-wi (green arrow); T1-wi with Gd - shows small venous malformation associated (white arrow).
- 35. Massive calcifications in right frontal lobe colon cancer metastasis.
- 36. Subcortical/cortical large left frontal oligodendroglioma (a) NECT, (b) MRI with Gd - heterogenous mass with nodular calcification (arrows) and cystic component (star).
- 37. Obstructive craniopharyngioma. Axial NECT (a)- Heterogenous suprasellar masse with peripheral calcification (red arrows) and hypodense area; hydrocephaly associated(star); (b) CECT - Little enhancement (small white arrows) and mild displacement of Circle of Willis (large white arrow).
- 38. Large left parasellar meningioma. (a) NECT heterogenous mass with diffuse calcification, (b) MRI with Gd- homogenous enhancement (white arrow).
- 39. NECT - large left meningioma in two different patient with (a) circular calcification pattern and (b) radial calcification pattern.
- 40. Meningioma. (a) NECT Large left meningioma with radial pattern calcification, (b) CECT - homogenous enhancement.
- 41. Mineralizing microangiopathy. Small bilateral calcifications involving the thalamo-lenticular regions and the subcortical white matter (arrows).
- 42. AP X-ray of the skull (2A) and lateral (2B) view show a ghost-like appearance (‘alien look’) with cranial hyperostosis (black arrowheads). Focal bilateral symmetrical intracranial calcification is seen (black arrows). Thinned out and focally absent enamel with missing teeth and cavities are seen (thin white arrows) with broadened mandible (thick white arrow).
- 43. Pericallosal and interhemispheric lipoma with calcification.
- 44. Rare idiopathic disorders such as Fahrs disease.
- 45. Congenital infections with intra-cranial calcification.
- 46. Occipital Calcification with neonatal thyrotoxicosis.
- 47. Nonenhanced (left) and enhanced (right) CT scans of the brain in a patient with neurocysticercosis show multiple ring-enhancing lesions with perifocal edema.
- 48. Nonenhanced (left) and enhanced (right) CT images of the brain in a patient with neurocysticercosis show an enhancing disk lesion with perifocal edema suggestive of the granulomatous form of disease (arrow). Multiple ring lesions are also apparent; these are suggestive of the colloid stage of neurocysticercosis.
- 49. CT images of the brain in a patient with neurocysticercosis show numerous parenchymal lesions.
- 50. Cockayne syndrome with extensive intracranial calcification
- 51. (A) Magnetic resonance axial section T2* GRE sequence with extensive brain calcification. (B) Computed tomography scan axial section with basal ganglia calcification.
- 52. An 8-year-old male with a long complicated medical history was found to have hard-to-miss calcifications on the plain skull x-ray (a, d). The NCECT (b, e) and 3D reconstructions (c, f) show a large amorphous calcification originating from the basal ganglia, extending into the right lateral ventricle of the patient diagnosed with tuberous sclerosis. Subependymal nodules associated with tuberous sclerosis can calcify with age, typically presenting with globular or sometimes ring-like calcification.
- 53. A 17-year-old female with seizures presented with a large calcified mass apparently arising from the left temporal lobe. The calcification pattern (mostly peripheral) and morphology (“popcorn appearance”) strongly suggested a vascular lesion such as a cavernous malformation (cavernous angioma) or, less likely, a calcified haemangioma. Upon excision, the mass was later found to be a choroid plexus papilloma, shown in the axial NCECT in soft tissue (a) and bone windows (b) as well as the coronal NCECT reconstruction in soft tissue (c) and bone windows (d)
- 54. A 60-year-old male known HIV patient presented with seizures. The solid calcifications on NCECT at the right frontal (a) left basal ganglia(b) and right parietal areas (c) represent sequelae following treatment for documented toxoplasmosis. 3D reconstruction (d). In congenital toxoplasmosis, calcifications have been shown to decrease in size or even completely resolve with treatment
- 55. An adult case of leukoencephalopathy with intracranial calcification and cyst.
- 58. Pachygyria, and cerebellar hypoplasia, B: generalized intracranial calcification, C: intracranial calcification and cerebellar hypoplasia.
- 59. Conclusion 1.Intracranial calcifications are relatively common and CT is the most sensitive method in their detection and proper location. 2.The presence of intracranial calcifications, their distribution and semiologcal appearance in association with the clinic and biological data and in particular cases the follow up of the patient, help to make an accurate diagnosis.
- 60. Thank You.