Case Review #31: 60 Year Old Female with Adult Idiopathic Scoliosis
•
2 j'aime•996 vues

60 year old female presented with Adult Idiopathic Scoliosis and Grade 2 Isthmic Spondylolisthesis. She was treated with an anterior and posterior spinal fusion.

Recommandé
Recommandé
Contenu connexe
Tendances
Tendances (20)
Similaire à Case Review #31: 60 Year Old Female with Adult Idiopathic Scoliosis
Similaire à Case Review #31: 60 Year Old Female with Adult Idiopathic Scoliosis (20)
Plus de Robert Pashman
Plus de Robert Pashman (14)
Dernier
Dernier (20)
Case Review #31: 60 Year Old Female with Adult Idiopathic Scoliosis
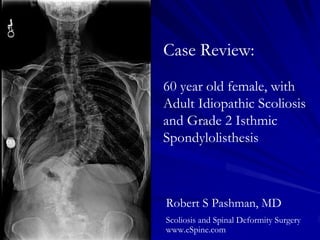
- 1. Case Review: 60 year old female, with Adult Idiopathic Scoliosis and Grade 2 Isthmic Spondylolisthesis Robert S Pashman, MD Scoliosis and Spinal Deformity Surgery www.eSpine.com
- 2. Patient History & Pre-op X-rays 60-year-old female Kim/SRP type 3 curved thoracic lumbar Grade 2 Isthmic Spondylolisthesis of L5-S1. The patient has significant lumbosacral obliquity.
- 3. Indications for Surgery 1. Kim/SRP type 3 adult idiopathic scoliosis. 2. Grade 2 isthmic spondylolisthesis L5-S1. 3. Severe frontal and sagittal plane decompensation of thoracolumbar spine. 4. Osteopenia of thoracolumbar spine. 5. Failed conservative therapy with low back and leg pain.
- 4. Surgical Strategy An anterior interbody fusion is indicated for the following reasons: 1) spondylolisthesis, 2) there is significant rotation and curvature, 3) the frontal and sagittal plane decompensation, 4) and the need for horizontalization of the primary L4-5 and L5- S1 interspace to gain posterior coronal balance. Characteristic of the KIM 3 SRP classification, the patient will need T3 to sacral pelvic fixation. Bilateral fixation is necessary because of the high instability with the isthmic spondylolisthesis. The patient has multiple challenges including some pulmonary disease as well as osteopenia. The instability and progressive curvature which is greater than 80 degrees, thoracic lumbar with significant degeneration, facet arthropathy necessitates osteotomy at multiple levels to induce flexibility of the spine to guarantee sagittal and coronal plane balance.
- 5. Surgical Strategy – Stage 1 Subtotal vertebrectomy L5 for introduction of anterior lumbar interbody fusion graft L5-S1. Interbody complete evacuation of disk and diskectomy L5-S1. Radical diskectomy L4-5. Interbody fusion L4-5, L5-S1 with polyetheretherketone device Alphatec 8-mm with allograft and recombinant human bone morphogenetic protein centrally. Anterior screw fixation L4-5, L5-S1. Intraoperative fluoroscopic control.
- 6. Surgical Strategy – Stage 2 Segmental spinal instrumentation, T3, to the sacral pelvis using titanium screw, cobalt chrome instrumentation. Sacral pelvic fixation, bilaterally, through separate incisions. Posterior spinal fusion, T3 to the sacral pelvis, using locally- harvested autogenous bone and allograft putty. Spinal osteotomy, Smith-Peterson osteotomy T12-L1, L1-2, L2-3, L3- 4, L4-5. Bilateral neural foraminotomy with complete facetectomy and a lateral recess decompression, L1-2, L2-3, L3-4, L4-5 using high- intensity illumination. Reduction spondylolisthesis, L5-S1, using a reduction screw, pedicle screw, and sacropelvic fixation of grade 2 isthmic spondylolisthesis. Intraoperative somatosensory-evoked potential and motor-evoked potential processing. Neuro-navigation with stealth/O-arm intraoperative navigation. Plastic closure of wound.
- 7. Post-Op Films The patient is well balanced in the sagittal and coronal plane. She gained approximately 2 inches in height, and is thrilled with her outcome.