
Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
En vedette (15)
Similaire à Nutrition in surgery
Similaire à Nutrition in surgery (20)
Dernier
Dernier (20)
Nutrition in surgery
- 1. N U T R I T I O N A L A S S E S M E N T A N D M A N A G E M E N T I N S U R G I C A L P A T I E N T S B Y : D A W I T ( M D , G S R 1 ) M O D E R A T O R : D R . D A W I T T ( C O N S U L T A N T S U R G E O N ) J I M M A S P E C I A L I Z E D H O S P I T A L 12/21/2015 1
- 2. Outline 12/21/2015 2 Introduction Nutritional assessment in surgical patients Nutritional requirments and interventions Nutrition in specific disease conditions Summary and recommendations
- 3. Objectives 12/21/2015 3 To elaborate causes and consequences of malnutrition in the surgical patient To clarify objective nutritional assessment methods To discuss on the different methods of providing nutritional support and their complications
- 4. Introduction 12/21/2015 4 Health is strongly influenced by nutritional status Rates up to 50 percent in certain populations 1936=33% vs 3.5%(mortality) Identification Minimizes unwanted outcome in surgery
- 5. Consequence of malnutrition in surgical patients 12/21/2015 5 Increase susceptibility to infection Poor wound healing Increase frequency of decubitus ulcer Over growth of bacteria in GIT Abnormal nutrient losses through the stool
- 6. Factors Affecting Nutritional Intake during Illness 12/21/2015 6 Medications our role ???? Fear and Anxiety Pain Inappropriate Diet Orders
- 7. ASSESSMENT OF NUTRITIONAL STATUS 12/21/2015 7 The possibility of malnutrition should form part of the work up of all patients A clinical assessment of nutritional status involves: Focused Hx Focused P/E Focused Ixs
- 8. Nutritional ass’t…cont’d 12/21/2015 8 1. Clinical History History of poor nutrient intake Loss of body weight Social & economic condition that may lead to poverty & malnutrition Gastrointestinal symptoms Other chronic medical illnesses
- 9. Nutritional ass’t…cont’d 12/21/2015 9 2. Physical Examination G/A V/S Anthropometry Body Mass Index
- 10. CONT’D 12/21/2015 10 BMI INTERPRETATION <18.5 underweight 18.5-24.9 normal 25-29.9 Over wt 30-34.9 Obesity GI 35-39.9 Obesity GII >/= 40 Extreme obesity GIII
- 11. HEENT 12/21/2015 11 Signs deficiencies Alopecia, Easily plukablity PEM Angular palebritis Vit B2 Bitot’s spots,conjuctival xerosis Vit A Angular stomatitis Vit B2,6,12 Bleeding gum Vit C
- 12. Cont’d 12/21/2015 12 Cardiovascular: Evidence of heart failure or high- output state Neck: Thyromegaly Extremities: Edema, muscle wasting Skin: Ecchymoses, petechiae, pallor, pressure ulcers, assessment of surgical wound healing and signs of wound infection (if postoperative). Neurologic: Evidence of peripheral neuropathy, reflexes, tetany, mental status
- 13. Nutritional ass’t…cont’d 12/21/2015 13 3. Laboratory Investiaton To detect subclinical nutritional deficiencies • Nitrogen Balance • Serum Albumin • Creatinine excretion • Immunological function assessment(TLS)
- 14. Nitrogen balance 12/21/2015 14 Provides an index of protein gain/loss 1 g protein =6.25 g nitrogen Nitrogen intake – loss{90%urine,intugumentary 5%,5% stool} overall protein status effectiveness of a nutrition intervention Serum albumin fall during acute stress b/c of Increase incirculating extravascular volume TNF alpha mediated inhibition of synthesis
- 15. Cont’d 12/21/2015 15 Serum albumin most abundant liver = t1/2, 18-20 days =2.2 g/dl marker of –ve catabolic state Serum transferrin =t1/2, 8-9 days 215–380 mg/dL Serum prealbumin(transthyretin)=t1/2, 2-3 days. 19 to 43 mg/dL Retinol binding protien
- 16. Creatinine excration 12/21/2015 16 Metabolic product of skeletal muscle Produced constantly indirect proportion to skeletal mass 1g creatinine=18.5 fat free skeletal muscle CHI 24-hour urine creatinine (mg) expected 24-hour urine creatinine (cm)
- 17. TOTAL ENERGY EXEDITURE 12/21/2015 17 Definition BEE 60% of TEE Basal energy requirement is the function of the individual's weight,height, age, gender, activity level and the disease process
- 18. Basal energy expenditure (BEE) 12/21/2015 18 Estimated using the Harris-Benedict equations: BEE(men)=66.47+13.75(W)+5(H)-6.67(A) BEE(women)=655.1+9.56(W)+1.85(H)- 4.68(A) where W = weight in kilograms; H = height in centimeters; and A = age in years.
- 19. Cont’d 12/21/2015 19 It will be adjusted in stress conditions Total calories=BEE X stress factor X activity factor Activity factor=1.2 in bed rest =1.3 out of bed conditions Kcal/kg/day Above BEE Normal 25-30 1.1 Mild stress 25-30 1.2 Moderate stress 30 1.4 Sever stress 30-35 1.6 burns 35-40 2
- 20. ENERGY REQUIRMENT….cont’d 12/21/2015 20 Rest Energy Expenditure Adults (18-65)………………….. 20-30 kcal/kg Elderly (65+)……………………. 25 kcal/kg For burns Patients…………….. 30-35kcal/kg Other factors: Pregnancy………………………..Add 300 kcal/day Lactation………………………… Add 500 kcal/day Obese or Super obese……… 15-20 kcal/kg
- 21. ENERGY REQUIRMENT….cont’d 12/21/2015 21Stress Factors • Peritonitis……………………+ 15% • soft tissue traum ………..+ 15% • Fracture……………………..+ 20% • fever (per oC rise)……….+ 13% • Moderate infection………..+ 20% • Severe infection ……………+ 40% • <20% BSA Burns…………..+ 50% • 20-40% BSA Burns…………+ 80% • >40% BSA Burns……………+ 100%
- 22. NUTRITIONAL REQUIREMENTS…cont’d 12/21/2015 22FAT Requirement =3 g/kg/day 30-40 percent of nutrition Liver can synthesize most fatty acids, but humans lack the desaturase enzyme needed to produce n-3 and n-6 fatty acid series Therefore linoleic acid should constitute at least 2% and linolenic acid at least 0.5% of daily caloric intake to prevent essential fatty acid deficiency
- 23. NUTRITIONAL REQUIREMENTS…cont’d 12/21/2015 23CARBOHYDRATE 40-50 percent of total nutrition PROTEIN The basic requirement for nitrogen 0.10–0.15 g/kg per day Additional protein burn injuries, open wounds, protein losing Enteropathy / Nephropathy A lower protein intake may be necessary in patient with chronic renal insufficiency who are not treated by dialysis and certain patients with hepatic encephalopathy
- 24. NUTRITIONAL REQUIREMENTS, PROTEIN…cont’d 12/21/2015 24 Clinical condition requirement normal 0.8 Metabolic stress (illness, injury) 1.0-1.5 Acute renal failure (undialyzed) 0.8-1.0 hemodialysis 1.2-1.4 Peritoneal dialysis 1.3-1.5
- 25. NUTRITIONAL INTERVATION 12/21/2015 25 Goal To alter the course and outcome of critical illness To supply the substrate necessary to meet the metabolic needs of patients in who adequate nourishment cannot be provided by mouth
- 26. Indications for nutritional intervention 12/21/2015 26 General indication pre existing nutritional deprivation Anticipated/actual inadequate energy intake
- 27. Specific Indications for nutritional intervention 12/21/2015 27 Inadequate intake for 5-7 days or anticipated no intake for the same period Serum albumin less than 3gm/dl Weight loss of greater than 10% body wt in 6months. Current wt less than 80% of the ideal wt Anticipated severe insult to the body Concurrent medical problem
- 28. ARTIFICIAL NUTRITIONAL SUPPORT 12/21/2015 28 Nutritional support, via either enteral or parenteral routes, is used in three main settings: To provide adequate nutritional intake during recuperative phase of illness or injury to support the pts during systemic response to inflammation, injury or infection during an extended critical illness pts with permanent loss of intestinal length or function
- 29. 12/21/2015 29
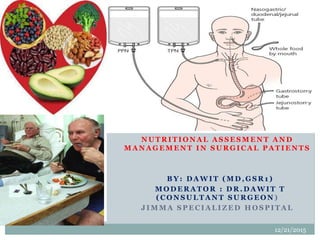
- 30. ENTERAL FEEDING 12/21/2015 30 Delivery of nutrients into the gastrointestinal tract This can be achieved with oral supplements (sip feeding) or variety of tube-feeding techniques (NG, ND,NJ tubes) Surgical techniques Percutaneous endoscopic gastrostomy (PEG) Surgical gastrostomy Percutaneous endoscopic Jejunostomy (PEJ) Surgical Jejunostomy A variety of nutrient formulations are available for enteral feeding
- 31. ENTERAL FEEDING...cont’d 12/21/2015 31 Long term feeding (>6 wk) usually requires gastrostomy or jejunostomy tube Enteral feeding is often required in pts with anorexia, impaired swallowing, or bowel disease Enteral formulas: standard (osmolality- 300) and modified
- 32. ENTERAL FEEDING....CONT’D 12/21/2015 32 Why Preferable? Physiologic & matabolic benefits Immunologic function Cost benefits Safety benefits Fewer infectious complicationsa 44% reduction in infectious complications Less hyperglycemia → neutrophil inhibition
- 33. Contraindications 12/21/2015 33 Short bowel syndrome Bowel obstruction GI bleeding Protracted vomiting & diarrhea Fistulas, Ileus GI ischemia Gastroparesis, GOO Repeated aspiration(reflux)
- 34. Complications 12/21/2015 34 Tube related malposition Blockage Aspiration Local complication mainly aspiration pneumonia and diarrhoea
- 35. Delivery Methods 12/21/2015 35 Sip feeding Commercially available supplementary sip feeds are used in patients who can drink but whose appetites are impaired Nasogastric tube less expensive, easier to secure and maintain Diabetics and patients with severe head injuries may have profound gastroparesis
- 36. Contraindications to NGT 12/21/2015 36 delayed gastric emptying Gastric residuals of 200 mL or more in a 4- to 6-hour period gastric outlet obstruction a history of repeated aspiration due to reflux inability to protect the airway (a relative contraindication to gastric feeding)
- 37. Delivery Methods….cont’d 12/21/2015 37 Post pyloric access via a duodenal or jejunal nasoenteric tube is preferred when gastric feedings are not tolerated and/or when patients are at risk for aspiration Gastrostomy The placement of a tube through the abdominal wall directly into the stomach if patients require enteral nutrition for prolonged periods (4–6 weeks) Surgical vs PEG
- 38. Delivery method….cont’d 12/21/2015 38 Jejunostomy Jejunal feeding has become increasingly popular uses: associated with a reduction in aspiration enhanced tolerance of enteral nutrition in patients with severe pancreatitis The only absolute contraindication is distal intestinal obstruction.
- 39. Feeding Tolerance 12/21/2015 39 Pts will tolerate If GI output’s ˂600ml/d Isotonic formula of 30ml/hr administered Poor tolerance Vomiting & severe abdominal cramp Gastric residuum >50% over past 4hrs Increased abdominal distension Worsening diarrhea NB: Parenteral nutrition if any of the above
- 40. Enteral Formulas 12/21/2015 40 Low-Residue Isotonic Formulas Isotonic Formulas with Fiber Immune-Enhancing Formulas Calorie-Dense Formulas High-Protein Formulas Elemental Formulas
- 41. low-residue isotonic formulas 12/21/2015 41 Most low-residue isotonic formulas provide a caloric density of 1.0 kcal/Ml standard or first-line formulas for stable patients with an intact gastrointestinal tract Elemental Formulas predigested nutrients and provide proteins in the form of small peptides ease of absorption malabsorption, gut impairment, and pancreatitis
- 42. Parenteral nutrition 12/21/2015 42 Definition considered 7-10 days enteral feeding is not feasible
- 43. Parenteral nutrition....cont’d 12/21/2015 43 TYPES Peripheral parenteral nutrition (PPN) osmolarity 1,000 mOsm (approximately 12% dextrose solution) to avoid phlebitis large volumes (>2,500 mL) are needed Temporary (<2weeks) solutions that contain more than 3% aminoacid and 5% glucose are poorly tolerated peripherally Generally intended as supplement to oral feeding and is not optimal for critically ill pts
- 45. Parenteral nutrition, types....cont’d 12/21/2015 45 Total/central parenteral nutrition (TPN/CPN) provides complete nutritional support The solution, volume of administration, and additives are individualized based on an assessment of the nutritional requirements Catheters placed into the central venous system terminate in the vena cava catheter inserted via subclavian or internal/external jugular vein
- 46. Parenteral nutrition, TPN....cont’d 12/21/2015 46TYPES OF TPN FORMULATIONS TPN formulation without lipid (2-in-1 solution) Calories from amino acids--- 20 to 25% Calories from dextrose------- 75-80% TPN formulation with lipid ( 3-in-1 solution) calories from amino acids----- 20 to 25% calories from lipids------------- 20% calories from dextrose--------- 55 to 60 %
- 47. Parenteral nutrition, TPN....cont’d 12/21/2015 47 Special solutions Additives Electrolytes should be adjusted daily If the serum bicarbonate is low, the solution should contain more acetate The calcium:phosphate ratio must be monitored to prevent salt precipitation
- 48. Parenteral nutrition, TPN....cont’d 12/21/2015 48 Medications: Albumin, H2-receptor antagonists, heparin, iron, dextran, insulin, and metoclopramide can be administered in TPN solutions However, not all medications are compatible with 3-in-1 admixtures Regular insulin should initially be administered subcutaneously according to a sliding scale After a stable insulin requirement has been established, insulin can be administered in the TPN solution, generally at two thirds of the daily subcutaneous insulin dose
- 49. Parenteral nutrition, TPN....cont’d 12/21/2015 49 TPN- macronutrient solutions Crystalline Aas containing 40-50% essential and 50- 60% non essential Aas are used to provide protein needs rich in branched chain for hepatic encephalopathy rich in essential Aas for renal insufficiency pts Glucose in IV solutions is hydrated While there is no absolute requirement of glucose in most pts, providing >150g glucose/d maximizes protein balance Lipid emulsions are available as 10% (1.1kcal/ml) or 20% (2 kcal/ml) solutions and provide energy as well as source of essential fatty acids Rate of infusion should not exceed 1 kcal/kg/h
- 50. INDICATIONS 12/21/2015 Entero-cutaneous fistula Renal failure (ATN) Short bowel syndrome Severe burns Hepatic failure Crohn’s disease Anorexia nervosa Acute radiation enteritis Acute chemotherapy toxicity Prolonged ileus Weight loss preliminary to major surgery 50 Parenteral nutrition, TPN....cont’d
- 51. Parenteral nutrition, TPN....cont’d 12/21/2015 51ADMINISTRATION OF TPN Introduction of TPN should be gradual E.g, approximately 1,000 kcal is provided the first day If there is metabolic stability (i.e.normoglycemia), this is increased to the caloric goal over 1 to 2 days Continuous vs cyclic administration
- 52. ADVANTAGES DISADVANTAGES 12/21/2015 Bed side technique Avoids complications of central venous catheter Avoid multiple venous cannulations Hypertonic solutions can be given Trained personnel is needed Line blockage Mal position Phlebitis Line sepsis thrombosis 52 Parenteral nutrition....cont’d PICC line
- 53. 12/21/2015 53
- 54. ADVANTAGES DISADVANTAGES 12/21/2015 Central access needed Multiple lumen can be used in acute emergency Hypertonic solutions can be given Can be placed for more than 6 weeks Inserted in theatre Increase infection rate Multiple complications 54 Parenteral nutrition....cont’d Central Catheter(Non Tunneled)
- 55. ADVANTAGES DISADVANTAGES 12/21/2015 Convenient exit site Long lasting than non tunnels Hypertonic solutions can be given Removal needs surgical dissection Catheter related sepsis Other complications 55 Parenteral nutrition....cont’d Central Catheter(Tunneled)
- 56. Parenteral nutrition....cont’d 12/21/2015 56 Discontinuation of TPN When the patient can satisfy 75% of his or her caloric and protein needs with oral intake or enteral feeding To discontinue TPN, the infusion rate should be halfed for 1 hour, halved again the next hour, and then discontinued Tapering in this manner prevents rebound hypoglycemia from hyperinsulinemia It is not necessary to taper the rate if the patient demonstrates glycemic stability
- 57. comparison 12/21/2015 57 Enteral Parenteral Cost $10-20 per day $100 or more per day Gut Preserves intestinal function May be associated with gut atrophy Infection Very small risk of infection High risk/incidence of infection and sepsis
- 58. 12/21/2015 58
- 59. Burns 12/21/2015 59 Extensive burns double or tripple REE & urinary nitrogen losses Increase in metabolic demand is proportional to ungrafted body surface Other interations ? Enteral feeding is preferred when tolerated Start within 6-12hrs postburn to reduce hyper metabolism & improve survival
- 60. Burns.... Cont’d 12/21/2015 60 Require 40kcal/TBSA in addition to the maintenance Increased Pr⁻ requirement frm the normal 0.8g/kg/d to 2.5g/kg/d During the hyper metabolic phase of burn injury (0–14 days), the ability to metabolize fat is restricted diet that derives calories primarily from carbohydrate is preferable
- 61. NUTRITION REQUIREMENTS IN HEAD INJURY 12/21/2015 61 Energy requirement calculation 2 wks after HI 120% to 250% above their basal energy expenditure Enteral administration is preferred for acute neurological patients. Nutrition therapy should start early: within 24 to 48 hours of admission to the intensive care unit.
- 62. CONT’D 12/21/2015 62 Enteral formulas: Complete and isotonic formulas should be initially chosen. Start with 30ml/hr Check G.residue Q 4hr ,stop if >125ml Increase by 15-25ml Q 12-24hr as tolerated until desired rate is achieved The Brain Trauma Foundation recommends that total nutritional support should be achieved within 7 days of the injury Prokinetic drugs???
- 63. Acute pancreatitis 12/21/2015 63 The DX of pancreatitis often mandates strict bowel rest for extended periods of time Patients with three or fewer Ranson criteria should be treated with: fluid replacement, nasogastric suction, and bowel rest for at least a week before considering parenteral nutrition Most of these patients can resume an oral diet and do not benefit from TPN Those with more than three Ranson criteria should receive nutritional support
- 64. Ranson’s Criteria Surg Gynecol Obstet 138:69, 1974 Hct decreases > 10% Calcium falls to < 8.0 mg% Base deficit > 4 mEq/L BUN increases > 5 mg% PaO2 is < 60 mmHg If > 3 are present within 48 hours of admission, 60% die
- 65. Cont’d 12/21/2015 65 If severe, initiate early nutrition support (within 72 hours) jejunal feeding is superior to TPN
- 66. Summary of Ideal Feeding Solutions in Acute Pancreatitis Parenteral: Crystalline amino acids, hypertonic glucose solutions (IV fat emulsions tolerated) Enteral: Low fat, elemental, hypertonic solutions given into jejunum
- 67. Nitrogen and Fat Needs in Pancreatitis Nitrogen: 1.0 – 2.0 gm/kg/d Nitrogen balance study is helpful Fat: Fat well tolerated IV and to limited degree in jejunum, no oral fat should be given
- 68. Renal-Failure Formulas 12/21/2015 68 The primary benefits of renal formulas are the lower fluid volume and concentrations of potassium, phosphorus, and magnesium needed to meet daily calorie requirements. This type of formulation almost exclusively contains essential amino acids Has a high nonprotein-calorie:nitrogen ratio; however, it does not contain trace elements or vitamins.
- 69. Pulmonary-Failure Formulas 12/21/2015 69 In pulmonary-failure formulas, fat content is usually increased to 50% of the total calories, with a corresponding reduction in carbohydrate content. The goal is to reduce carbon dioxide production and alleviate ventilation burden for failing lungs.
- 70. cancer 12/21/2015 70 over two-thirds of patients with cancer develop malnutrition Malnutrition associated death in 20–40% of these patients Rx can worsen preexisting malnutrition REE increases by 20-30% in some malignancies Lactic acidosis from high anaerobic metabolism in neoplastic tissue Neoplastic tissues act as nitrogen traps Cancer cachexia manifests as: progressive involuntary weight loss, fatigue, anemia, wasting, and tissue depletion It may occur at any stage of the disease
- 71. Cancer….cont’d 12/21/2015 71 Nutrition support has become an essential adjunct in caring for the cancer patient Nutritional supplementation in cancer patients may reduce : infectious complications perioperative morbidity But convincing evidence of improvement in overall survival is lacking Ample evidence that nutritional supplementation stimulate tumor growth
- 72. Short bowel syndrome 12/21/2015 72 SB ˂ 200cm or ˂ 150cm with ileocecal valve Minimum SB length required to become independent of TPN is 120cms Inadequate intestinal absorptive surface leads to malabsorption, excessive water loss, electrolyte derangements and malnutrition Usually need temporal parenteral nutrition Supplement TPN with oral intake Frequent small meals, avoiding hyperosmolar foods, Restricting fat intake and limiting consumption of high oxalate foods
- 73. SBS.... Cont'd 12/21/2015 73 Adaptation to short gut occurs over time, and initial management should be directed at avoiding electrolyte imbalance and dehydration providing daily caloric requirements through TPN Uniquely formulated diets containing glutamine and human growth hormone have shown promise for accelerating intestinal adaptation Adaptation - Increase in villous height - Luminal diameter - Mucosal thickness
- 74. summary 12/21/2015 74 The gut should always be the preferred route for nutrient administration Subjects receiving intravenous feedings and bowel rest had significantly exaggerated response to injury During parentral nutrition close monitoring of; Serum Na, K on alternative days has LFT, triglycerides weekly to be Renal parameters biweekly remembered
- 75. REFERENCES 12/21/2015 75 Uptodate 20.1 Bailey & Loves short practice of surgery, 25th and 26th edn. Schwartz's principles of surgery,9th and 10th edn. Medscape general surgery Nutrition therapy and pathophysiology ,Marcia nelms ACS, Principles & Practice of Surgery, 6th edn. Greenberg 6th edt
- 76. 12/21/2015 76