Urticaria&angioedema(copiedsenior)
•Télécharger en tant que PPT, PDF•
8 j'aime•1,802 vues


Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
En vedette (20)
Similaire à Urticaria&angioedema(copiedsenior)
Similaire à Urticaria&angioedema(copiedsenior) (20)
Plus de Habrol Afzam
Plus de Habrol Afzam (20)
Dernier
Dernier (20)
Urticaria&angioedema(copiedsenior)
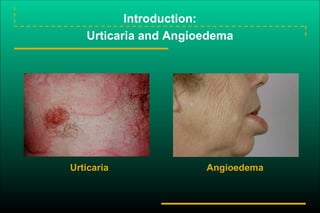
- 1. Introduction: Urticaria and Angioedema Urticaria Angioedema
- 2. Etiology of Urticarial Reactions: Allergic Triggers Acute Urticaria Drugs Foods Food additives Viral infections –hepatitis A, B, C –Epstein-Barr virus Insect bites and stings Contactants and inhalants (includes animal dander and latex) Chronic Urticaria Physical factors –cold –heat –dermatographic –pressure –solar Idiopathic
- 3. Chronic Urticaria & Angioedema Definition: Hives occurring greater than 6 weeks Hives and angioedema (40%) Hives alone (40%) Angioedema alone (20%) Etiology: Difficult to determine, cause rarely found Common in 3rd and 4th decade of life Usually not foods, drugs, pollens, infections, “dyes” Bad News: May last years….
- 4. HEURISTIC SUBDIVISIONSca 1. Acute urticaria - less than 6 weeks; history implicates cause in approx. 50%; difficult to study in clinical trials; good prognosis. 2. Chronic urticaria - greater than 6 weeks; workup indicated; easier to study; often persistent. 3. Chronic idiopathic urticaria - subset of chronic urticaria in which workup fails to pinpoint cause; diagnosis by exclusion; not homogeneous.
- 5. • Immune-mediated urticaria • The type I allergic immunoglobulin (Ig) E response is initiated by antigen-mediated IgE immune complexes that bind and cross-link Fc receptors on the surface of mast cells and basophils, thus causing degranulation with histamine release. • The type II allergic response is mediated by cytotoxic T cells, causing deposits of immunoglobulins, complement, and fibrin around blood vessels. This leads to urticarial vasculitis. • The type III immune-complex disease is associated with systemic lupus erythematosus and other autoimmune diseases that cause urticaria.[
- 6. • Non--immune-mediated urticaria • Complement-mediated urticaria includes viral and bacterial infections, serum sickness, and transfusion reactions. Urticarial transfusion reactions occur when allergenic substances in the plasma of the donated blood product react with preexisting IgE antibodies in the recipient. Certain drugs (opioids, vecuronium, succinylcholine, vancomycin, and others) as well as radiocontrast agents cause urticaria due to mast cell degranulation through a non-IgE-mediated mechanism
- 10. Physical Urticarias Reproducible by environmental factors Physical stimuli Most frequently in young adults Episodic and often limited to areas of inciting stimulus Usually, unresponsive to corticosteroids Overall, treatment with non-sedating antihistamines
- 11. Examples of Physical Urticarias Answer: Dermatographism 1. If you stroke the skin, and a hive occurs? 2. If you place an ice cube on the forearm, and after removal of ice cube, hive occurs? Answer: Cold-induced urticaria 3. If hives occur when the patient sweats or exposure to heat? Answer: Cholinergic urticaria or localized heat urticaria
- 12. Urticarial Vasculitis (Rare) Inflammatory injury of capillaries and postcapillary venules in the skin. Etiology: Manifestation of systemic disease Clinically: Hives persisting > 24 hours ± pruritic Painful, stinging, burning sensation “Leaves a trace” –Faint residual hyperpigmentation, indicating red blood cell extravasation
- 13. The Pathogenesis of Chronic Urticaria: Cellular Mediators
- 14. Histamine as a Mast Cell Mediator
- 15. Role of Mast Cells in Chronic Urticaria: Lower Threshold for Histamine Release Release threshold decreased by: Cytokines & chemokines in the cutaneous microenvironment Antigen exposure Histamine-releasing factor Autoantibody Psychological factors Release threshold increased by: Corticosteroids Antihistamines Cromolyn (in vitro) Cutaneous mast cell
- 16. An Autoimmune Basis for Chronic Idiopathic Urticaria: Antibodies to IgE
- 17. Angioedema (Swelling) Edema of the deep layers of the dermis and subcutaneous tissue. Non-pitting edema Skin is not hot Non-dependent areas It is not: “pre-tibial pitting edema”
- 18. • The swelling of the affected area of angioedema is a result of the fast onset of increase of local vascular permeability in submucosal and subcutaneous tissue. IgE-mediated mast cell activation and degranulation, key elements of an allergic reaction, often manifest as urticaria and angioedema. Non– IgE-mediated mast cell activation/mediator release may explain certain autoimmune-mediated and idiopathic angioedema
- 19. • Patients usually describe swelling of the face (eg, eyelids, lips), tongue, hands, and feet. It can be acute or chronic, and each episode of angioedema may last a few hours to a few days. A local burning sensation and pain can be observed without pronounced itchiness or local erythema.
- 20. • Abdominal pain can sometimes be the only presenting symptom of angioedema. Throat tightness, voice changes, and trouble breathing may indicate airway involvement. • For acute and new-onset angioedema, special attention should be directed to the potential relationship with food or drug intake, insect stings, or other unusual exposures. For chronic and recurrent cases, ask the patient about potential triggers, medication use and associated medical history, family history, and past evaluation.
- 21. Allergic angioedema • Allergic angioedema is often associated with urticaria. It is typically observed within 30 minutes to 2 hours after exposure to the allergen (eg, food, drug, venom, latex).
- 22. Pseudoallergic angioedema • Pseudoallergic angioedema is not IgE-mediated. However, its clinical course and presentation is very similar to allergic angioedema. Typical examples are angioedema induced by nonsteroidal anti-inflammatory drugs (NSAIDs) and intravenous contrast material; aspirin (ASA) is the most common culprit.
- 23. Nonallergic angioedema • Nonallergic angioedema does not involve IgE or histamine; urticaria is generally not associated with this type of angioedema. • Hereditary angioedema (HAE) is perhaps the prototype of this type of angioedema. Decreased functional C1-INH production leading to unchecked bradykinin production are believed to be the fundamental changes in HAE types I and II.[20] Acquired angioedema (AAE) also has decreased C1-INH function due to autoantibody production or accelerated consumption of C1-INH.
- 24. Idiopathic angioedema • The causes of idiopathic angioedema are, by definition, not identifiable. Furthermore, the exact mechanisms are unclear. [11, 12] Some may be associated with urticaria. Based on responses to medication, some cases are thought to be mediated by mast cell activation, albeit IgE-independent. • Physical urticaria/angioedema: Common triggers include heat, cold, emotional stress, and exercise. Nonspecific mast cell activation and degranulation are suspected causes.
- 25. Treatment • Histamine-mediated angioedema • Histamine-mediated angioedema is either IgE-dependent (eg, allergic reaction due to food or drug) or IgE-independent (eg, radiocontrast media). NSAIDs related and most idiopathic angioedema are treated with same measures. • Most cases can be managed well with outpatient treatment alone. Antihistamines as described in the urticaria article are often used as the first-line treatment for angioedema
- 26. • For moderate to severe cases, close monitoring is often necessary. Diphenhydramine (50) mg IM/IV is helpful. Hydrocortisone (200 mg) or Solu-Medrol (40-60 mg) IV may reduce the possibility of relapse. • For laryngeal swelling and airway obstruction, close monitoring of the airway is mandatory. Epinephrine (1:1,000) should be administrated IM at 0.01 mg/kg or 0.3 mg repeated every 10-15 min, if necessary. Occasionally, intubation or even tracheostomy may be necessary. These patients should be admitted for at least 24 hours of observation.
- 27. • Bradykinin-mediated angioedema • Antihistamines do not work for these patients. • Cortical steroids have limited or no value. • Monitor and support airway as in histamine-mediated angioedema. • Epinephrine does not work as well as in histamine-mediated angioedema. Its value for treating acute HAE attacks is limited. • Severe abdominal pain may sometimes be the only presenting symptom for these patients when seeking emergency medical care. • Supportive care includes pain control and relief of nausea.
- 28. • Fresh frozen plasma (2 units) has been shown to be helpful in certain patients. However, fresh frozen plasma worsening an acute attack of laryngoedema has also been reported. If this treatment is used, be ready to intubate or perform a tracheostomy, if necessary. • Antifibrinolytics (eg, Amicar or Traxeminic acid) may be helpful.
- 29. Initial Workup of Urticaria Patient history Sinusitis Arthritis Thyroid disease Cutaneous fungal infections Urinary tract symptoms Upper respiratory tract infection (particularly important in children) Travel history (parasitic infection) Sore throat Epstein-Barr virus, infectious mononucleosis Insect stings Foods Recent transfusions with blood products (hepatitis) Recent initiation of drugs Physical exam Skin Eyes Ears Throat Lymph nodes Feet Lungs Joints Abdomen
- 30. Laboratory Assessment for Chronic Urticaria Possible tests for selected patients Stool examination for ova and parasites Blood chemistry profile Antinuclear antibody titer (ANA) Hepatitis B and C Skin tests for IgE-mediated reactions Initial tests CBC with differential Erythrocyte sedimentation rate Urinalysis RAST for specific IgE Complement studies: CH50 Cryoproteins Thyroid microsomal antibody Antithyroglobulin Thyroid stimulating hormone (TSH)
- 31. Histopathology Group 2: Polymorphous perivascular infiltrate Neutrophils Eosinophils Mononuclear cells Group 3: Sparse perivascular lymphocytes
- 32. Urticaria Associated With Other Conditions Collagen vascular disease (eg, systemic lupus erythematosus) Complement deficiency, viral infections (including hepatitis B and C), serum sickness, and allergic drug eruptions Chronic tinea pedis Pruritic urticarial papules and plaques of pregnancy (PUPPP) Schnitzler’s syndrome
- 33. H1-Receptor Antagonists: Pros and Cons for Urticaria and Angioedema First-generation antihistamines (diphenhydramine and hydroxyzine) Advantages: Rapid onset of action, relatively inexpensive Disadvantages: Sedating, anticholinergic Second-generation antihistamines (astemizole, cetirizine, fexofenadine, loratadine) Advantages: No sedation (except cetirizine); no adverse anticholinergic effects; bid and qd dosing Disadvantages: Prolongation of QT interval; ventricular tachycardia (astemizole only) in a patient subgroup
- 34. An Approach to the Treatment of Chronic Urticaria
- 35. Treatment of Urticaria: Pharmacologic Options Antihistamines, others First-generation H1 Second-generation H1 Antihistamine/decongestant combinations Tricyclic antidepressants (eg, doxepin) Combined H1 and H2 agents Beta-adrenergic agonists Epinephrine for acute urticaria (rapid but short-lived response) Terbutaline Corticosteroids Severe acute urticaria –avoid long-term use –use alternate-day regimen when possible Avoid in chronic urticaria (lowest dose plus antihistamines might be necessary) Miscellaneous PUVA Hydroxychloroquine Thyroxine
- 36. Atopic Dermatitis: Acute, Subacute, and Chronic Lesions Acute Cutaneous Lesions Erythematous, intensely pruritic papules and vesicles Confined to areas of predilection –cheeks in infants –antecubital –popliteal Subacute Cutaneous Lesions Erythema excoriation, scaling Bleeding and oozing lesions Chronic Lesions Excoriations with crusting Thickened lichenified lesions Postinflammatory hyperpigmentation Nodular prurigo
- 37. Atopic Dermatitis: Physical Distribution by Age Group
- 38. Immune Response in Atopic Dermatitis Markedly elevated serum IgE levels Peripheral blood eosinophilia Highly complex inflammatory responses > IgE-dependent immediate hypersensitivity Multifunctional role of IgE (beyond mediation of specific mast cell or basophil degranulation) Cell types that express IgE on surface –monocyte/macrophages –Langerhans’ cells –mast cells –basophils
- 39. Atopic Dermatitis: Tests to Identify Specific Triggers Skin prick testing for specific environmental and/or food allergens RAST, ELISA, etc, to identify serum IgE directed to specific allergens in patients with extensive cutaneous involvement Tzanck smear for herpes simplex KOH preparation for dermatophytosis Gram’s stain for bacterial infections Culture for antibiotic sensitivity for staphylococcal infection; supplement with bacterial cultures Cultures to support tests bacterial, viral, or fungal
- 40. Topical Corticosteroids Ranked from high to low potency in 7 classes –Group 1 (most potent): betamethasone dipropionate 0.05% –Group 4 (intermediate potency): hydrocortisone valerate 0.2% –Group 7 (least potent): hydrocortisone hydrochloride 1% Local side effects: Development of striae and atrophy of the skin, perioral dermatitis, rosacea Systemic effects: Depend on potency, site of application, occlusiveness, percentage of body covered, length of use May cause adrenal suppression in infants and small children if used long term
- 41. Antihistamines and Other Treatments Standard Treatment Oral antihistamines to relieve itching Moisturizer to minimize dry skin Topical corticosteroids Hard-to-manage Disease Antibiotics Coal tar preparations (antipruritic and anti-inflammatory) Wet dressings and occlusion Systemic corticosteroids UV light therapy Hospitalization
Notes de l'éditeur
- 1