Casos Clínicos
•Télécharger en tant que PPT, PDF•
1 j'aime•567 vues

caso clínicos de pacientes com patologia. Identificar a patologia através da visualização das imagens radiológicas.

Recommandé
Recommandé
Contenu connexe
Tendances
Tendances (20)
Similaire à Casos Clínicos
Similaire à Casos Clínicos (20)
Dernier
Dernier (20)
Casos Clínicos
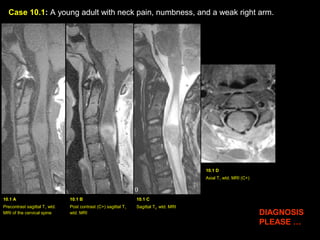
- 1. Case 10.1: A young adult with neck pain, numbness, and a weak right arm. 10.1 A Precontrast sagittal T1 wtd. MRI of the cervical spine 10.1 B Post contrast (C+) sagittal T1 wtd. MRI 10.1 C Sagittal T2 wtd. MRI 10.1 D Axial T1 wtd. MRI (C+) DIAGNOSIS PLEASE …
- 2. Case 10.2: A middle-aged male with gradual weakness of both arms. 10.2 A Post contrast (C+) sagittal T1 wtd. MRI 10.2 C Axial T1 wtd. MRI (C+) 10.2 B Sagittal T2 wtd. MR image of the C-spine DIAGNOSIS PLEASE …
- 3. Name 2 common intramedullary tumors involving the spinal cord. A. ? B. ?
- 4. Name 2 common intramedullary tumors involving the spinal cord. A. Astrocytoma B. Ependymoma
- 5. Case 10.3: A 50-year-old patient with renal cell carcinoma with back pain and leg weakness. 10.3 A Sagittal T1 wtd. MRI of the lumbar spine 10.3 B Post contrast (C+) sagittal T1 wtd. MRI 10.3 C Sagittal T2 wtd. MRI DIAGNOSIS PLEASE … 10.3 D Axial T1 wtd. MRI (C+)
- 6. Case 10.4: A 55-year-old lady with gradual lower extremity weakness. 10.4 A Post contrast (Ct) sagittal T1 wtd. MRI DIAGNOSIS PLEASE … 10.4 B Sagittal T2 wtd. MRI of thoracic spine 10.4 C Precontrast sagittal T1 wtd. MRI 10.4 D Axial CT image of the thoracic spine
- 7. Case 10.5: A 24-year-old male with neck pain and right arm weakness. 10.5 A Precontrast sagittal T1 wtd. MRI of C- spine DIAGNOSIS PLEASE … 10.5 B Post contrast (C+) sagittal T1 wtd. MRI 10.5 C Precontrast axial T1 wtd. MRI 10.5 D Axial T1 wtd. MRI (C+)
- 8. Name 2 common intradural tumors within the spinal canal: A. ? B. ?
- 9. Name 2 common intradural tumors within the spinal canal: A. Nerve sheath tumors (schwannoma, neurofibroma) B. Meningioma
- 10. Case 10.6: A 42-year-old patient, developed acute bilateral paraparesis following placement of an epidural catheter for drug delivery to relive constant severe back pain. 10.6 A Post contrast sagittal T1 wtd. MRI of the thoracic spine DIAGNOSIS PLEASE … 10.6 B Post contrast Axial T1 wtd. MRI
- 11. Case 10.7: A 68 yr. Old male with renal cell carcinoma with progressive difficulty in walking and weakness involving both legs. 10.7 A Pre-contrast sagittal T1 wtd. MRI of the thoracic spine DIAGNOSIS PLEASE … 10.7 B Sagittal T2 wtd. MRI 10.7 C Post contrast sagittal T1 wtd. MRI 10.7 D Pre contrast axial T1 wtd. MRI
- 12. Answers
- 13. Case 10.1: A young adult with neck pain, numbness, and a weak right arm. A. B. C. D. Findings: : An inhomogeneously enhancing tumor (red arrow in B) is seen within the upper cervical cord. Large cysts (C) are seen both above and below the tumor, best seen on T2 wtd. image C. Eccentric location of the tumor, more to the right of the cervical cord (yellow arrow) is shown on axial image D. Diagnosis: Astrocytoma C C
- 14. Astrocytoma of the Spinal Cord Incidence: Common intramedullary tumor particularly in children and young adults. Pathology: Usually low grade MRI Findings: • Eccentric location of tumor within the spinal cord • Multisegmental involvement • Variable degree of tumoral enhancement • Cysts are common • Hemorrhage is rare Treatment: • Complete resection of tumor is not possible due to infiltrative nature. Radiation therapy is also used for recurrence or growing tumors.
- 15. Case 10.2: A middle-aged male with gradual weakness of both arms. 10.2 A Post contrast (C+) sagittal T1 wtd. MRI 10.2 C Axial T1 wtd. MRI (C+) 10.2 B Sagittal T2 wtd. MR image of the C-spine Findings: : A sausage-shaped intensely enhancing tumor (yellow arrow in A) is seen within the upper cervical cord extending from just above the cranio-cervical junction with involvement of the dorsal medulla (black arrow in A) down to C5 level. Small amount of old blood is better seen on T2 wtd. image as an area of dark signal intensity within the tip of the tumor (white arrow in B). Central location of tumor (yellow arrows in C) is better appreciated on axial post contrast image. Diagnosis: Ependymoma
- 16. Ependymoma of the Spinal Cord Incidence: Common intramedullary tumor in adults Pathology: Cellular tumors that originate from ependymal cells lining the central canal. Clinical Symptoms: Nuchal pain/radicular pain, Paresthesia, Motor weakness MRI Findings: Moderate to markedly enhancing tumor, Blood products from hemorrhage within the tumor is common, Tumor can also contain intrinsic cysts. Treatment: Surgery. Ependymoma have a well-defined cleavage plane between the tumor and adjacent spinal cord. Thus, the tumor can be completely resected with modern neurosurgical techniques with relief of clinical symptomatology. Recurrence is rare following complete resection.
- 17. Case 10.3: A 50-year-old patient with renal cell carcinoma with back pain and leg weakness. 10.3 A Sagittal T1 wtd. MRI of the lumbar spine 10.3 B Post contrast (C+) sagittal T1 wtd. MRI 10.3 C Sagittal T2 wtd. MRI 10.3 D Axial T1 wtd. MRI (C+) Findings: : Bony metastasis (yellow arrow in A, B, C) is seen involving the T12 vertebral body. Intramedullary location of metastasis within the distal thoracic cord, is verified on post contrast sagittal image (red arrow in B) and axial image (red arrow in D). Edema (green arrow in C) within the thoracic cord is best shown on T2 wtd. image C. Diagnosis: Bony Metastasis and metastasis to the Spinal Cord
- 18. Metastasis to the Spinal Cord Incidence: Rare Primary Sites: •Lung •Breast •Melanoma •Kidney •Lymphoma/Leukemia Intracerebral Tumors: •Medulloblastoma •Ependymoma •Glioblastoma •Germ Cell Tumor Route of Spread: Arterial seeding, Batson’s venous plexus, Drop metastasis (from intracerebral tumor)
- 19. Case 10.4: A 55-year-old lady with gradual lower extremity weakness. 10.4 A Post contrast (C+) sagittal T1 wtd. MRI 10.4 B Sagittal T2 wtd. MRI of thoracic spine 10.4 C Precontrast sagittal T1 wtd. MRI 10.4 D Axial CT image of the thoracic spine Findings: : An intradural enhancing meningioma (arrow in A), the ventrally located tumor has produced cord compression and with displacement of the thoracic cord (red arrow in D) to the right side. Calcified nature of the tumor is identified on sagittal T2 wtd. image as an area of dark signal intensity (yellow arrow in B) and confirmed by CT imaging (yellow arrow in D) as an area of high attenuation density. Diagnosis: Classic example of calcified intradural meningioma
- 20. Intraspinal Meningioma Incidence: • Second common intradural tumor • Middle-aged females (80%) • Thoracic spine (80%), cervical spine (15%) MRI Findings: • Intensely enhancing intradural tumor • Calcification, when seen, clinches the diagnosis Treatment: • Surgery
- 21. Case 10.5: A 24-year-old male with neck pain and right arm weakness. 10.5 A Precontrast sagittal T1 wtd. MRI of C.spine 10.5 B Post contrast (C+) sagittal T1 wtd. MRI 10.5 C Precontrast axial T1 wtd. MRI 10.5 D Axial T1 wtd. MRI (C+) Findings: An enhancing intradural nerve sheath tumor (Schwannoma) is shown (red arrow in B and D). Dumbbell shape of tumor with intraspinal component (red arrow in D) producing cord compression (yellow arrow in D) and paraspinal tumor extension through an enlarged neural foramen (green arrow in C & D) following the exiting nerve root is best shown on axial post contrast image D. Diagnosis: Schwannoma arising from the spinal nerve root
- 22. Intraspinal Nerve Sheath Tumors Incidence: Most common intradural tumor • Solitary nerve sheath tumor is usually Schwannoma and commonly seen in adults. • Multiple nerve sheath tumors are usually neurofibromas and commonly seen in the pediatric age group with neurofibromatosis MRI Findings: • Dumbbell shaped enhancing intradural tumor with paraspinal extension through enlarged neural foramen is a characteristic feature of nerve sheath tumor. • Can cause cord compression. Treatment: Surgrey
- 23. Case 10.6: A 42-year-old patient, developed acute bilateral paraparesis following placement of an epidural catheter for drug delivery to relive constant severe back pain. 10.6 A Post contrast sagittal T1 wtd. MRI of the thoracic spine 10.6 B Post contrast Axial T1 wtd. MRI Findings: The central portion of the midthoracic cord is compressed and displaced anteriorly (red arrows in A outline the thoracic cord both above and below the level of cord compression) by an epidural abscess (yellow arrows in A, B). The capsule of the abscess enhances intensely with central low signal intensity produced by pus. Figure B demonstrates ventrally displaced thoracic cord (red arrow) by dorsally located epidural abscess (yellow arrows). Diagnosis: Epidural abscess Treatment: Surgical drainage and antibiotics.
- 24. Case 10.7: A 68 yr. Old male with renal cell carcinoma with progressive difficulty in walking and weakness involving both legs. 10.7 A Pre-contrast sagittal T1 wtd. MRI of the thoracic spine 10.7 B Sagittal T2 wtd. MRI 10.7 C Post contrast sagittal T1 wtd. MRI 10.7 D Pre contrast axial T1 wtd. MRI Findings: Bony metastasis involving the T8 vertebral body, right pedicle/transverse process and spinous process (arrow in A,B,C,D) with epidural tumor producing marked degree of cord compression (red arrow). Diagnosis: Bony metastasis from renal cell carcinoma with epidural tumor producing cord compression