Beta adrenergic blockers
•Télécharger en tant que PPTX, PDF•
41 j'aime•27,283 vues

This presentation deals with the beta blockers commonly used in day-to-day practice alongwith some interesting mnemonics to remember their names & site of action

Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
En vedette (20)
Similaire à Beta adrenergic blockers
Similaire à Beta adrenergic blockers (20)
Plus de Karun Kumar
Plus de Karun Kumar (20)
Dernier
Dernier (20)
Beta adrenergic blockers
- 1. Beta adrenergic blockers Moderator Dr. Ali Ahmad Resident Dr. Karun Kumar (JR – II)
- 2. Overview of presentation • Location & effects of β receptors • Classification & brief overview of β blockers • Chemistry & Pharmacokinetics of β blockers • Pharmacodynamics of β blockers • Effects of β blockers on CVS, RS, Eye, Metabolic, etc. • Clinical pharmacology of β blockers and rationale of use • Synopsis of β blockers (Uses, A/E, C/I, Interactions)
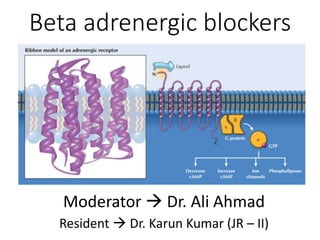
- 3. Location of β receptors
- 6. Introduction • All β blockers used clinically are competitive pharmacologic antagonists • 1958 Dichloroisoprenaline (low potency & partial agonist) • 1963 Propranolol (blocks β1,β2 & weak activity on β3). Also, an inverse agonist (↓ resting HR*) *HR – Heart Rate
- 7. Classification I. Nonselective (β1 and β2) a. Without ISA* Propranolol, Sotalol, Timolol. b. With ISA* Pindolol c. Addnl. α blocking property Labetalol, Carvedilol II. Cardioselective (β1) [safe in asthmatics] Metoprolol, Atenolol, Acebutolol, Bisoprolol, Esmolol, Betaxolol, Celiprolol, Nebivolol *ISA - intrinsic sympathomimetic activity
- 8. Non-selective beta blockers • Most imp. effects CVS & bronchial sm. Muscle • Competitively block the effects of NE on β1 & β2 • Some exhibit ISA & memb. stabilizing (LA) activity • Blockade of β1 receptors (Heart, Kidneys) • Blockade of β2 receptors (Lungs, Liver) • Also mask some of the early signs of hypoglycemia (e.g., tachycardia and sweating) in diabetic patients
- 9. Cardioselective β blockers (Rationale) 1. ↓ propensity to cause bronchoconstriction 2. Safer in diabetics 3. ↓ incidence of cold hands and feet 4. Less deleterious effect on blood lipid profile 5. Less liable to impair exercise capacity
- 11. FPMBBB
- 12. Pharmacodynamics
- 13. β1 β3β2
- 14. Effect on CVS • Do not cause hypotension in healthy individuals • Slowed AV conduction with ↑ PR interval β1 block in AVN • In vascular system, β2 blockade ↑ SVR (α1) • Nonselective and β1-block Inhibit renin • Acute effects ↑ peripheral resistance • Chronic drug admin. ↓ peripheral resistance
- 17. Effect in an anaesthetized dog
- 18. Effect on respiratory tract • Blockade of β2 rec. in bronchial smooth muscle ↑ airway resistance (asthma) • Patients with chronic obstructive pulmonary disease (COPD) tolerate these drugs quite well & benefits outweigh the risks (Albouaini et al., 2007) • Patients with COPD discharged with β-blockers after an MI had a lower all-cause mortality compared to patients not prescribed β-blockers (Andell et al., 2015) [JAHA, 2015]
- 19. Other effects • Eye ↓ i.o.p. (glaucoma) • Metabolic & Endocrine - inhibit SNS stimulation of lipolysis ↑ VLDL & ↓ HDL • Sotalol Nonselective β-receptor antagonist that lacks LA action but has marked class III antiarrhythmic effects, reflecting K channel blockade
- 20. Clinical Pharmacology of β blockers 1. Hypertension 2. Ischemic heart disease (Angina, MI) 3. Cardiac arrhythmias 4. Heart failure 5. Glaucoma 6. Hyperthyroidism 7. Neurologic disease (Migraine, tremors, “stage fright”) 8. Miscellaneous (BOV)
- 21. Hypertension
- 28. • Atenolol Less lipophilic (fewer CNS s/e) • Labetalol chr. HTN & HTN emergencies. Because of its α-adrenoceptor–blocking activity, it can cause orthostatic hypotension. • Esmolol (i.v.) HTN in surgical patients & in persons with HTN emergencies • Carvedilol Antioxidant properties that can protect the vascular wall from free radicals that damage blood vessels and thereby contribute to the progression of cardiovascular disease. • Nebivolol (3rd gen.) selective β1-blocker with antioxidant properties; ↑ endothelial NO rel. (vasodilating effect)
- 29. Management of Hypertension • Lifestyle Modifications exercise,wt. loss, mod. of alcohol intake & diet low in Na & adeq. K Ca Mg. Fruits & vegetables & low sat. & total fat. • Selection of Drug Therapy • Stage I HTN A+B (<55) ; C + D (>55) • Stage II HTN 1 out of A/B + 1 out of C/D • Step 3 A/B + C + D • Step 4 (Resistant HTN) A + B + C + D
- 31. Rationale for use • Typical angina pectoris and acute MI but NOT in vasospastic angina/acute anginal attacks. • In typical angina Prevent exercise-induced tachycardia & ↓ MOD (myocardial O2 demand) • Also prevent reflex tachycardia induced by either organic nitrates or DHPs CCBs • Post-MI ↓ risk of recurrence & improve survival • MI Metoprolol (i.v.) during the early phase of treatment, followed by oral maintenance therapy • C/I HF late stage (-ve inotropic effect)
- 32. • Abrupt withdrawal of BB should not be done (ppt. angina attack & acute MI due to sudden ↑ sympathetic tone of heart; upregul. Of beta rec. (tapered over 2-3 days)] • ↑ EDV & ↑ ejection time (↑ MOD) blunts beneficial effects of BB if used as a single drug therapy for angina
- 33. Additional use • β-blockers protect the heart against the damage caused by ischemia and free radicals that may be formed during reperfusion of the coronary arteries when fibrinolytic drugs are used.
- 34. • Prophylaxis β-blocker/long-acting NO3/CCB • β-blockers ↓ risk of MI & improve survival in SA • UA Aspirin + β-blockers for patients with unstable • VA CCB • Angina & asthma CCB (relax bronch. sm. Musc.) • angina & diabetes CCB/β1 blocker/3rd gen • HF long-acting nitrate (angina prophylaxis)
- 35. β blocker + long-acting NO3 because: (a) Tachycardia due to nitrate is blocked by β blocker. (b) The tendency of β blocker to cause ventricular dilatation is counteracted by nitrate. (c) The tendency of β blocker to reduce total coronary flow is opposed by nitrate.
- 36. Heart failure • Exc. SNS Cardiac remodeling by :- 1. Tachycardia (β1 receptors) ↑ MOD 2. RAAS 3. Chr. Stim. of cardiac β rec. myocyte hypertrophy & apoptosis Cardiac dilatation & ventricular wall thinning 4. ↑ cardiac cytokines (TNF α & Ils) induce myocyte hypertrophy and apoptosis Fibrosis & ventricular wall stiffness. • β bl. ↓ exc. Sympath. Stimul. of heart (Mild to severe HF caused by LV systolic dysfunction)
- 37. Rationale in Heart failure (early) 1. Inhibition of the sympathetic stimulation of myocardium and cardiac remodelling 2. Suppression of the RAAS activation by decreasing the release of renin from renal juxtaglomerular cells 3. attenuation of oxidative stress and inflammation in myocardium.
- 38. • Carvedilol β1,β2, α1 (vd); antioxidant, antiinflmmatory and antiapoptotic (multiple-action neuroendocrine antagonist). • Given in symptomatic HF without hypotension, pulmonary congestion, or AV block. • A/E Bradycardia, worsening heart failure, and dizziness or light headedness (vd & ↓ BP) • Started on low doses & then gradually ↑ (beneficial effects have a delayed onset of action & a/e occur immediately) • Also, can lead to ↑ symptoms for 4 to 10 weeks before any improvement is noted
- 40. Arrhythmias • The Class II antiarrhythmics are β-adrenoceptor antagonists (β-blockers) such as esmolol, metoprolol, and propranolol. • Prevent & treat SVA* & ↓ ventricular ectopic depol. and sudden death in patients with MI • Antiarrhythmic effects Inhibit sympathetic activation of cardiac automaticity and conduction (↓ HR, ↓ AVN conduction velocity & ↑ AVN refractory period) SVA Supraventricular arrhythmias
- 41. • Esmolol Acute SVT/HTN during or immediately after surgery • Metoprolol & Propranolol SVA & VA
- 42. Synopsis of β blockers • Uses, A/E, C/I and drug interactions of non- selective β blockers (Propranolol prototype) • Uses of partial agonists & other non-selective agents • Uses of cardioselective β blockers • Uses of 3rd generation β blockers • Dosage forms & strengths of commonly used β blockers
- 43. Uses of Propranolol (THAPPAD) 1. Thyrotoxicosis & Tremors 2. HTN, HOCM, HF (Compensated) 3. Angina & Acute MI 4. Prophylaxis of migraine 5. Phaeochromocytoma (α blockers) 6. Anxiety & Arrhythmias 7. Dissecting aortic aneurysm 8. Digitalis toxicity
- 44. A/E of Propranolol (BBC Loses Viewers in Rochedale) • Bradycardia • Bronchoconstriction • Claudication • Lipids (LDL & TG ↑; HDL ↓) • Vivid dreams & nightmares • Negative ionotropic action • Reduced sensitivity to hypoglycemia • Tiredness & ↓ exercise capacity • Cold hands and feet, worsening of PVD
- 45. Contraindications of Propranolol • Don’t Prescribe Him Propranolol 1. Diabetes mellitus 2. Pulmonary diseases (Asthma, COPD) 3. Heart block, bradycardia 4. Prinzmetal’s angina 5. Peripheral vascular disease
- 47. Interactions 1. Additive depression of SAN & AV conduction with digitalis and verapamil cardiac arrest 2. Propranolol delays recovery from hypoglycaemia due to insulin and oral anti diabetics. 3. Phenylephrine, ephedrine in cold remedies ↑ BP 4. Indomethacin & other NSAIDs Attenuate anti- HTN action of β blockers. 5. Ppnl retards lidocaine metabolism 6. ↑ bioavailability of chlorpromazine by ↓ FPM
- 48. Partial agonistic (ISA) action • Exhibited by Pindolol, Carteolol, Celiprolol and acebutolol • Benefits are :- 1. Preferred in those prone to severe bradycardia (elderly patients; sick sinus) or with low cardiac reserve 2. Withdrawal less likely to exacerbate HTN/angina 3. Plasma lipid profile is not/less worsened.
- 49. Uses of other beta blockers 1. Pindolol HTN 2. Nadolol HTN, angina & prevent migraine, BOV 3. Timolol HTN, acute MI, glaucoma & prevent migraine 4. Levobunolol Glaucoma 5. Carteolol Glaucoma
- 51. Uses of cardioselective β blockers • Acebutolol HTN and cardiac arrhythmias • Atenolol HTN, angina & acute MI • Esmolol HTN & acute SVT during surgery • Metoprolol HTN, angina & acute MI • Bisoprolol HTN • Betaxolol HTN & POAG
- 52. α- and β-adrenoceptor antag. • Carvedilol (β1,β2,α1) & has antioxidant activity:- 1. Inhibition of lipid peroxidation in myocardial membranes 2. Anti-oxidant (scavenging of free radicals) 3. Inhibition of neutrophil release of O2 4. Antiapoptotic properties (prevent myocyte death and reduce infarct size in persons with myocardial ischemia and Systolic HF) • Carvedilol is also known as “third-generation β- blocker and neurohumoral antagonist,” (HTN, AMI, HF)
- 54. • Labetalol (β1,β2,α1 blocker) HTN emergencies (i.v.) • Nebivolol is a novel β1-selective antagonist 1. Promotes vasodilation via NO release from endothelial cells 2. Activates cardiac β3‐adrenergic receptors (protective mechanism against heart failure and myocardial ischemia–reperfusion injury)
- 55. Dosage forms & strengths • Atenolol (Tenormin): Oral, 25, 50, and 100mg tablets • Bisoprolol (Zebeta): Oral, 5 and 10mg tablets • Carvedilol (Coreg): Oral, 3.125, 6.25, 12.5, and 25mg tablets • esmolol (Brevibloc): Intravenous, 10ml (10mg/ml) vials • labetalol (Normodyne, Trandate): Oral, 100, 200, and 300mg tablets; 5 mg/ml in 20 and 40 ml vials • metoprolol (lopressor, Toprol): Oral, 50 and 100mg tablets (metoprolol tartrate); 25, 50, 100, and 200mg extended‐release tablets (metoprolol succinate) • Nebivolol (Bystolic): Oral, 2.5, 5, 10, and 20mg tablets • Propranolol (Inderal): Oral, 10, 20, 40, 60, and 80mg tablets; 60, 80, 120, and 160 mg capsules (extended release); intravenous, 1mg/ml in 1 ml vials
- 56. Thank you Old man (Mr . Propranolol) needs to change his glasses !!, he can read the large β Letters but he cant get a clear vision of their numbers Business man (Mr. Atenolol) Very hardworking. He focuses all the time on his One and only target ( β1 selective ) Mr. carvidilol is young but he is far from the Flying Betas so he cant recognize their types ( Non selective). Also, Mr. Carvidilol likes to blow red cylindrical Gum .. this reminds you of something ? Blood vessels
Notes de l'éditeur
- β1-selective antagonists (β1 > β2)—acebutolol (partial agonist), atenolol, betaxolol, esmolol, metoprolol Selective antagonists mostly go from A to M (β1 with 1st half of alphabet) Nonselective antagonists (β1 = β2)—nadolol, pindolol (partial agonist), propranolol, timolol Nonselective antagonists mostly go from N to Z (β2 with 2nd half of alphabet) Nonselective α- and β-antagonists—carvedilol, labetalol Nonselective α- and β-antagonists have modified suffixes (instead of “-olol”); Nebivolol b1 + b3 (which activate nitric oxide synthase in the vasculature)
- pindolol and propranolol exhibit membrane stabilizing activity, or local anesthetic activity, nadolol and timolol do not.
- The physiological processes mediated by adrenergic receptor signaling. As depicted, activation of adrenergic receptors by epinephrine (epi) and norepinephrine (Ne) not only directly impacts the cardiovascular system but also affects other organs/systems and diverse metabolic pathways.
- A few members of this group, used only for experimental purposes, bind irreversibly to β receptors.
- carvedilol (a non-selective β-adrenoceptor antagonist with additional α1-blocking activity) and nebivolol (a β1-selective antagonist that also causes vasodilatation by inducing endothelial nitric oxide production; 1. Receptor selectivity—Nadolol, propranolol, and timolol are typical nonselective β blockers. Labetalol and carvedilol have combined α- and β-blocking actions. These drugs are optically active, and different isomers have α- or β-blocking action. Nebivolol has vasodilating action in addition to β1-selective antagonism. 2. Partial agonist activity—Partial agonist activity (“intrinsic sympathomimetic activity”) may be an advantage in treating patients with asthma because these drugs (eg, pindolol, acebutolol)—at least in theory—are less likely to cause bronchospasm. In contrast, full antagonists such as propranolol are more likely to cause severe bronchospasm in patients with airway disease. 3. Local anesthetic activity—Local anesthetic activity (“membrane-stabilizing activity”) is a disadvantage when β blockers are used topically in the eye because it decreases protective reflexes and increases the risk of corneal ulceration. Local anesthetic effects are absent from timolol and several other β blockers that are useful in glaucoma.
- (-ve chronotropic, inotropic, and dromotropic effect.Because the β-blockers reduce cardiac output and blood pressure (see Fig. 9-2), they can be used to treat arterial hypertension. Heart ↓ sympathetic stimulation Kidneys ↓ renin from JG cells Eye ↓ aqueous humor secretion & i.o.p. Blockade of β2 receptors Lungs Bronchoconstriction Liver - Inh. E stimulated glycogenolysis ↓ hepatic glucose output from liver Also mask some of the early signs of hypoglycemia (e.g., tachycardia and sweating) in diabetic patients
- Less interference with carbohydrate metabolism and less inhibition of glycogenolysis during hypoglycaemia—safer in diabetics. However, tachycardia in response to hypoglycaemia is blocked
- The β-adrenoceptor antagonists are structural analogues of β-adrenoceptor agonists
- aMinor component normally but may become significant in heart failure.
- do not usually cause hypotension in healthy individuals with normal blood pressure. In vascular system, β2 blockade ↑ SVR from unopposed α-receptor–mediated effects as the sympathetic nervous system discharges in response to lowered blood pressure due to the fall in cardiac output. Nonselective and β1-blocking drugs antagonize the release of renin caused by the sympathetic nervous system.
- The baroreceptor reflx. A, Increased arterial pressure activates stretch receptors in the aortic arch and carotid sinus. B, Receptor activation initiates afferent impulses to the brain stem vasomotor center (VMC). C, Via solitary tract fiers, the VMC activates the vagal motor nucleus, which increases vagal (parasympathetic) outflw and slows the heart. At the same time, the VMC reduces stimulation of spinal intermediolateral neurons that activate sympathetic preganglionic fibers, and this decreases sympathetic stimulation of the heart and blood vessels. By this mechanism, drugs that increase blood pressure produce reflex bradycardia. Drugs that reduce blood pressure attenuate this response and cause reflex tachycardia.
- pharmacological effects of β‐blockers on the cardiovascular system. The beneficial cardiovascular outcomes of β‐blockers are primarily attributed to (i) decreased heart rate, contractility, and conduction; (ii) vasodilation; and (iii) inhibition of the renin–angiotensin– aldosterone system (RAAS). Notably, the third‐generation β‐blockers also possess other novel activities, especially augmentation of nitric oxide (NO) bioavailability. These effects collectively contribute to decreased blood pressure, reduced myocardial oxygen demand, attenuated water and salt retention, inhibition of oxidative and inflammatory stress, and retardation of cardiovascular pathogenic remodeling. here, the term remodeling refers to alterations in the structure and morphology of the cardiovascular tissues in response to hemodynamic load and/or tissue injury in association with neurohormonal activation, especially activation of the RAAS. Cardiovascular remodeling can be physiological (adaptive) or pathological (maladaptive) in nature. Cardiovascular pathological remodeling is an important mechanism of cardiovascular degeneration under disease conditions, including hypertension, myocardial infarction, and heart failure
- The effect in an anesthetized dog of the injection of epinephrine before and after propranolol. In the presence of a β-receptor–blocking agent, epinephrine no longer augments the force of contraction (measured by a strain gauge attached to the ventricular wall) nor increases cardiac rate. Blood pressure is still elevated by epinephrine because vasoconstriction is not blocked.
- Blockade of the β2 receptors in bronchial smooth muscle may lead to an increase in airway resistance, particularly in patients with asthma. Beta 1-receptor antagonists such as metoprolol and atenolol may have some advantage over nonselective β antagonists when blockade of β1 receptors in the heart is desired and β2-receptor blockade is undesirable. However, no currently available β1- selective antagonist is sufficiently specific to completely avoid interactions with β2 adrenoceptors. Consequently, these drugs should generally be avoided in patients with asthma. On the other hand, many patients with chronic obstructive pulmonary disease (COPD) may tolerate these drugs quite well and the benefits, for example in patients with concomitant ischemic heart disease, may outweigh the risks. COPD patients are at greater risk of ischaemic heart disease than asthmatics, so would benefit from the use of BBs. The results indicate that MI patients with COPD may benefit from b-blockers.
- inhibition of peripheral conversion of thyroxine to triiodothyronine hyperthyroidism Since sympathetic activity may enhance skeletal muscle tremor, it is not surprising that β antagonists have been found to reduce certain tremors. diminish portal vein pressure in patients with cirrhosis
- The sympathetic flow and drug targeting. As illustrated, there are four categories of drugs that inhibit the sympathetic activity: centrally acting sympatholytics inhibit central sympathetic discharge by activating α2‐adrenergic receptors in the brainstem, thereby leading to decreased sympathetic flow to the peripheral tissues and organs; ganglionic blocking agents block the neurotransmission in the ganglia; neuronal blocking agents block the synthesis, storage, or release of norepinephrine from the sympathetic postganglionic nerve terminal; and adrenergic receptor antagonists block α‐ and β‐adrenergic receptors or both located primarily on the membranes of the effector cells. Ach and Ne denote acetylcholine and norepinephrine, respectively.
- FIGURE 10-1. Physiologic control of blood pressure and sites of drug action. Blood pressure is the product of cardiac output and peripheral vascular resistance (PVR). These parameters are regulated on a systemic level by the sympathetic nervous system and the kidneys. Antihypertensive drugs act to suppress excessive sympathetic activity and modify renal function to counteract the mechanisms responsible for hypertension. Sites of action of the following drugs are shown: 1, vasodilators; 2, β-adrenoceptor antagonists ( β-blockers); 3, α-adrenoceptor antagonists ( α-blockers); 4, angiotensin receptor antagonists; 5, centrally acting sympatholytics; 6, angiotensin-converting enzyme (ACE) inhibitors; and 7, diuretics. The vasodilators, sympatholytic drugs, and angiotensin inhibitors reduce PVR; β-adrenoceptor blockers reduce cardiac output; and diuretics promote sodium excretion and reduce blood volume.
- The α1-blockers reduce peripheral vascular resistance, whereas β1-blockers can cause a slight increase in peripheral resistance as a result of reflex vasoconstriction
- The β1-blockers reduce cardiac output, whereas the α 1-blockers can increase cardiac output by decreasing cardiac afterload and aortic impedance to ventricular ejection of blood.
- Both α1-blockers and β1-blockers reduce mean arterial blood pressure.
- β‐blockers with vasodilating effects, including carvedilol and nebivolol, but not the traditional β‐blocker atenolol, should be considered whenever β‐blockers are indicated in hypertensive patients.
- Systolic BP > 220 or diastolic BP > 120 mm Hg with evidence of active end organ damage (encephalopathy or intracranial haemorrhage) is labelled ‘hypertensive emergency’, while the same elevation of BP without overt signs of endorgan damage is termed ‘hypertensive urgency’.
- 3 FDA approved beta blockers Labetalol, carvedilol, and metoprolol
- Metoprolol and bisoprolol have also been shown to produce benefiial effects in patients with heart failure. Some studies, however, suggest that these drugs are not as benefiial as carvedilol in some patients with heart failure. In the Carvedilol or Metoprolol European Trial (COMET). of patients with heart failure, carvedilol reduced mortality more than did metoprolol. This study has been criticized with respect to whether the doses of the βblockers used in the study produced the same degree of βblockade.
- VA VT, VF, PVC; SVA SVT/PSVT, AF, WPW, PAC, Aflutter; VA is more dangerous
- HOCM Subaortic region is hypertrophic. reducing left ventricular outflow obstruction TT Propranolol rapidly controls the sympathetic symptoms (palpitation, nervousness, tremor, fixed stare, severe myopathy and sweating) without significantly affecting thyroid status. It also inhibits peripheral conversion of T4 to T3 and is highly valuable during thyroid storm. Major use, however, is preoperatively and while awaiting response to antithyroid drugs/radioactive iodine. PC β blockers may be used to control tachycardia and arrhythmia, but should never be administered unless an α blocker has been given before, otherwise dangerous rise in BP can occur. They suppress cardiomyopathy caused by excess CAs. Pheochromocytoma is sometimes treated with combined α- and β-blocking agents (eg, labetalol), Diss. Aa blockers help by reducing cardiac contractile force and aortic pulsation. HF metoprolol, bisoprolol, nebivolol, carvedilol. The benefit may result from antagonism of deleterious effects of sympathetic overactivity (invoked reflexly by heart failure) on myocardium. Overactivation of cardiac β1 receptors has been found to exert toxic effects on the heart by accelerating myocyte apoptosis and promoting functionally unfavourable remodeling. Myocardial infarction (MI) In relation to MI, β blockers have been used for two purposes: (a) Secondary prophylaxis of MI: There is now firm evidence of benefit. Long-term use after recovery from MI has been found to decrease subsequent mortality by 20%. They may act by: (i) Preventing reinfarction (ii) Preventing sudden ventricular fibrillation at the subsequent attack of MI. High risk patients (those who had large infarcts) should be put on β blockers (if there are no haemodynamic contraindications) for at least 2 years. β blockers with partial agonistic action are less suitable for this purpose. (b) Myocardial salvage during evolution of MI: Administered i.v. within 4–6 hours of an attack followed by continued oral therapy. β blockers — (i) May limit infarct size by reducing O2 consumption—marginal tissue which is partially ischaemic may survive. (ii) May prevent arrhythmias including ventricular fibrillation. 3. Cardiac arrhythmias β blockers (mainly propranolol) suppress extrasystoles and tachycardias, especially those mediated adrenergically (during anaesthesia, digitalis induced)—may be used i.v. for this purpose. Propranolol controls ventricular rate in atrial fibrillation and flutter, but only occasionally restores sinus rhythm. Esmolol is an alternative drug for paroxysmal supraventricular tachycardia
- Cardioselective β blockers and those with intrinsic sympathomimetic activity have little/no deleterious effect on blood lipids. Withdrawal of propranolol after chronic use should be gradual, otherwise rebound hypertension, worsening of angina and even sudden death can occur. This is due to supersensitivity of β receptors occurring as a result of long-term reduction in agonist stimulation. Tiredness and reduced exercise capacity: due to blunting of β2 mediated increase in blood flow to the exercising muscles as well as attenuation of glycogenolysis and lipolysis. Cold hands and feet, worsening of peripheral vascular disease are noticed due to blockade of vasodilator β2 receptors.
- Regulation of vascular smooth muscle contraction. Vascular smooth muscle contraction occurs when calcium (Ca2 +) enters smooth muscle via L-type calcium channels, binds to calmodulin, and activates myosin light-chain kinase. This leads to formation of myosin phosphate, which interacts with actin to cause muscle contraction. Calcium inflx is inhibited by CCBs, leading to muscle relaxation. Organic nitrates release nitric oxide, which activates guanylyl cyclase and increases formation of cyclic guanosine monophosphate (cGMP). Investigators believe that cGMP causes smooth muscle relaxation by activating kinases that increase myosin phosphatase activity and decrease myosin phosphate levels. α1-Adrenoceptor agonists activate phospholipase C (PLC), which increases formation of inositol triphosphate (IP3) from phosphatidylinositol bisphosphate (PIP2), leading to increased release of calcium from the sarcoplasmic reticulum. β2-Adrenoceptor agonists increase formation of cyclic adenosine monophosphate (cAMP), which activates kinases that inhibit myosin light-chain kinase.
- 1. However, propranolol has been safely used with nifedipine. Warning signs of hypoglycaemia mediated through sympathetic stimulation (tachycardia, tremor) are suppressed. In some cases BP rises due to unopposed α action of released Adr.
- These drugs themselves activate β1 and/or β2 receptors submaximally. The benefits of this property are controversial. 1. Bradycardia and depression of contractility at rest are not prominent, but exercise tachycardia is blocked; may be preferred in those prone to severe bradycardia (elderly patients; sick sinus) or with low cardiac reserve. 2. Withdrawal is less likely to exacerbate hypertension or angina; continued agonistic action on β receptors (of the drug itself) prevents development of supersensitivity. 3. Plasma lipid profile is not/less worsened. 4. Not effective in migraine prophylaxis—they dilate cerebral vessels. 5. Not suitable for secondary prophylaxis of MI.
- This effect is observed when the patient is resting and sympathetic tone is low, and it can result in a smaller reduction in heart rate than that caused by β-blockers without intrinsic sympathomimetic activity. When sympathetic tone is high, pindolol acts as a competitive receptor antagonist to inhibit sympathetic stimulation of the heart in the same manner as other β-blockers. Pindolol is approved only to treat hypertension. This means that, apart from blocking β1‐ and β2‐adrenergic receptors, it produces some stimulation. pindolol therefore only slightly influences normal sympathetic drive at rest but effectively reduces the effects of elevated sympathetic activity. at low therapeutic doses, selective β1‐blockers do not generally cause bronchoconstriction. however, as doses increase, they may also block β2‐receptors, and as such, they should be used with caution in patients with asthma or COpD. Although pindolol and propranolol exhibit membranestabilizing activity, or local anesthetic activity, nadolol and timolol do not. Drugs with local anesthetic activity can block sodium channels in nerves and heart tissue and thereby slow conduction velocity.
- reduce aqueous humor secretion and intraocular pressure. Timolol was selected for ophthalmic use partly because it does not have membranestabilizing activity and therefore does not anesthetize the cornea when instilled into the eye. Nadolol is also efficacious in the prevention of bleeding from esophageal varices in patients with cirrhosis. It is pharmacologically attractive for this indication because it has a long half-life, allowing once-daily administration, and, because the drug is excreted primarily by renal elimination without hepatic metabolism, no dosing adjustments are needed on account of hepatic insufficiency. Penbutolol is an additional drug in this class. An ocular formulation of timolol is used in the treatment of glaucoma; even when administered to the eye, systemic absorption of the drug may be suffi ciently high to cause adverse effects in susceptible patients. Levobunolol and carteolol are additional nonselective -blockers that are indicated for administration via eye drops in the treatment of glaucoma.
- partial agonists inhibit the activation of β receptors in the presence of high catecholamine concentrations but moderately activate the receptors in the absence of endogenous agonists. Finally, evidence suggests that some β blockers (eg, betaxolol, metoprolol) are inverse agonists— drugs that reduce constitutive activity of β receptors—in some tissues. Pure antagonists; that is, the occupancy of a β receptor by such a drug causes no activation of the receptor.
- Atenolol shows less variability in its oral absorption than do other β-blockers and is excreted largely unchanged in the urine. It also has lower lipid solubility and has been associated with a lower incidence of central nervous system side effects (e.g., vivid dreams, tiredness, and depression). Atenolol is administered orally or parenterally and is primarily used to treat hypertension, angina pectoris, and acute myocardial infarction. Esmolol has a much shorter half-life than otherβ-blockers and is administered intravenously to treat hypertension and acute supraventricular tachycardia when these occur during surgery. Esmolol is rapidly metabolized to inactive compounds by plasma esterase enzymes. Metoprolol is used to treat hypertension, angina pectoris, and acute myocardial infarction. It can be administered
- Carvedilol & Labetalol Both are b1,b2 & a1 (both used in HTN). Blockage of α1‐adrenergic receptors causes vasodilation, thereby lowering blood pressure. Decreased blood pressure potentially results in reflex tachycardia. Importantly, blockage of cardiac β1‐adrenergic receptors by these drugs suppresses reflex tachycardia caused by α1 blockage.
- The baroreceptor reflx. A, Increased arterial pressure activates stretch receptors in the aortic arch and carotid sinus. B, Receptor activation initiates afferent impulses to the brain stem vasomotor center (VMC). C, Via solitary tract fiers, the VMC activates the vagal motor nucleus, which increases vagal (parasympathetic) outflw and slows the heart. At the same time, the VMC reduces stimulation of spinal intermediolateral neurons that activate sympathetic preganglionic fibers, and this decreases sympathetic stimulation of the heart and blood vessels. By this mechanism, drugs that increase blood pressure produce reflex bradycardia. Drugs that reduce blood pressure attenuate this response and cause reflex tachycardia.