Normal birth can cause tears to the vagina and the surrounding tissue, usually as the baby's head is born, and sometimes these tears extend to the rectum. These are repaired surgically, but take time to heal. To avoid these severe tears, it is recommended making a surgical cut to the perineum with scissors or scalpel to prevent severe tearing and facilitate the birth. This intervention, known as an episiotomy, is used as a routine care policy during births in some countries. Both a tear and an episiotomy need sutures, and can result in severe pain, bleeding, infection, pain with sex, and can contribute to long term urinary incontinence.
Episiotomies—incisions made between the vagina and anus during childbirth—have long been a topic of debate among clinicians, researchers and advocates. Outdated clinical guidelines previously recommended the routine use of episiotomy to avoid natural vaginal tearing. Over the past two decades, a growing body of literature and increased advocacy efforts have led to a general consensus that episiotomy should not be conducted as a standard practice. Nevertheless, in many parts of the world, the majority of women still undergo episiotomy during childbirth.
In women where no instrumental delivery is intended, selective episiotomy policies result in fewer women with severe perineal/vaginal trauma.
2. DEFINATION
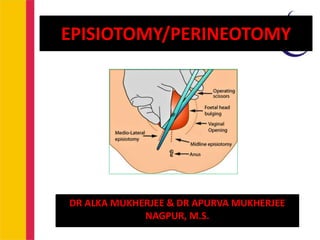
Episiotomy/ perineotomy, is a surgical incision of the perineum and
the posterior vaginal wall generally done by a obstetrician
The episiotomy is a technique originally designed to reduce the
incidence of severe perineal tears (third and fourth-degree) during
labor.
The general idea is to make a controlled incision in the perineum, for
enlargement of the vaginal orifice, to facilitate difficult deliveries.
Ideally, an episiotomy would relieve pressure on the perineum
resulting in an easily repairable incision when compared to
uncontrolled vaginal trauma.
2DR MUKHERJEE ALKA NAGPUR
3. DR MUKHERJEE ALKA NAGPUR 3
• Country Episiotomy rate (year)
• China 44.9% (2002)
• India 45.0% (2003)
• Indonesia 53.5% (2005)
• Iran 79.2% (2012)
• Malaysia 46.0% (2005)
• Philippines 63.7% (2005)
• Thailand 91.8% (2005)
• South Africa 63.3% (2003
4. Indications
• The selective use of episiotomy.
• According to a cochrane database review by xu qian et
al., The implementation of a selective episiotomy policy
in women undergoing non-operative vaginal delivery,
resulted in significantly fewer women with severe
perineal trauma when compared to women who
underwent routine episiotomy
• However, there is still no solid supporting evidence for
the benefits of its use as a stand-alone elective
procedure.
4DR MUKHERJEE ALKA NAGPUR
5. a. Threatened perineal injury in primigravidae
b. Rigid perineum
c. Forceps, breech, occipitoposterior or face delivery.
d. Anticipating perineal tear
e. Operative delivery
f. Previous perineal surgery
A retrospective cohort study suggested that episiotomy use may put
multiparous women at increased risk for third and fourth-degree
tears.
Because of such studies, the American College of Obstetricians and
Gynecologists recommends against the routine use of episiotomy.
CONTRAINDICATIONS
COMMON INDICATIONS
5DR MUKHERJEE ALKA NAGPUR
6. TIMING
Bulging thinned
perineum during
contraction just
prior to crowning
(when 3–4 cm of
head is visible)
• During forceps
delivery, it is
made after the
application of
blades.
If done early, –
the blood loss
will be more.
If done late, – it
fails to prevent
the invisible
lacerations of the
perineal body
6DR MUKHERJEE ALKA NAGPUR
7. EQUIPMENT
1) Episiotomy scissors
2) Needle holder
3) Stitches
4) Surgical drape
5) Local anesthetic
6) Hemostatic
forceps/tissue forceps
7) Sim's speculum
8) Foley catheter
9) Syringe, needles
10) Scalpel/blade
11) Kidney tray
PREPARATION
a) Ensure that the woman
consents to the procedure
b) Ensure good lighting
c) Assess the perineum and
decide about the type of
episiotomy
d) Ensure adequate anesthesia
e) Check the equipment before
starting the procedure
f) Count swabs before and after
performing the episiotomy
repair
g) Use a loose, continuous non-
locking method for vaginal
mucosa and perineal muscles
and a continuous subcuticular
technique for perineal skin
7DR MUKHERJEE ALKA NAGPUR
8. STRUCTURES CUT ARE
I. Posterior vaginal wall
II. Superficial and deep transverse perineal muscles,
bulbospongiosus and part of levator ani
III. Fascia covering those muscles
IV. Transverse perineal branches of pudendal vessels and nerves
V. Subcutaneous tissue and skin.
8DR MUKHERJEE ALKA NAGPUR
9. TYPES OF EPISIOTOMY
1. Median (midline, medial) episiotomy - Median episiotomy begins at the
posterior fourchette and runs along the midline through the central tendon
of the perineal body.The extension of the incision should be roughly half of
the length of the perineum.This type of episiotomy is commonly used in the
USA and Canada.
2. Modified median episiotomy
A modification of median episiotomy is performed by adding two transverse
incisions in opposite directions just above the expected location of the anal
sphincter. The transverse incision is performed on each side, perpendicular
to the midline, so that it measures 2·5 cm in total.The use of this
modification is claimed to increase the diameter of the vaginal outlet by
83% compared with a standard median episiotomy, possibly by separation
of both perineal membrane/sphincter attachments, and so allows true
posterior displacement of the anus with no risk of any resultant traction
injury
9DR MUKHERJEE ALKA NAGPUR
11. 3. ‘J’‐shaped episiotomy
This episiotomy commences with a midline incision and is then curved laterally
to avoid the anus. In this technique curved scissors are used starting in the
midline of the vagina until the incision is 2·5 cm from the anus. Then the ‘J’
is made by directing the incision towards the ischial tuberosity away from the
anal sphincter.
4. Mediolateral episiotomy
This is the most frequently used type of episiotomy in Europe. Defined as an
incision beginning in the midline and directed laterally and downwards away
from the rectum.
5. Lateral episiotomy
This type of episiotomy was first described in 1850. It begins in the vaginal
introitus 1 or 2 cm lateral to the midline and is directed downwards
towards the ischial tuberosity.Lateral episiotomy is mentioned very rarely in
the obstetric literature.
11DR MUKHERJEE ALKA NAGPUR
13. 6. Radical lateral (Schuchardt incision) - often considered to be a
non‐obstetrical incision. It is a fully extended episiotomy, which carries
deep into one vaginal sulcus and is curved downward and laterally part way
around the rectum.
It may be performed at the beginning of radical vaginal hysterectomy or
trachelectomy to permit easy access to the parametrium,to enable
extraction of a neglected vaginal pessary
or, very occasionally, to facilitate childbirth in complicated deliveries (large
head, difficult breech or for correction of shoulder dystocia).
7. Anterior episiotomy or deinfibulation - (the procedure of opening the scar
associated with some degrees of female genital mutilation) is usually
performed during delivery on women who have had female infibulation
performed previously.
The practitioner’s finger is inserted through the introitus and directed towards
the pubis. To free the scar, fused labia minora are incised in the midline
until the external urethral meatus can be seen and the anterior flap is
completely open.
The clitoral remnants should not be incised. Another type of episiotomy
(preferably mediolateral) may be required during delivery.
13DR MUKHERJEE ALKA NAGPUR
14. TYPES OF EPISIOTOMY
• Types of episiotomy. 1: median episiotomy, 2: modified
median episiotomy, 3: ‘J’‐shaped episiotomy, 4: mediolateral
episiotomy, 5: lateral episiotomy, 6: radical lateral (Schuchardt
incision), 7: anterior episiotomy (white arrow). 14DR MUKHERJEE ALKA NAGPUR
16. Recommendations
Standardized classification system in terms of
The origin of the incision, the direction (e.G. The angle of the cut
In the case of medio-lateral episiotomy), and the length, based
Upon current research evidence
There is a need to standardize the practice of mediolateral
Episiotomy, both to inform practice in those specific situations
Where it is clearly clinically indicated, but also particularly in the
Context of future research into the risks and benefits of
Episiotomy with respect to major perineal trauma.
16DR MUKHERJEE ALKA NAGPUR
19. STEP I
Preliminaries
The perineum is thoroughly swabbed with
antiseptic (povidone-iodine) lotion and draped
properly.
Local anesthesia –
The perineum, in the line of proposed incision is
infiltrated with 10 mL of 1% solution of lignocaine
19DR MUKHERJEE ALKA NAGPUR
20. STEPS OF MEDIOLATERAL EPISIOTOMY
STEP II
1. Incision - Two fingers are placed in the vagina between the presenting
part and the posterior vaginal wall by a curved or straight blunt pointed
sharp scissors (scalpel may also be used)
2. One blade of which is placed inside, in between the fingers and the
posterior vaginal wall and the other on the skin
3. The incision should be made at the height of an uterine contraction
when an accurate idea of the extent of incision can be better judged
from the stretched perineum.
4. Deliberate cut should be made starting from the center of the fourchette
extending laterally either to the right or to the left
5. It is directed diagonally in a straight line which runs about 2.5 cm away
from the anus.
6. The incision ought to be adequate to serve the purpose for which it is
needed,
7. The bleeding is usually not sufficient to use artery forceps unless the
operation is done too early or the perineum is thick.
20DR MUKHERJEE ALKA NAGPUR
21. STEP III TIMING OF REPAIR
a) The repair is done soon after expulsion of placenta.
b) If repair is done prior to that, disruption of the wound
is inevitable, if subsequent manual removal or
exploration of the genital tract is needed.
c) Oozing during this period should be controlled by
pressure with a sterile gauze swab and bleeding by
the artery forceps.
d) Early repair prevents sepsis and eliminates the
patient’s prolonged apprehension of “stitches”.
21DR MUKHERJEE ALKA NAGPUR
22. a) REPAIR STEPS Preliminaries
• Lithotomy position.
• A good light source
• Cleansed with antiseptic solution.
• Blood clots are removed from the vagina and the wound
area.
• The patient is draped properly and repair should be done
under strict aseptic precautions.
• If the repair field is obscured by oozing of blood from
above, a vaginal pack may be inserted and is placed
high up.
22DR MUKHERJEE ALKA NAGPUR
24. ADVANTAGES
Maternal:
(a) a clear and controlled incision is easy to repair
and heals better
(b) reduction in the duration of second stage
(c) Reduce the trauma to pelvic floor muscles
Fetal: – It minimizes intracranial injuries specially
in premature babies or after-coming head of
breech
24DR MUKHERJEE ALKA NAGPUR
25. REPAIR
The principles to be followed are
Perfect hemostasis,
To obliterate the dead space and
Suture without tension.
LAYERS • The repair is to be done in the following order:
(1) Vaginal mucosa and sub-mucosal tissues
(2) Perineal muscles
(3) Skin and subcutaneous
25DR MUKHERJEE ALKA NAGPUR
26. (1) Repair steps
a. The vaginal mucosa is sutured first. The first suture is
placed at or just above the apex of the tear.
b. Thereafter, the vaginal walls are apposed by interrupted
sutures with Polyglycolic acid suture (dexon) or no. “0”
chromic catgut, from above downwards till the
fourchette is reached.
D. The suture should include the deep tissues to obliterate
the dead space.
E. A continuous suture may cause puckering and
shortening of the posterior Vaginal wall.
F. Care should be taken not to injure the rectum.
26DR MUKHERJEE ALKA NAGPUR
27. POSTOPERATIVE CARE
• Dressing
• Comfort – MgSo4 compression – Infrared heat – Ice
pack – Analgesic (ibuprofen)
• Ambulance
• Removal of stitches – Non-absorbable (6th day)
Watch for
• Vital signs
• Symptoms and signs of wound infection
• Any abnormal discharge
• Pain score
• Urine output
• Patient ambulation and level of activity
27DR MUKHERJEE ALKA NAGPUR
28. IMMEDIATE COMPLICATIONS
(1) Extension of the incision to involve
the rectum.
(2) Vulval hematoma
(3) Infection: (A) throbbing pain on the
perineum (B) rise in temperature
(C) the wound area looks moist, red
and swollen and (D) offensive
discharge
TREATMENT:
(a) To facilitate drainage of pus
(b) Local dressing with antiseptic
powder or ointment
(c) MgSO4 compression or application
of infrared heat to the area to
reduce edema and pain
(d) Systemic antibiotic
(4) Wound dehiscence
(5)Injury to anal sphincter causing
incontinence of flatus or
feces.
(6) Rectovaginal fistula
(7)Necrotizing fasciitis (rare) in a
woman who is diabetic or
immunocompromised
REMOTE COMPLICATION
Dyspareunia
Chance of perineal
lacerations in subsequent
labor
Scar endometriosis (rare).
28DR MUKHERJEE ALKA NAGPUR
29. Enhancing Healthcare Team Outcomes
Imperative
To obtain consent from the patient and provide
education
Clearly communicating about the risks, benefits, and
alternatives for episiotomy
Ensuring that adequate exposure of the perineum is
maintained.
The patient should receive further written
information about the procedure and instructions on
how to care for their wounds after the procedure.
Counseling the patient on the proper use of
analgesics and anti-inflammatory drugs within the
first 24 to 72 hours after episiotomy.
29DR MUKHERJEE ALKA NAGPUR
30. TEACH THE PATIENT SELF-CARE
To relieve pain or
discomfort:
Ask to apply ice packs
right after the birth.
Using ice packs in the
first 24 hours after birth
decreases the swelling
and helps with pain.
Take warm baths but
wait until 24 hours after
giving birth. Make sure
that the bathtub is
cleaned with a
disinfectant before
every bath.
Take medicine like
ibuprofen to relieve pain.
Use sietz baths a few
times a day after 24 hours
Change pads every 2 to
4 hours.
Keep the area around
the stitches clean and
dry. Pat the area dry
with a clean towel after
bath.
30DR MUKHERJEE ALKA NAGPUR