TYPHOID FEVER
•Télécharger en tant que PPTX, PDF•
99 j'aime•70,429 vues

TYPHOID FEVER

Recommandé
Contenu connexe
Tendances
Similaire à TYPHOID FEVER
Similaire à TYPHOID FEVER (20)
Plus de MAHESWARI JAIKUMAR
Plus de MAHESWARI JAIKUMAR (20)
Dernier
Dernier (20)
TYPHOID FEVER
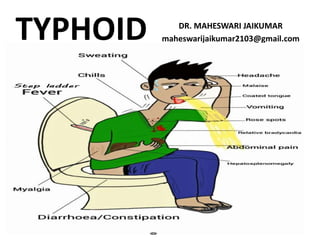
- 1. TYPHOID DR. MAHESWARI JAIKUMAR maheswarijaikumar2103@gmail.com
- 2. TYPHOID • Typhoid fever is due to systemic infection mainly by Salmonella typhi • Salmonella typhi infection is found only in men
- 3. • The disease is clinically characterized by a typical continuous fever for 2-3 weeks, with relative bradycardia with involvement of lymphoid tissues and considerable constitutional symptoms
- 4. • The term “ENTERIC FEVER” includes both typhoid and para typhoid fevers • The disease may occur sporadically, epidemically or endemically
- 5. EPIDEMIOLOGICAL DETERMINANTS • AGENT: 1.Salmonella typhi is the major cause of entric fever 2. S.para A & S.para B are relatively infrequent
- 8. • S.typhi has three main antigens : O, H & Vi and a number of phage types • S.typhi survives intra cellularly in the tissues of various organs
- 9. • It is readily killed by drying, pasteurization and common disinfectants • The factors which influence the onset of typhoid fever in man are the infecting dose and virulence of the organism
- 10. • RESERVOIR OF INFECTION: Man is the only known reservoir of infection (via cases & carriers) • CASES: A case is infectious as long as bacilli appears in stools or urine
- 11. • CARRIERS: The carriers may be temporary (incubatory, convalescent) or chronic • Convalescent carriers excrete bacilli for 6-8 weeks (after which their numbers diminish rapidly by the end of three months)
- 12. • Persons who excrete bacilli for more than one year are after clinical attack are called chronic carriers
- 13. • In most chronic carriers the bacilli exists in gall bladder and in the billiary tract. A chronic carrier may excrete the bacili for several years (may be as long as 50 years)
- 14. • A famous case of “Typhoid Mary” who gave raise to 1300 cases in her life time is an example for a chronic carrier state • Faecal carriers are more common than urinary carriers
- 16. SOURCE OF INFECTION • The primary sources of infection are faeces and urine of cases or carriers • The secondary sources include contaminated water, food, fingers and flies
- 17. HOST FACTORS • AGE: Typhoid fever may occur at any age • GENDER: Males are more affected than females
- 18. • IMMUNITY: All ages are susceptible to infection • The host factors that contributes to resistance to the bacilli are gastric acidity & local intestinal immunity
- 19. ENVIRONMENTAL & SOCIAL FACTORS • Enteric fevers are observed all throughout the year • The peak incidence is reported during July-September
- 20. • Vegetables grown in sewage farmlands or washed in contaminated water are positive health hazard
- 21. • Typhoid bacilli grow rapidly in milk without altering in taste or appearance in anyway, in which case ingestion of such raw milk poses a threat to the consumer
- 22. • These factors are compounded by such social factors as pollution of drinking water supplies, open air defecation and urination, low standards of food and personal hygiene and health ignorance
- 23. • Therefore typhoid fever may be regarded as an index of general sanitation in any country
- 24. INCUBATION PERIOD • Usually 10-14 days • But the it can be as short as 3 days or as long as 3 weeks, depending on the dose of bacilli ingested
- 25. MODE OF TRANSMISSION • Typhoid fever is transmitted via the faecal-oral route or urine- oral routes
- 26. • This may take place directly through soiled hands contaminated with faeces or urine of cases or carriers or indirectly by the ingestion of contaminated water, milk, food or through flies
- 28. CLINICAL FEATURES • The onset is insidious, but in children may be abrupt with chills and high fever
- 29. • During the prodromal stage , there is malaise, headache, cough and sore throat often with abdominal pain and constipation • The fever ascends in step ladder fashion
- 30. • After about 7-10 days, the fever reaches a plateau and the patient looks toxic appearing exhausted and often prostrated • There may be marked constipation, especially in the early stages or “pea soup diarrhoea”
- 31. • There is marked abdominal distension • There is leukopenia and blood, urine and stool culture is positive for salmonella
- 32. • If there are no complications the patient’s condition improves over 7-10 days • However relapse may occur for up to 2 weeks after termination of therapy
- 33. • During early phase, physical findings are few • Later splenomegaly, abdominal distension and tenderness, relative bradycardia, dicrotic pulse and ocassionaly meningsmus appear
- 34. • The rash (rose spots)commonly appear during the second week of the disease • The individual spot , found principally on the trunk, is a pink papule 2-3 mm in diameter that fades on pressure. It disappears in in 3-4 days
- 35. ROSE SPOTS
- 36. • Serious complication occur in up to 10 percent of patients (especially those who have been ill for longer than 2 weeks and who have not received proper treatment)
- 37. • Intestinal haemorrhage is manifested by a sudden drop in temperature and signs of shock, followed by dark or fresh blood in the stool • Intestinal perforation is most likely to occur during the third week
- 38. • Less frequent complications are urinary retention, pneumonia, thrombophlebitis, myocarditis, psychosis, cholecystitis, nephritis and oeteomyelitis
- 39. LABORATORY DIAGNOSIS • MICROBIOLOGICAL PROCEDURES The definitive diagnosis of typhoid fever depends on the isolation of the bacilli from blood, bone marrow and stools. Blood culture is the mainstay of diagnosis of this disease
- 40. SEROLOGICAL PROCEDURE • Felix-Widal test measures agglutinating antibody levels against O & H antigens • Usually “O” antibodies appear on day 6-8 and “H” antibodies on day 10-12 after the onset of disease
- 41. • The test is usually performed on an acute serum (at first contact with the patient) • The test has moderate sensitivity and specificity
- 42. • It can be negative up to 30% of culture – proven case of typhoid fever • This may be because of prior antibiotic therapy, that has blunted the antibody response
- 43. NEW DIAGNOSTIC TESTS • The IDL tubex test can detect specific IgM antibodies in samples to S. Typhi liposaccharide (LPS) antigen and the staining of bound antibodies by anti-human IgM antibody conjugated to colloidal dye particles
- 45. CONTROL OF TYPHOID FEVER • The control or elimination of the typhoid fever is well within the scope of modern public health
- 46. • There are generally three lines of defence against typhoid fever: • 1. Control of reservoir • 2. Control of sanitation • 3. Immunization
- 47. CONTROL OF RESERVOIR • The usual methods of control of reservoir are their identification, isolation, treatment & disinfection
- 48. • CASES: EARLY DIAGNOSIS –This is of vital importance as the early symptoms are non-specific • Culture of blood and stools are important investigations in the diagnosis of cases
- 49. NOTIFICATION: Notification must be done in areas where it is mandatory ISOLATION: Since typhoid is an infectious disease the cases are to be transferred to hospital
- 50. • As a rule cases should be isolated till three bacteriologically negative stools and urine reports are obtained on three separate days
- 51. TREATMENT • Flouroquinolones are widely regarded as the drug of choice for the treatment of of typhoid fever
- 52. TREATMENT
- 53. • They are relatively inexpensive and well tolerated and more reliably and effectively than chloremphenicol, ampicillin, amoxicillin, and trimethoprim & sulphamethoxazole
- 54. • Patients seriously ill and profoundly toxic should be given Inj of hydrocortisone 100 mg daily for 3-4 days • DISINFECTION: stools and urine are the sole sources f infection. They should be received in in closed containers and disinfected with 5% cresol for at least 2 hours
- 55. • All soiled clothes and linen should be soaked in a solution of 2% chlorine and be stream sterilized • Doctors and nurses should disinfect their hands
- 56. FOLLOW UP • Examination of stools and urine should be should be done for S.typhi 3-4 months after discharge and again 12 months to prevent development of carrier state
- 57. CARRIERS: • Since carriers are the ultimate source of infection, their identification and treatment is one of the most radical ways of controlling typhoid fever • The following are the measures recommended:
- 58. • IDENTIFICATION: Carriers are identified by cultural and serological examinations. Duodenal drainage establishes the presence of salmonella in the biliary tract of carriers • The antibodies are present in about 80% of chronic carriers
- 59. TREATMENT OF CARRIERS: • The carriers should be given an intensive course of ampicillin or amoxycillin (4-6 g a day) together with probenecid (2g/day) for 6 weeks
- 61. • These drugs are concentrated in the bile and may achieve eradication • Chloromycetin is considered worthless for clearing the carrier state
- 62. SUREGERY • Cholecyctectomy with concomitant ampicillin therapy has been regarded as the most successful approach to the treatment of carriers
- 63. • Urinary carriers are eassy to treat, but refractory cases may need nephrectomy when one kidney is damaged and the other is healthy • SURVEILLANCE: The carriers should be kept under surveillance. They should be prevented from handling food, milk or water for others
- 64. HEALTH EDUCATION • Health education regarding washing of hands with soap after defecations or urination and before preparing food is an essential element
- 65. • In short, the management of carriers continues to be an unsolved problem • This is the crux of the problem, in the elimination of typhoid
- 66. CONTROL OF SANITATION • Protection and purification of drinking water supplies, improvement of basic sanitation and promotion of food hygiene are essential measures to interrupt transmission of typhoid fever
- 67. IMMUNIZATION • Immunization is a complimentary approach in the prevention of typhoid • It yields the highest benefit to the money spent
- 68. • Immunization against typhoid does not give 100% protection, but it definitely lowers both the incidence and seriousness of the infection • It can be given at any age upwards 2 years
- 69. • Immunization is recommended to those who live in endemic areas, house hold contacts and groups at risk of infection such as school children and hospital staff, travellers proceeding to endemic areas and those attending melas and yatras
- 70. ANTI TYPHOID VACCINES • Two vaccines are available: 1. Vi polyssaccharide vaccine 2. The Type 21a vaccine
- 72. Vi POLYSSACCHARIDE VACCINE • The vaccine is composed of purified Vi capsular polysaccharide from the Ty2 S typhi strain and elicits a T-cell independent IgG response that is not boosted by additional doses
- 73. • The vaccine is administered sub cutaneously or intra muscularly . The target value of each single human dose is about 25 micro gram of antigen • The vaccine is stable for 6 months at 370 C and for 2 years at 220 C
- 74. • The recommended storage temperature is 2-8oC.The Vi vaccine does not elicit adequate immune responses in children aged less than 2 yrs • Only one dose is required and the vaccine confers protection after 7 days of vaccination
- 75. • To maintain protection revaccination is recommended every three years. • The vaccine can be co- administered with other vaccines (such as yellow fever, and hepatitis A and with routine childhood vaccinations)
- 76. • No serious adverse events and minimum of local effects are associated with Vi vaccination • There are no contra indications to the vaccine other than previous hypersensitivity reaction to vaccine components
- 77. THE TYPE 21a VACCINE • Is an orally administered live attenuated Ty2 strain of S.typhi. The lyophilized vaccine is available as enteric coated capsules
- 78. TYPE 21 a VACCINE
- 79. • The vaccine has to be stored at 2-80C, it retains potency for approximately 14 days at 250 C • The capsules are licensed for use in individuals aged above 5 yrs
- 80. • The vaccine is administered every other day (on 3 and 5 day) a 3-dose regimen is recommended • Protective immunity is achieved 7 days after the last dose
- 81. • The recommendation is to repeat the series every 3 years for people living in endemic areas and every year for individuals travelling from non endemic to endemic areas
- 84. THANK YOU