ECTOPIC PREGNANCY
•Télécharger en tant que PPTX, PDF•
64 j'aime•6,973 vues

DIWAN SHRESTHA (D1) presentation on ECTOPIC PREGNANCY

Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
En vedette (20)
Similaire à ECTOPIC PREGNANCY
Similaire à ECTOPIC PREGNANCY (20)
Dernier
Dernier (20)
ECTOPIC PREGNANCY
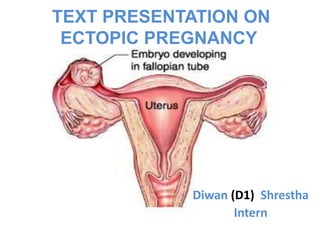
- 1. TEXT PRESENTATION ON ECTOPIC PREGNANCY Diwan (D1) Shrestha Intern
- 2. Ectopic Pregnancy Definition Any pregnancy where the fertilised ovum gets implanted & develops in a site other than the normal endometrial cavity.
- 3. Incidence Accounts for 1-2 % of total pregnancy Rising due to PID, use of IUCD, tubal surgeries, ART & STIs Recurrence rate – 15% after 1st, 25% after 2 ectopics
- 4. Sites for ectopic pregnancy
- 6. Risk Factors of Ectopic Pregnancy Up to half of women with ectopic pregnancy will have no identifiable risk factors. • History of prior tubal surgery including tubal ligation • Prior ectopic pregnancy • In utero diethylstilbestrol (DES) exposure • History of PID • IUD use • Perimenopausal women • Infertility • Smoking • Multiple sexual partners • Endometriosis
- 8. Clinical Features Wide spectrum of clinical presentation from asymptomatic pt to others with acute abdomen & hemodynamic shock. The classic symptom triad of it is pain, amenorrhea & vaginal bleeding. - Pain May be unilateral / bilateral & may occur in upper or lower abdomen dull, sharp or crampy continuous or intermittent With rupture transient relief of pain may occur. Feeling of nausea, vomiting, fainting attack, syncope attack due to reflex vasomotor disturbance may be present
- 9. Clinical Features Contd.. - Physical examination Should include vital signs & examination of abdomen & pelvis The abdomen may be non tender or mildly tender with or without rebound Uterus may be slightly enlarged Cervical motion tenderness may or may not be present An adnexal mass may be palpable in up to 50% cases but the mass varies markedly in size, consistency & tenderness
- 10. Clinical Features Contd.. -With rupture & intra abdominal hemorrhage, patient develops tachycardia followed by hypotension Bowel sounds are decreased or absent Abdomen is distended with marked tenderness & rebound tenderness Cervical motion tenderness is present.
- 11. Investigation Accuracy of initial clinical evaluation is less than 50%. Additional tests are frequently required to differentiate early viable intrauterine pregnancy or suspected ectopic or abnormal intrauterine pregnancy General investigation such as Hb, blood grouping & cross matching, TC, DC, BT, CT
- 12. Investigation contd. Bed side test : 1.Urine pregnancy test : positive in 95% cases 2.Culdocentesis: It can be done with 18-20G spinal needle through posterior fornix into POD. If non clotting blood is obtained, results are positive.If serous fluid is present,results are negative A lac of fluid return or clotted blood is non- diagnostic
- 13. Investigation Contd:Other invest as 1) Ultrasonography: Transvaginal USG is superior to transabdominal USG Evidence of an empty uterus, detection of adnexal masses , free peritoneal fluid & signs of ectopic pregnancy are more reliably established with transvaginal procedure Identification of double decidual sac sign is the best method to differentiate true sacs from pseudosacs Presence of free cul-de-sac fluid is frequently associated with ectopic pregnancy TVS can detect gestational sac at 4 weeks & by TAS at 6 wks
- 14. # USG PICTURE Bagel sign – Hyperechoic ring around gestational sac in adnexal region Hyperechoic Hyperechoic ring around gestational gestational in adnexal region Investigation Contd
- 15. Investigation Contd: 2)Color Doppler Sonography : It improve the accuracy & identify the placental shape (ring of fire pattern) & blood flow outside the uterine cavity
- 16. Investigation contd 3)Quantitative B-hCG : • -Diagnostic cornerstone for ectopic pregnancy • -The hCG enzyme immunoassay is positive in virtually all documented ectopic pregnancies • -When hCG level < 2000IU/Ldoubling time helps to predict viable Vs non viable pregnancy • -Rise of B-hCG < 66% in 48 hrs indictate ectopics or nonviable intrauterine pregnancy
- 17. Investigation Contd: 4)Laparoscopy: Gold standard for the diagnosis of ectopic pregnancy Diagnosis & removal of ectopic mass can be done at the same time
- 18. Investigation Contd: 5)Dilatation & Curettage: It is performed when the pregnancy is confirmed to be nonviable & location of pregnancy cannot be confirmed by USG Identification of decidua without chorionic villi is suggestive of extra uterine pregnancy
- 19. Investigation Contd: 6) Other tests a)Estradiol: Levels are significantly lower in ectopic pregnancies when compared with viable pregnancies b)Relaxin: is a protein hormone produced solely by corpus luteum of pregnancy & its levels are significantly lower in ectopic pregnancies. c)Maternal AFP: levels are elevated in ectopic pregnancies d)Serum progesterone: With ectopicpregnancies is lower than 25 ng/mL .
- 20. Management Of Ectopic Pregnancy Management may be medical or surgical or expectant Management approach depends on clinical circumstances, site of ectopic pregnancy & the available resources 1.Surgical treatment : •It can be accomplished by laparoscopy or laparotomy •The hemodynamic stability of patient, size & location of ectopic mass & surgeons expertise all contribute to determining the appropriate surgical approach
- 21. Surgical management: Contd Laparotomy: Indicated when the patient becomes hemodynamically unstable & an expedited abdominal entry is required Advantages of laparoscopy: decreased cost, operative time ,blood loss & hospital stay An alternative to laparoscopy is the use of minilaparotomy incision.
- 22. Surgical management: contd There is debate about which surgical procedure (Salpingectomy or Salpingostomy) is best. The decision to choose one technique over the other depends on the condition of the affected & contralateral fallopian tubes, history of previous ectopic in the affected tube & patients desire for future fertility Linear salpingostomy: Can be considered when the patient has an unruptured ectopic pregnancy, wishes to retain her potential for future fertility & the affected fallopian tube appears otherwise normal If the contralateral tube appears damaged , a salpingostomy should be considered
- 23. Surgical management: Contd In salpingostomy the products of conception are removed through an incision made into the tube on its antimesenteric border Contraindications Of salpingostomy: Ruptured fallopian tube use of extensive cautery to obtain hemostasis severely damaged tube recurrent ectopic pregnancy in the same tube.
- 24. Mx Of Ectopic Pregnancy: Contd 2. Medical Treatment: The drug most frequently used for medical management of ectopic pregnancy is methotrexate Other agents such as KCL, hyperosmolar glucose, prostaglandins are not recommended because their safety & accuracy are not well documented These agents may be given systemically ( IV, IM or orally ) or locally (laparoscopic direct injection or retrograde salpingography ).
- 25. Medical Treatment Contd: Methotrexate: It is a folic acid analogue that inhibits dehydrofolate reductase & thereby prevents synthesis of DNA Candidates for Methotrexate – patients with confirmed or high suspicion for ectopic pregnancy who are hemodynamically stable with no evidence of rupture Contraindications: hemodynamically unstable ruptured ectopic pregnancy unable to comply with medical management follow up Breastfeeding Immunodeficiency preexisting blood dyscrasias active pulmonary disease
- 26. Medical Treatment Contd: Methotrexate treatment regimens – 1.Multidose regimen – MTX 1mg/kg IM on 1,3,5,7 days Leucovorin 0.1mg/kg on 2,4,6,8 days Measure B-hCG levels on days 1,3,5,7 until 15% decrease between 2 measurement Once B-hCG level drops 15%, stop MTX & monitor B-hCG weekly until non pregnant level
- 27. Medical Treatment Contd: 2.Single dose regimen: MTX 50mg/m2 on day 0 Measure B-hCG level on days 4 & 7 If level drops by 15%, monitor B-hCG weekly until non pregnant level. If levels do not drop by 15%, repeat dose of MTX & measure B-hCG on days 4 & 7 3.Two dose regimen: MTX 50mg/m2 on days 0 & 4 Measure B-hCG levels on days 4 & 7 If levels drop by 15%, monitor B-hCG weekly until non pregnant level If level do not drop by 15%, repeat dose of MTX on days 7 & 11 & measure B-hCG on days 7 & 11. If levels drop 15%, monitor B-hCG level weekly until non pregnant level
- 28. Medical Treatment Contd: Effectiveness of Methotrexate The overall effectiveness of MTX therapy ranges from 78 to 96%. Side effects: Dose & frequency dependent nausea, vomiting Stomatitis abdominal pain bone marrow suppression Alopecia dermatitis & pneumonitis.. • The risk of subsequent ectopic pregnancy is about 10% following either methotrexate or salpingostomy. Comparision of laparoscopically treated & methotrexate treated patients shows 2 methods have similar reproductive outcomes
- 29. Mx of ectopic pregnancy: Contd 3.Expectant management: # Identification criteria : 1.Tubal ectopic pregnancies only 2.Haemodynamically stable 3.Haemoperitoneum < 50 ml 4.Adnexal mass of < 3.5cm without heart beat 5.Initial B-hCG < 1000 IU/L & falling in titre * Success rate – up to 60 %
- 30. Expectant Mx: Contd # Protocol Hospitalisation with strict monitoring of clinical symptom Daily Hb estimation Serum B-hCG monitoring 3-4 days until it is <10 IU/L TVS to be done twice a week #Spontaneous resolution occurs in 72%, while 28% will need laparoscopic salpingostomy
- 31. Management of ruptured ectopic PRINCIPLE: Resuscitation & Laparotomy ANTI SHOCK TREATMENT: - IV line opened, crystalloid started - Folleys catheterization done - colloids for volume replacement LAPAROTOMY: - Rapid exploration of abdominal cavity done - Salpingectomy is the definitive surgery - Blood transfusion done
- 32. Cervical Ectopic • Clinical criteria for diagnosing cervical ectopic: Uterus smaller than the surrounding distended cervix External os may be open Visible cervical lesion often blue or purple in colour Profuse bleeding on manipulation of cervix Management Medical treatment with methotrexate & surgical dilation & curettage Ideal regimen for medical Mx is unknown & success is reported with both single & multidose regimens as previously described
- 33. Ovarian ectopic A pregnancy confined to ovary accounts for up to 3% of all ectopic pregnancies. • Criteria for ovarian pregnancy diagnosis: 1.The fallopian tube on the affected side must be intact 2.The fetal sac must occupy the position of the ovary 3.The ovary must be connected to the uterus by the ovarian ligament 4.Ovarian tissue must be located in the sac wall Treatment: Ovarian cystectomy &/or wedge resection Successful treatment with Methotrexate is reported
- 34. Abdominal ectopic pregnancy • It can be classified 1. Primary 2. Secondary #Studdifords criteria for diagnosis of primary abdominal pregnancy are - Presence of normal tubes & ovaries with no evidence of recent or past pregnancy No evidence of uteroplacental fistula The presence of a pregnancy related exclusively to the peritoneal surface & early enough to eliminate the possibility of secondary implantation after primary tubal nidation # Secondary – conceptus escapes out through a rent from primary site – Intraperitoneal or Extraperitoneal broad ligament Surgical intervention is recommended when an abdominal pregnancy is diagnosed It can be treated with Methotrexate in patients not considered to be optimal surgical candidates.
- 35. THANK YOU