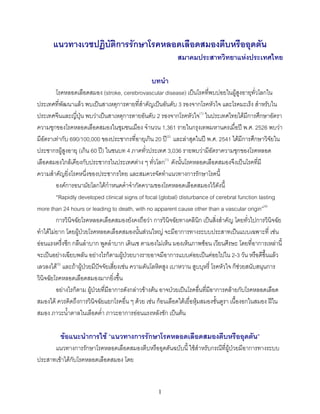
3. แผนภูมิที่ 1
Sudden onset of focal neurological deficit suspecting acute stroke
(Base on history and physical examination )
(Onset 3-72 hr.)
Basic life support (airway, breathing, circulation)
Emergency blood sugar and additional lab: CBC, BUN, creatinine, electrolytes
Emergency non-contrast CT brain scan∗
Non stroke Stroke
Appropriate consultation
and treatment Normal/hypodensity Hyperdensity
(hemorrhage)
AppropriateIschemic stroke
consultation
and treatment
General management
• Avoid antihypertensive except SBP>220mmHg or DBP>120 or MAP> 140 mmHg.
• Avoid intravenous glucose solution unless necessary
• Control BS<180 mg/dl and avoid hypoglycemia
• Treatment of fever and concomitant conditions
∗ ในกรณีที่ไมสามารถทํา CT scan brain ได และมีประวัติและการตรวจรางกายเขาไดกับโรคหลอดเลือดสมองอยางชัดเจน รวมทั้งญาติและผูปวยยอมรับความเสี่ยงที่อาจ
เปนโรคอื่น ที่มีอาการคลายกับโรคหลอดเลือดสมองได ตองบันทึกเหตุผล และมีแนวทางการปฏิบัติดังนี้
- พิจารณาใช Siriraj stroke score เพื่อแยก hemorrhage หรือ infarct ถาเปน hemorrhage ใหสงตอผูปวยไปยังสถานที่ทํา CT scan แตถาเปน infarct
ใหดูวาเปน lacune หรือ non lacune
- ในกรณีที่เปนกลุมอาการของ lacune และไมพบ source of emboli สามารถใหแอสไพรินไปกอน และ observe อาการ 7 วัน ถาดีขึ้นพิจารณาใหยา
antiplatelet ในระยะยาว แตถาอาการเลวลงใหสงตอผูปวยไปยังสถานที่ทํา CT scan ได
- ในกรณี non lacune หรือสงสัย cardiac emboli หรือในกลุม undetermined ใหสงตอเพื่อทํา CT scan เพื่อการวินิจฉัยที่ถูกตอง
∗ ในกรณีที่ CT ปกติ แตอาการและอาการแสดงเขาไดกับ stroke ใหวินิจฉัยโรคโดยใชลักษณะทางคลินิกเปนหลัก
3
4. แผนภูมิที่ 2
Non lacunar infarct with midline shift or herniation
or cerebellar infarct with brainstem compression
Treatment of increased intracranial pressure
Intubation and on respirator
Hyperventilation, Keep pCO2 30-35 mmHg
Elevate head position up 20-30
IV fluid restriction
Osmotherapy and diuretic
Consider surgical intervention
Work up for stroke etiology
Treatment guided by stroke mechanism
Consider PM&R and secondary prevention strategy
∗=Massive MCA or ICA
Hemiplegia with alteration of consciousness with cortical signs (forced eye deviation aphasia/hemi-
inattention), unequal pupils/bilateral signs, or CT shows massive infarct with midline shift.
Cerebellar infarct with brainstem compression
Severe occipital headache with ataxia and cerebellar signs, deterioration of consciousness, clinical brainstem compression (pinpoint
pupils, ophthalmoplegia), or CT shows cerebellar infarct with brainstem co
4
5. แผนภูมิที่ 3
Non Iacunar infarct without midline shift or herniation
or cerebellar infarct without brainstem compression
Close observation for: Glasgow Coma Scale
Pupils size
Clinical signs of brain edema or herniation
Known source of emboli and/or Worsening
Stroke in evolution
Consider
complications of stroke
Yes No
Consider anticoagulant Antiplatelet medications
or antiplatelet medications
Work up for stroke etiology
Treatment and prevention guided by stroke mechanisms
∗ Stroke in evolution=worsening of neurological deficits which are caused by propagation of thrombus rather
than other causes, such as edema, metabolic disturbance
5
6. แผนภูมิที่ 4
Lacunar infarct∗
Oral antiplatelet
Work up for stroke etiology
Treatment and secondary prevention strategy
guided by stroke mechanisms
Stable Worse
Consider PM&R Consider complications stroke
∗=Common clinical lacunar syndromes (patient must have good conciousness and no cortical signs such as
aphasia, apraxia, etc.)
• Pure motor hemiparesis
• Pure sensory stroke
• Motor sensory stroke
• Ataxic hemiparesis
• Dysarthria-clumsy hand sysdrome
And CT findings compatible with lacunar infarct (normal or infarct diameter <1.5 cm. in deep area)
6
7. แผนภูมิที่ 5
(แผนภูมินี้ตองทําในสถาบันที่มีประสาทศัลยแพทยและมีเครื่อง CT scan)
Sudden onset of focal neurological deficit suspecting acute stroke
(Onset < 6 hr)
Basic life support (airway, breathing, circulation) and capillary blood
glucose to exclude hypoglycemia
Facility to investigate and start IV or IA thrombolytic medication within 3 or 6 hours after
stroke onset with inform consent*
No Yes
ability to transfer to appropriate center Emergency lab.
to obtain thrombolytic drug (CBC, BS, BUN, creatinine, electrolytes, EKG)
within 3-6 hours after stroke onset
Emergency non-contrast CT scan brain
Non stroke Stroke
Yes No
Appropriate consultaion
and treatment
Refer** Normal/ Hypodensity Hyperdensity
(hemorrhage)
Consider
appropriate treatment
General management
แผนภูมิที่ 1
Ischemic stroke
Thrombolytic medication***
* การให thrombolytic treatment มีโอกาสเสี่ยงตอภาวะเลือดออกได ตองมีการพูดคุยกับญาติถึงผลดีและผลเสียของ
การรักษา และมีการบันทึกใหความยินยอมเปนหลักฐาน
** ในกรณีตัดสินใจที่จะสงตอ ควรติดตอประสานกับสถาบันที่จะรับผูปวยกอนทุกครั้ง
*** ควรจะรับผูปวยไวใน ICU หรือ acute unit
7
15. เอกสารอางอิง
1. นิพนธ พวงวรินทร. Epidemiology of stroke. ใน: นิพนธ พวงวรินทร, บก. โรคหลอดเลือดสมอง (Stroke)
ฉบับเรียบเรียงครั้งที่ 2 กรุงเทพมหานคร: เรือนแกวการพิมพ, 2544: 1-37.
2. Viriyavejakul A, Poungvarin N, Vannasaeng S. The prevalence of stroke in urban community of
Thailand. J Neurology 1985; 232 (suppl): 93.
3. Viriyavejakul A, Senanarong V, Prayoonwiwat N, Praditsuwan R, Chaisevekul R, Poungvarin N.
Epidemiology of stroke in the elderly in Thailand. J Med Assoc Thai 1998; 81: 487-505
4. World Health Organization Meeting on Community Control of Stroke and Hypertension. Control
of stroke in the community: methodological considerations and protocol of WHO stroke register.
CVD/s/73.6 Geneva: WHO, 1973.
5. Adams H P Jr, Brott TG, Cowell RM, et al. Guidelines for the management of patients with acute
ischemic stroke. A statement for healthcare professionals from a special writing group of the
Stroke Council, Amerian Heart Association. Stroke 1994;25: 1901-14.
6. Poungvarin N, Viriyavejakul A, Komontri C. Siriraj stroke score and validation study to distinguish
supratentorial intracerebral haemorrhage from infarction. Br Med J 1991; 302 : 1565-7.
7. ZhengMing Chen, Sandercock P, Pan HC, et al. Indications for early aspirin use in acute
ischemic stroke. A combined analysis of 40,000 randomized patients from the Chinese Acute
Stroke Trial and the Internationl Stroke Trial. Stroke 2000;31: 1240-9.
8. The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue
plasminogen activator for acute ischemic stroke. N Engl J Med 1995;333: 1581-7.
9. Adams HP, Brott TG, Furlan AJ, et al. Guidelines for thrombolytic therapy for acute stroke: a
supplement to the guidelines for the management of patients with acute ischemic stroke: a
statement of healthcare professionals from a special writing group of the stroke Council,
American Heart Association. Circulation. 1996;94: 1167-74
10. Symon L, Branston N, Strong A. Autoregulation in acute focal ischemia. An experimental study.
Stroke 1976; 7: 547-54.
11. Straudgaard S. Autoregulation of cerebral blood flow in hypertensive patients. Cerculation
1976;58: 720-7.
15
16. 12. Straudgaard S, Paulon O. Cerebral blood flow and is pathophysiology in hypertension. Am j
Hypertens 1989; 2: 486-92.
13. Hatashita S, Hoff J, Ishii S. Focal brain edema associated with acute arterial hyperetnsion. J
Neurosurg 1986; 64: 643-9.
14. Hacke W, Kaste M, Skyhoj Olsen T, Hacke W, Orgogozo JM. For the EUSI Executive Committee.
Acute treatment of ischemic stroke. Cerebrovasc Dis 2000; 10 (suppl 3): 22-33.
15. Broderick JP, NINDS. Guidelines for medical care and treatment of blood pressure in patients
with acute stroke. Proceeding of a National Symposium on Rapid Identification and Treatment of
Acute Stroke. December 12-13, 1996.
16. CAST(Chinese Acute Stroke Trial) Collaborative Group. CAST: randomized placebo controlled
trial of early aspirin use in 20,000 patients with acute ischemic stroke. Lancet 1997; 349: 1641-9.
17. International Stroke Trial Pilot Study Collaborative Group. Study Design of the International
Stroke Trial (IST), baseline data, and outcome in 984 randomized patients in the pilot study. J
Neurol Neurosurg Psychiat 1996; 60: 371-6.
18. International Stroke Trial Collaborative Group. The International Stroke Trial (IST): a randomized-
trial of aspirin, subcutaneous heparin, both, or neither among 19,435 patients with acute
ischemic stroke. Lancet 1997; 349: 1569-81.
19. Gubitz G, Sandercock P, Prevention of ischemic stroke. Br Med J 2000; 321: 1455-9.
20. Poungvarin N, Opartkiattikul N, Chaithiraphan S, Viriyavejakul A. A comparative study of
coumadin and aspirin for primary cardioembolic stroke and thromboembolic prevention of
chromic rheumatic mitral stenosis with atrial fibrillation. J Med Assoc Thai 1994; 77: 1-8.
21. Ferlan A, Higashida R, Wechsler L, et al. Intra-arterial prourokinase for acute ischemic stroke.
22. The PROACT II study: a randomized controlled trial. Prolyse in acute cerebral thromboembolism.
JAMA 1999; 282: 2003-11.
23. Bogousslavsky J, Kaste M, Skyhoj Olsen T, Hacke W, Orgogozo JM. For the EUSI executive
Committee. Risk factors and stroke prevention. Cerebrovasc Dis 2000; 10 (suppl 3): 12-21.
24. Gresham E.E., Duncan P.W. (Eds.) Post Stroke Rehabilitation, Clinical Practice Guideline. U.S.
department of Health and Human Services, Public Health Service. Rockville: AHCRP Publication
95-0662, 1995; 67-79
16