Presenting diameters
•Télécharger en tant que PPT, PDF•
148 j'aime•79,687 vues

Presenting diameters of foetal head and how does it affect the labour process. Also the outcomes and few management options are included too.

Recommandé
Contenu connexe
Tendances
Tendances (20)
Similaire à Presenting diameters
Similaire à Presenting diameters (20)
Dernier
Dernier (20)
Presenting diameters
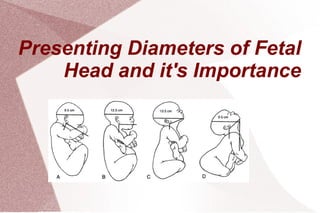
- 1. Presenting Diameters of Fetal Head and it's Importance
- 2. Anatomy of Fetal Skull
- 3. Fetal cranium made of 5 bones- 2 parietal bones / 2 frontal bones and the occipital bone These are held together by membranous structures called sutures- permit movements of bones during labour There are 4 prominent sutures 1. Coronal suture : separates frontal bones from parietal bones 2. Sagittal suture : separates two parietal bones 3. Lamboid suture : separates occipital bone from parietal bones 4. Frontal suture : separates two frontal bones.
- 4. Fontanelle : When two or more sutures meet, there is an irregular membranous part between them called fontanelle There are two important fontanelles 1. Anterior fontanelle ( bregma ) : Diamond shaped area at the junction of coronal and sagittal sutures. AP/transverse diameter 3 cm. Fused around ~18 months 2. Posterior fontanelle ( lambda ) : Small triangular area at the junction of sagittal and lamboid sutures (closes 2-3 months after birth )
- 6. Regions of Fetal Head Occiput : The bony prominence that lies behind posterior fontanelle Vertex : Diamond shaped area between anterior and posterior fontanelle Sinciput : Area in front of anterior fontanelle. Includes forehead. Brow – between bregma and root of nose lying below root of nose and supra orbital bridges
- 8. Diameters of Fetal Head Five important diameters. 1. Suboccipito-bregmatic diameter 2. Suboccipitofrontal diameter 3. Occipitofrontal diameter 4. Mentovertical diameter 5. submentobregmatic diameter
- 9. Suboccipito-bregmatic diameter The diameter is from suboccipital region to centre of the bregma. Diameter = 9.5 cm Fetal head circumference is smallest (32 cm ) Head well flexed Flexed vertex presentation
- 10. Suboccipito-frontal diameter Diameter calculated from prominence at mid frontal bone to the under-surface of the occipital bone where it joins neck The diameter is 10.5 cm Vertex is partially deflexed. Results in occipito-posterior position.
- 11. Occipito-frontal diameter Diameter extends from the prominent point of mid-frontal bone to the most prominent point of occipital bone The diameter = 11.5 cm Fetal head circumference ~ 34.5 cm Vertex is deflexed Associated with Direct occipito- posterior position.
- 12. Occipito-posterior position It is a vertex presentation in which the occiput is placed posteriorly . It can be:- 1.Right occipto-posterior (the commonest) 2.Left occipto-posterior. 3.Direct occipto-posterior Associated diameters are 1. Suboccipito frontal diameter 2. Occipitofrontal diameter
- 13. Incidence :Incidence : In 20% of cases the occiput is posterior at the beginning of labour . Causes :-Causes :- 1. Pelvic Factors:- 50% of cases are associated with anthropoid pelvis or android pelvis . 2.Fetal Factors:- Marked deflection of the fetal head due to high pelvic inclination or anterior wall placenta . 3.Uterine Factor:- Abnormal uterine contraction which may be the cause or effect .
- 14. DiagnosisDiagnosis Abdominal Examination Features suggesting the diagnosis include -backache during labour. -flattening of the abdomen below the umbilicus . -the fetal limbs are more easily felt near the midline on both sides. -The head not engaged and feels larger than usual
- 15. Problems associated with Occiput Posterior – -the head faces the front of the mother's pelvis instead of turning toward the mother's back. -delivered with the head facing the ceiling,which is often a more difficult way to deliver. vaginal examination -Elongated bag of membrane which is likely to rupture early . -High deflexed head with the anterior fontanelle in the centre of the pelvis .
- 16. - A large episiotomy may be required. - OP may lead to dysfunctional labour (in primigravida). - Contraction may be painful and accompanied by backache Mechanism of Labour in OP position First and second stage of labour usually prolonged . -membrane usually rupture early with the hazards of cord prolapse and infection . -In favorable circumstances (90% of cases) good uterine contraction result in good flexion of the head and the occipt rotates 3/8 of the circle (135c0 ) anteriorly and deliver as occipito-anterior position .
- 17. In unfavorable circumstances (10% of cases) the occiput 1. Fail to rotate and remain in the oblique diameter of the pelvis . 2. Rotate anteriorly 1/8th of circle (short rotation) and the head become arrested in the transverse diameter of the pelvis (deep transverse arrest) . 3. Rotate posterioly 1/8th of the circle to lie on the sacral hollow this called direct-occipto- posterior position . And if the fetus is small & pelvis is Adequate spontenous delivery can occur as face to pubic.
- 18. ManagementManagement - Unless there is fetal hypoxia or other complication labour is allowed to proceed with the following special instructions . -Provide adequate analgesia (an epidural is ideal). -Prevent dehydration with intravenous fluid. -You may need to promote uterine contraction with oxytocin . -Good monitoring for progress of labour ,fetal condition and maternal condition .
- 19. - In the majority of cases anterior rotation of the occipt is completed and the baby is delivered as occipto-anterior. - In direct occipto-posterior delivery as face to pubis may occur ,The perineum should be protected by a generous episiotomy. Persistent –occipto posterior and deep transverse arrest . - If the fetal head is not engaged caesarian section is the treatment of choice . - If the fetal head is engaged the treatment will be one of the following .
- 20. 1) Manual rotation and delivery by forceps as occipto-anterior . 2) Rotation to occipto-anterior and extraction using kielland’s forceps . 3) Ventouse (vacuum extraction). 4) Caesarean section if the above lines of treatment fail or there is other complicating factor . 5) Craniotomy when the fetus is dead .
- 21. Mento-vertical diameter Diameter extending from the chin to furthest point of vertex. Measures 13cm Largest antero-posterior diameter Head is partially extended. Associated with brow presentation
- 22. Brow presentation Incidence: ranges from 1:1000 to 1:3500 Rarest malpresentation The presenting diameter 13.5cm (mento-vertical ) Incompatible with vaginal delivery Causes Prematurity Multiple pregnancies Goiter or hygroma
- 23. DiagnosisDiagnosis Abdominal examination- suspect if both chin and occiput are palpable head doesn't descend below ischeal spines Vaginal examination Palpate supra orbital ridges/nose, anterior fontanelle. Cant palpate chin.
- 24. ManagementManagement Watch and wait : may become face or vertex presentation If progress is slow or the brow persists caesarian section
- 25. Submento-bregmatic diameter The diameter extending from just behind chin to the centre of bregma Measures 9.5cm Head is fully extended Associated with face presentation
- 26. Face presentation Incidence : 1:600- 1:1500 Due to hyper-extension of fetal head Presenting diameter 9.5 cm (submento-bregmatic diameter ) Engagement of fetal head late Progression of labour slow Probably due to lack of molding of facial bones
- 27. CausesCauses Fetal anomalies. The most common anomaly that causes face presentation is anencephaly. Anencephalic babies present face first because of the faulty development of the cranium. Tumors on the neck or back may also cause extension of the head. Pelvic contractures or android pelvis. This is the major factor. It accounts for about 40% of face presentations. Fetopelvic disproportion Multiparity
- 28. Preterm birth Polyhydramnios. When the membranes rupture the rush of fluid may cause the head to extend as it descends. Coils of umbilical cord around the neck. DiagnosisDiagnosis Vaginal examination The orbital ridges/nose/malar eminences/ mentum/ mouth and gums
- 29. Management In the chin-anteriorchin-anterior position prolonged labor is common. Descent and delivery of the head by flexion may occur. In the chin-posteriorchin-posterior position, however, the fully extended head is blocked by the sacrum. This prevents descent and labour is arrested.
- 30. Management Chin-Anterior PositionChin-Anterior Position If the cervix is fully dilated: Allow to proceed with normal childbirth; If there is slow progress and no sign of obstruction, augment labor with oxytocin; If descent is unsatisfactory, deliver by forceps. If the cervix is not fully dilated and there are no signs of obstruction: augment labor with oxytocin. Chin-Posterior PositionChin-Posterior Position If the cervix is fully dilated: Deliver by caesarean section. If the cervix is not fully dilated Monitor descent, rotation and progress. If there are signs of obstruction, deliver by caesarean section. *Do not perform vacuumDo not perform vacuum extraction for faceextraction for face presentation.presentation.
- 31. Thank You!!