2. Norman Barrett
• Norman Rupert Barrett (1903-1979) was
an Australian-born British thoracic
surgeon who is primarily remembered
for describing Barrett’s oesophagus in
1950.
3. Barret esophagus
• Barrett's oesophagus, sometimes called
Barrett syndrome or
• Columnar epithelium lined lower oesophagus (CELLO).
4. Barrett Esophagus
Barrett esophagus is a complication of
chronic GERD ( 5-15%) that is characterized by
intestinal metaplasia within
the esophageal squamous mucosa.
• Barrett esophagus is defined as the replacement
of the normal distal stratified squamous mucosa
by metaplastic columnar epithelium containing
goblet cells.
5.
6. Epidemiology
• The incidence of Barrett esophagus is rising,
and it is estimated to occur in as many as 10%
of individuals with symptomatic GERD.
• Barrett esophagus is most common in white
(Caucasian) males and it typically presents between
40 and 60 years of age.
• The greatest concern in Barrett esophagus is
that it confers an increased risk of
esophageal adenocarcinoma.
7. A pre-malignant condition
Molecular studies suggest that
Barrett epithelium may be more
similar to adenocarcinoma than
to normal esophageal epithelium,
consistent with the view that
Barrett esophagus is a pre-
malignant condition.
8. Epithelial dysplasia
Epithelial dysplasia, considered to be
a pre-invasive lesion, is detected in
0.2% to 2.0% of persons with
Barrett esophagus each year and is
associated with prolonged
symptoms and increased patient
age
9. 90%Although the vast majority of esophageal
adenocarcinomas are associated with Barrett
esophagus,
it is important to remember that most
(90%) individuals with Barrett
esophagus do not develop esophageal
tumors.
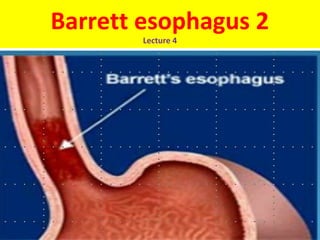
10. Red Patches
Barrett esophagus can be recognized as one or
several tongues or patches of red, velvety
mucosa extending upward from the
gastroesophageal junction.
12. Long segment & Short segment
High-resolution endoscopes have increased the
sensitivity of Barrett esophagus detection. This
has led to subclassification of Barrett esophagus
as long segment, in which 3 cm or more of
esophagus is involved, or short segment, in
which less than 3 cm is involved. It is not yet
clear if the risk of dysplasia in short segment
disease is less than in long segment Barrett
esophagus.
15. What we want to prevent --
Cancer Arising in Barrett’s
Courtesy of Dr. C. Mel WilcoxCourtesy of Dr. C. Mel Wilcox
16. Diagnosis• Diagnosis of Barrett esophagus requires both
endoscopic evidence of abnormal mucosa above
the gastroesophageal junction and histologically
documented intestinal metaplasia.
17. Goblet cells
• Goblet cells, which have distinct mucous vacuoles
that stain pale blue by H&E and impart the shape
of a wine goblet to the remaining
cytoplasm, define intestinal metaplasia and are
necessary for diagnosis of
Barrett esophagus
19. Intestinal metaplasia
• The requirement for intestinal metaplasia
reflects the fact that this feature correlates
with neoplastic risk.
• Foveolar mucus cells, which do not have
distinct mucous vacuoles are insufficient for
diagnosis.
20. Role of Endoscopy
The requirement for an endoscopic abnormality
helps to prevent misdiagnosis
if metaplastic goblet cells within the cardia are
included in the biopsy.
21.
22. Dysplasia
• When dysplasia is present, it is classified as low
grade or high grade. Increased epithelial
proliferation, often with atypical mitoses,
nuclear hyperchromasia and stratification,
irregularly clumped chromatin, increased
nuclear-to-cytoplasmic ratio, and a failure of
epithelial cells to mature as they migrate to the
esophageal surface are present in both grades
of dysplasia.
23. Dysplasia cont.
• Gland architecture is frequently abnormal
and is characterized by budding, irregular
shapes, and cellular crowding.
• High-grade dysplasia exhibits more severe
cytologic and architectural changes.
Intramucosal carcinoma is
characterized by invasion of
neoplastic epithelial cells into the
lamina propria.
24. Barrett esophagus. A, Normal gastroesophageal junction. B, Barrett
esophagus. Note the small islands of paler squamous mucosa within the Barrett mucosa. C,
Histologic appearance of the gastroesophageal junction in Barrett esophagus. Note the
transition between esophageal squamous mucosa (left) and Barrett metaplasia, with
abundant metaplastic goblet cells (right).
25. Clinical Features.
• Barrett esophagus can only be identified thorough
endoscopy and biopsy,
which are usually prompted by GERD symptoms
(dysphagia, heartburn,
regurgitation of sour-tasting
gastric contents & attacks of
severe chest pain).
27. Future Hope
Management of esophageal dysplasia is evolving,
and it is hoped that improved molecular
understanding of neoplastic progression
may allow development of chemopreventive
approaches that reduce incidence of
esophageal adenocarcinoma.
28. Points to Remember
1. In Barrett's esophagus, the tissue lining the esophagus is
replaced by tissue that is similar to the lining of the intestine.
2. Barrett's esophagus is associated with gastroesophageal reflux
disease (GERD).
3. Improvement in GERD symptoms with acid-reducing drugs may
decrease the risk of developing Barrett's esophagus.
4. Barrett's esophagus is diagnosed through an upper
gastrointestinal endoscopy and biopsies.
5. People who have Barrett's esophagus should have periodic
surveillance endoscopies and biopsies.
6. Endoscopic treatments are used to destroy Barrett's tissue,
which will hopefully be replaced with normal esophageal tissue.
7. Removal of most of the esophagus is recommended if a person
with Barrett's esophagus is found to have severe dysplasia or
cancer and can tolerate a surgical procedure.