Nephrotic syndrome (Primary glomerulonephrosis)
•
2 j'aime•714 vues

Nephrotic syndrome happens when damage to your kidneys causes these organs to release too much protein into your urine. Nephrotic syndrome isn’t itself a disease. Diseases that damage blood vessels in your kidneys cause this syndrome. Nephrotic syndrome is characterized by the following: A high amount of protein present in the urine (proteinuria) high cholesterol and triglyceride levels in the blood (hyperlipidemia) Low levels of a protein called albumin in the blood (hypoalbuminemia) Swelling (edema), particularly in your ankles and feet, and around your eyes.

Recommandé
Contenu connexe
Tendances
Tendances (20)
Similaire à Nephrotic syndrome (Primary glomerulonephrosis)
Similaire à Nephrotic syndrome (Primary glomerulonephrosis) (20)
Plus de kalyan kumar
Plus de kalyan kumar (20)
Dernier
Dernier (20)
Nephrotic syndrome (Primary glomerulonephrosis)
- 1. NEPHROTIC SYNDROME Presented by Mr B.Kalyan kumar M.Sc (N)
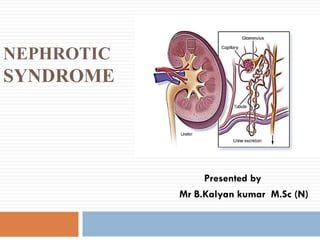
- 2. Introduction ⌛ The nephron (from Greek nephros, meaning "kidney") is the microscopic structural and functional unit of the kidney. ⌛ It is composed of a renal corpuscle and a renal tubule. ⌛ The renal corpuscle consists of a tuft of capillaries called a glomerulus and an encompassing Bowman's capsule. ⌛ The glomerulus is responsible for the initial stage of urine formation and the filtration rate depends upon the intact glomerular membrane
- 3. ⌛ Nephrotic syndrome is the common cause of hospitalization in children. ⌛ Nephrotic syndrome is a condition that causes the kidneys to leak large amounts of protein into the urine. ⌛ This can lead to a range of problems, including swelling of body tissues and a greater chance of catching infections.
- 4. Definitions Nephrotic syndrome is a clinical state that includes massive proteinuria, hypoalbuminemia, hyperlipidemia, and edema. The disorder is characterized by increased glomerular permeability to plasma protein which results in massive urinary protein loss. -Parul dutta
- 5. Nephrotic syndrome is a collection of symptoms due to kidney damage. This includes protein in the urine, low blood albumin levels, high blood lipids, and significant swelling. -Wikipedia
- 6. Incidence Incidence of condition is 2 to 7 per 1000 children. It is more common in male child. Mean age of occurrence is 2 to 5 years
- 7. Classification It can be classified as : ❑ Congenital ❑ Idiopathic or Primary Nephrotic Syndrome ❑ Secondary
- 8. Congenital Nephrotic Syndrome It is rare but a serious and fatal problem usually associated with other congenital anomalies of kidney. It is inherited as an autosomal recessive Several renal insufficiency and urinary infections along with this condition results in poor prognosis.
- 9. Primary or Idiopathic Nephrotic Syndrome Primary nephrotic syndrome is also known as idiopathic nephrosis, childhood nephrosis or minimal change nephrotic syndrome (MCNS). It is the most common type (aband regarded as autoimmune phenomenonout 90%),and regarded as autoimmune phenomenon, as it responds to suppressive therapy.
- 10. It occurs in about 10 % of all cases. This condition may occur due to some form of chronic glomerulonephritis or due to some form of chronic glomerulonephritis ,or due to diabetes mellitus ,malaria, malignant hypertension ,hepatitis ‘B’ , infective endocarditis, HIV /AIDS, drug toxicity ,lymphomas, syphilis, etc. Secondary Nephrotic Syndrome
- 11. Causes Nephrotic syndrome is usually caused by damage to the clusters of tiny blood vessels (glomeruli) of your kidneys. The glomeruli filter your blood as it passes through your kidneys, autosomal recessive disease. Several separating things your body needs from those it doesn't. Healthy glomeruli keep blood protein (mainly albumin) — which is needed to maintain the right amount of fluid in your body — from seeping into your urine
- 12. When damaged, glomeruli allow too much blood protein to leave your body, leading to nephrotic syndrome.
- 13. Etiology of Nephrotic Syndrome There are many possible causes for Nephrotic Syndrome. Many diseases and conditions can cause glomerular damage and lead to nephrotic syndrome, including:
- 14. Minimal change disease: The most common cause of nephrotic syndrome in children, this disorder results in abnormal kidney function, but when the kidney tissue is examined under a microscope, it appears normal or nearly normal. The cause of the abnormal function typically can't be determined
- 15. Characterized by scattered scarring of some of the glomeruli, this condition may result from another disease or a genetic defect or occur for no known reason. Focal segmental glomerulosclerosis:
- 16. Membranous nephropathy: This kidney disorder is the result of thickening membranes within the glomeruli. The exact cause of the thickening isn't known, but it's sometimes associated with other medical conditions, such as hepatitis B, malaria, lupus and cancer.
- 17. Diabetic kidney disease: Diabetes can lead to kidney damage (diabetic nephropathy) that affects the glomeruli. Systemic lupus erythematosus: This chronic inflammatory disease can lead to serious kidney damage.
- 18. Amyloidosis: This disorder occurs when substances called amyloid proteins accumulate in your organs. Amyloid buildup often affects the kidney. Blood clot in a kidney vein: Renal vein thrombosis, which occurs when a blood clot blocks a vein connected to the kidney, can cause nephrotic syndrome.
- 19. Heart failure: Some forms of heart failure, such as constrictive pericarditis and severe right heart failure, can cause nephrotic syndrome.
- 20. Clinical Manifestations Periorbital puffiness. Edema (minimal or massive) Profound weight gain(within a short period of days or week is found). Dependent edema develops (ankle, feet, genitalia, scrotum) the edematous part is soft and pits easily on pressure.
- 21. Striae may appear on the skin due to overstretching by edema. Fluid accumulates in the body space, resulting in ascites, pleural effusion with respiratory distress and generalized edema (anasarca) Urine output is reduced and becomes concentrated with frothy appearance. GI disturbance is also found as vomiting, loss of appetite and diarrhea.
- 22. Other features include: ◊ Fatigue ◊ lethargy, ◊ Pallor ◊ Irritability. ◊ Hypertension ◊ Hematuria ◊ Hepatomegaly and wasting of muscle may found in some cases.
- 23. Diagnostic Evaluation History of illness and physical examination hlp to diagnose the condition clinically. Urine examination shows gross proteinuria(2 to 20 gm/day),presence of cast, slight hematuria and increased specific gravity. Blood examination demonstrates reduced total protein albumin less than 2.5 gm/dl and cholesterol more than 200mg/dl.
- 24. Lipoproteins and BUN (Blood Urea Nitrogen) are increased. Serum albumin and globulin ratio is reversed. There is hypogammaglobuminemia, hypomagnesia, and low – creatinine level. Renal biopsy is indicated in case of poor response to steroid therapy. Other investigation show low ASO titre and IgM raised IgG and IgE ,serum raised IgG and IgE ,serum.
- 25. Management Bed rest and high protein diet with restriction of fluid intake are important aspects of management. Steroid therapy with oral prednisolone is the most significant aspect of management of nephrotic syndrome. It is given 2 mg/kg/day in 2 to 3 divided doses for at least 4 to 6 weeks and then gradually tapered off or abruptly doses for at least 4 to 6 weeks and then gradually tapered off or abruptly stopped after another 4 to 6 weeks. Antacid is given along with prednisolone to prevent gastric complications.
- 26. Antibiotic therapy is indicated in the presence of any infection Diuretics are prescribed in the presence of severe edema and massive ascites. Frusemide 1 mg/kg/day in 2 divided dosed alone or with spironolactone 2-3 mg/kg/day in two divided doses is given. Potassium supplementation is given along with diuretics.
- 27. Albumin infusion (1gm/kg/day) maybe given in case of massive edema and ascites. It helps to shift the fluid from interstitial space into the vascular system Diuretic therapy is given in combination of albumin infusion. Plasma or blood transfusion may be given in some cases to treat hypoalbuminemia. Renal transplantation is indicated in end stage renal failure due to steroid Resistant glomerulosclerosis.
- 28. Immunosuppressive drugs (Levamisole, methotrexate, cyclophospham, cyclosporine, chlorambucil ) may be administered along with prednisolone in case of frequent (4 or more per year) relapses and in steroid dependent cases.
- 29. Nursing Management Continuous monitoring of fluid retention or excretion. Strict intake and output records Urine examination of albumin. Daily weight check and measurement of abdominal girth. Assessment of edema, the degree of pitting, and the colour and texture of the skin. Vital signs are monitored for early signs of complications such as shock or an infective process.
- 30. The children are particularly prone to infections and thus they should be kept warm and dry, active and away from infected persons. Salt is usually restricted during the edema phase and while child in on steroid therapy. Fluid restriction is limited to short term use during massive edema. Suitable recreational and diversional therapies are an important part in their care. Continuous support of the child and the family are important consideration in nursing care.
- 31. Complications ■ Ascites ■ Pleural effusion ■ Generalized edema ■ Coagulation disorders ■ Thrombosis ■ Recurrent infection of different system ■ Renal failure. ■ Growth retardation ■ Calcium and vitamin D deficiency ■ Protein energy malnutrition ■ Relapse of Nephrotic Syndrome
- 32. Prognosis ❖ The prognosis for ultimate recovery is good. ❖ It is self-limiting disease, and in children who respond to steroid therapy, the tendency to relapse decrease with time. ❖ With early detection and prompt implementation of therapy to eradicate proteinuria, progressive basement membrane damage is minimized so that when the tendency to relapse is past, renal function is usually normal or near normal. ❖ It is estimated that approximately 80% of affected children have this favorable prognosis.