Diabeticretinopathy30 3-2011-121109075116-phpapp01
•Télécharger en tant que PPTX, PDF•
3 j'aime•195 vues

Prevention of blindness in Diabetic Retinopathy

Recommandé
Contenu connexe
Tendances
Tendances (20)
Similaire à Diabeticretinopathy30 3-2011-121109075116-phpapp01
Similaire à Diabeticretinopathy30 3-2011-121109075116-phpapp01 (20)
Plus de Md Afzal Mahfuzullah
Plus de Md Afzal Mahfuzullah (12)
Dernier
Dernier (20)
Diabeticretinopathy30 3-2011-121109075116-phpapp01
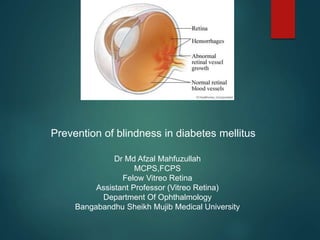
- 1. Prevention of blindness in diabetes mellitus Dr Md Afzal Mahfuzullah MCPS,FCPS Felow Vitreo Retina Assistant Professor (Vitreo Retina) Department Of Ophthalmology Bangabandhu Sheikh Mujib Medical University
- 2. Diabetes mellitus Diabetes is one of the most prevalent and serious non- communicable diseases all over the world. Among the adults (age 20-79 years) with diabetes in the top five South East Asian countries, Bangladesh is in the second position.
- 3. Diabetes mellitus, Cont The number of people with diabetes in Bangladesh was 5.10 million in 2013, which is expected to increase to 8.20 million by 2035. Reason for blindness in diabetes is due to diabetic retinopathy
- 4. Diabetic Retinopathy Diabetic retinopathy is the major ocular complication associated with diabetes. It represents the leading cause of legal blindness in the working-age population of developing countries. Classically diagnosis is based on abnormalities of the retinal microvasculature,
- 5. Diabetic Retinopathy, Cont Diabetic retinopathy is now widely recognized as a neurovascular disease. All patients with diabetes are at increased risk for eye disease including diabetic retinopathy, proactive measures, and timely intervention can prevent or delay subsequent vision loss.
- 6. Diabetic Retinopathy, Cont Systemic management of diabetes by combined control of glycaemia, blood pressure, and serum lipid levels remains the most important method of preventing diabetic retinopathy onset and progression. Once detected, surgical and medical interventions including photocoagulation, intravitral drug injection and , surgical vitrectomy can help to preserve vision.
- 7. Risk factors Duration of diabetes Most important Pt diagnosed before age 30 yr 50% DR after 10 yrs 90% DR after 30 yrs Poor metabolic control Less important, but relevant to development and progression of DR HbA1c ass. with risk Pregnancy Associated with rapid progression of DR Predicating factors : poor pre-pregnancy control of DM, too rapid control during the early stages of pregnancy, pre-eclampsia and fluid imbalance
- 8. Risk factors,Cont Hypertension Very common in patients with DM type 2 Should strictly control (<140/80 mmHg) Nephropathy Ass with worsening of DR Renal transplantation may be ass with improvement of DR and better response to photocoagulation Others Obesity, increased BMI, high waist-to-hip ratio Hyperlipidemia Anemia
- 9. Pathogenesis Microvascular leakage Microvascular occlusion
- 10. Microvascular leakage Degeneration and loss of pericytes Plasma leakage Intraretinal hemorrhageHard exudate (Circinate pattern) Capillary wall weakening microaneurysm Retinal edema
- 11. Microvascular occlusion Neovascularization and fibrovascular proliferation VEGF Increased plasma viscosity Deformation of RBC Increased platelets stickiness Decreased capillary blood flow and perfusion Endothelial cell damage and proliferation Capillary basement membrane thickening Retinal hypoxia A-V shunt IRMA* *intraretinal microvascular abnormalities Proliferative retinopathy Rubeosis iridis
- 13. Classification Non-proliferative diabetic retinopathy (NPDR) Proliferative diabetic retinopathy (PDR) Advanced diabetic eye disease(ADED)
- 14. Non-proliferative diabetic retinopathy Mild NPDR Moderate NPDR Severe NPDR Very Severe NPDR
- 15. Signs Of NPDR Microaneurysm Retinal hemorrhage “Dot or Blot” “Flame or Splinter shape” hemorrhage Hard exudate Cotton wool Spot Venous beading Intra-retinal microvascular abnormalities (IRMA)
- 17. Microaneurysm
- 18. Moderate NPDR More microaneurysms Scattered hard exudates Cotton-wool spots
- 19. Hemorrhage
- 20. Severe NPDR 4-2-1 rule 4 quadrants of severe retinal hemorrhages 2 quadrants of venous beading 1 quadrant of IRMA Very severe NPDR more than 1 of above
- 21. Microaneurysms may leak plasma constituents into the retina Scattered hyperfluorescent
- 22. Retinal Hemorrhage Capillary or microaneurysm is weakened rupture intraretinal hemorrhages Dot & blot hemorrhages Deep hemorrhage - inner nuclear layer or outer plexiform layer Usually round or oval Dot hemorrhages - bright red dots (same size as large microaneurysms) Blot hemorrhages - larger lesions
- 23. Retinal Hemorrhage,Cont Flame-shape or splinter hemorrhages More superficial - in nerve fiber layer Absorbed slowly after several weeks Indistinguishable from hemorrhage in hypertensive retinopathy May have co-existence of systemic hypertension BP must be checked
- 24. Dot Spot VS Flame Shape
- 25. Dot Spot VS Flame Shape
- 26. Hard exudate Intra-retinal lipid exudates Yellow deposits of lipid and protein within the retina Accumulations of lipids leak from surrounding capillaries and microaneuryisms May form a circinate pattern Hyperlipidemia may correlate with the development of hard exudates
- 28. Cotton Wool Spot White fluffy lesions in nerve fiber layer Result from occlusion of retinal pre-capillary arterioles supplying the nerve fibre layer with concomitant swelling of local nerve fibre axons Also called "soft exudates" or "nerve fiber layer infarctions"
- 30. Hard Exudate VS Cotton Wool Spot
- 33. Diabetic maculopathy Macular ischemia Retinal capillary non-perfusion Progressive NPDR Macular edema Increased retinal vascular permeability Seen in both NPDR and PDR Focal or diffuse or mixed
- 35. Focal macular edema Diffuse macular edema
- 36. Macular ischemia
- 37. Clinical Significant Macular Edema (CSME) 1 of 3 Retinal edema within 500 microns of centre fovea Hard exudates within 500 microns of fovea if ass with adjacent retinal thickening Retinal edema > 1 disc diameter, any part is within 1 disc diameter of centre of fovea
- 38. Proliferative diabetic retinopathy 5% of DM pt. Finding Neovascularization : NVD, NVE Vitreous changes Advanced diabetic eye disease Final stage of Uncontrolled PDR Blindness from persistent vitreous hemorrhage, tractional RD, opaque membrane formation,
- 41. Fluorescein dye leakage is seen in neovascularized area Neovascularization of elsewhere
- 43. Rubeosis iridis (neovascularisation of the iris) Neovascular glaucoma
- 45. Vitreous changes
- 46. Tractional retinal detachmentVitreous hemorrhage
- 47. New vessels of the disc (advanced)
- 50. Signs & symptoms of DR Blurred or distorted vision or difficulty reading Floaters Partial or total loss of vision a shadow or veil across patient’s visual field ocular pain
- 53. Medical therapy Treat underlying conditions Control blood sugar – HbA1c < 7 Control blood pressure – SBP < 130 mmHg Control lipid profile – TG, LDL Correct anemia Control diabetic nephropathy
- 54. Management, Cont Laser Photocoagulation(PRP) Intravitreal injection Anti VEGF Intravitreal triamcinolone acetonide (Steroid) Vitreoretinal surgery
- 55. Photocoagulation Focal or Grid Laser (CSME in both NPDR and PDR) Panretinal Photocoagulation (PRP) (PDR)
- 56. Laser Panretinal photocoagulation (PRP) PDR New vessels Vitreous or preretinal hemorrhage New vessels on optic disc or within 1,500 microns from optic disc rim Large new vessels Iris or angle neovascularization CSME
- 57. Laser panretinal photocoagulation (PRP) Inducing involution of new vessels Preventing vitreous hemorrhage and preventing visual loss Limitations : Patient must have clear lens and vitreous If cataract treat before laser PRP If vitreous hemorrhage vitrectomy + laser photocoagulation
- 61. Advanved Diabetic Eye Disease(ADED)
- 62. Indications for pars plana vitrectomy (PPV) in DR Severe persistent vitreous hemorrhage Progressive tractional RD (threatening or involving macula) Combined tractional and rhegmatogenous RD Premacular subhyaloid hemorrhage Recurrent vitreous hemorrhage after laser PRP
- 63. Vitreous hemorrhage Tractional retinal detachment
- 64. Vitreoretinal Surgery Pars plana vitrectomy (PPV) Membrane peeling (MP) Endolaser (EL) Fluid gas exchange (FGX) Silicon oil injection SF6 C3F8
- 65. Patient Profile Mrs Nargis Akhter Age:45 years Diabetic for 10 years (On Insulin) Visual acuity : Right eye: Hand movement Left eye: 3/60
- 67. After 1 month of vitrectomy Surgery (PPV) Visual acuity Right eye: 6/18 Left eye:6/36 Before surgery After surgery
- 68. Take home message Diabetic retinopathy is a complex neurovascular disorder that may threaten vision in all patients with diabetes. A proactive, multidisciplinary approach can help significantly reduce the risk for vision loss from diabetes and associated eye disease such as diabetic retinopathy. The intricate mechanisms contributing to disease pathogenesis continue to be elucidated. Future research should be integrative in nature, addressing both systemic and ocular factors as they contribute to vision impairment in diabetes.
- 69. Thank
Notes de l'éditeur
- I. Focal. (a) A ring of hard exudates temporal to the macula; (b) FA late phase shows focal area of hyperfluorescence due to leakage corresponding to the centre of the exudate ring. 2. Diffuse. (c) Dot and blot haemorrhages; (d) FA late phase shows extensive hyperfluorescence at the posterior pole due to leakage.
- 3./schaemic. (e) Dot and blot haemorrhages and cotton-wool" spots; (f) FA venous phase shows hypofluorescence due to capillary non-perfusion at the macula and elsewhere